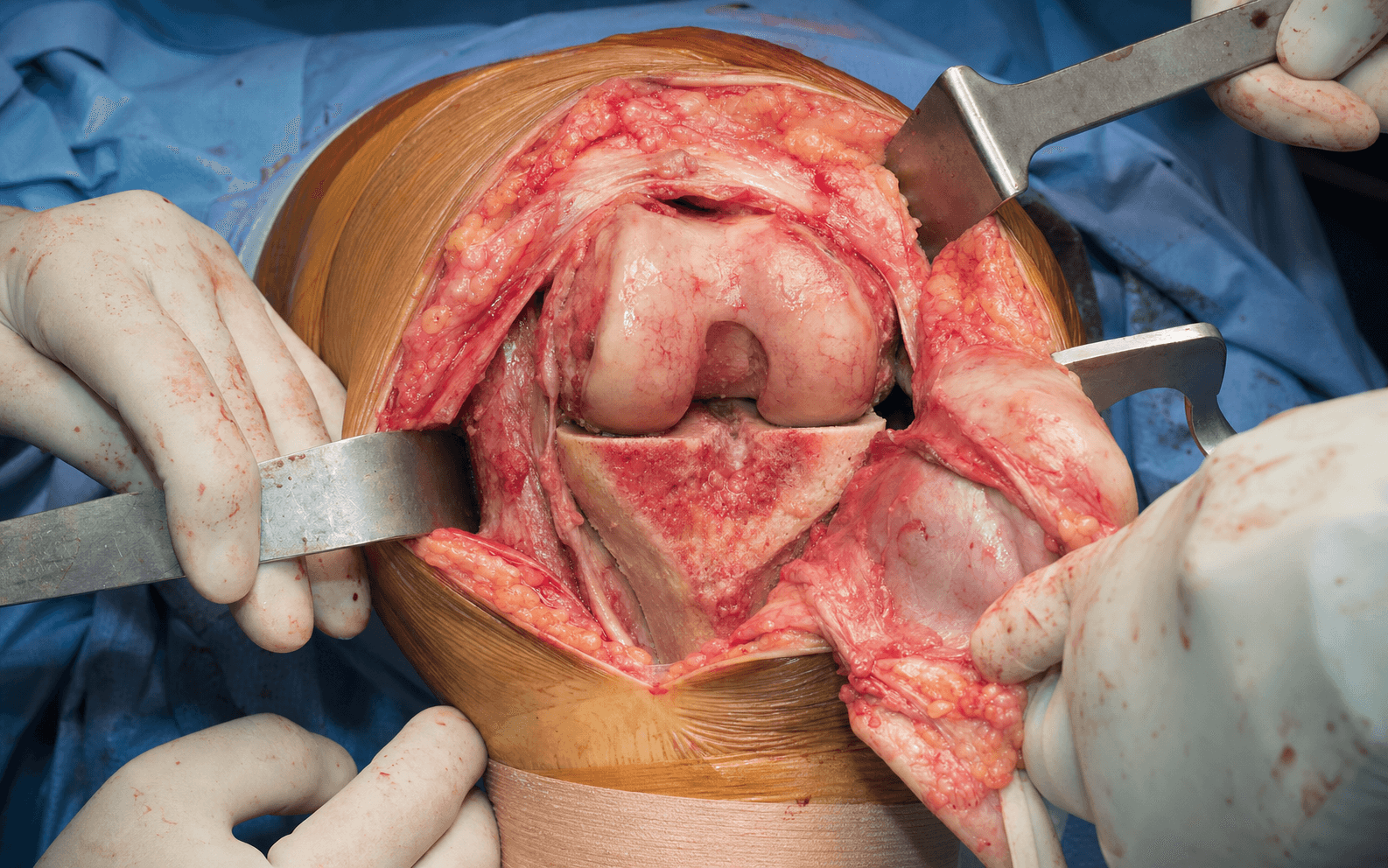
Medial parapatellar arthrotomy (gold standard approach) | advanced
- The medial parapatellar approach is the gold-standard exposure for primary TKA: incise 5mm medial to the patella to preserve the lateral blood supply (lateral genicular arteries), then evert the patella laterally.
- Femoral component rotation is set from three landmarks that must agree within 2 degrees — Whiteside's line (AP axis), the transepicondylar axis, and 3 degrees external rotation from the posterior condylar axis. Internal rotation is the leading cause of patellar maltracking and painful TKA.
- Gap balancing demands equal, rectangular flexion and extension gaps (roughly 10mm with 1-2mm symmetric laxity), assessed with spacer blocks at 0 and 90 degrees. Varus releases medially (deep MCL before superficial); valgus releases laterally with common peroneal nerve risk.
- Modern (third-generation) cement technique is the global default: pulsatile lavage, bone drying, pressurisation, cement on both bone and implant. Cemented fixation is the registry benchmark with roughly 90-93 percent all-cause survival at 15 years.
- “Be able to draw the rotational landmarks on a distal femur model and explain the 3 degrees external rotation rule from posterior condyles, confirming with Whiteside's line and the transepicondylar axis
- “Know the cross-registry survivorship message (NJR, AJRR, AOANJRR, NZJR, SHAR): cemented fixation remains the benchmark with roughly 90-93 percent all-cause survival at 15 years, and CR vs PS designs show broadly equivalent survivorship
- “Understand sequential soft tissue balancing: varus deformity requires medial release (deep MCL before superficial), valgus requires lateral release with peroneal nerve risk
- “Describe intraoperative patellar tracking assessment through full ROM - lateral maltracking indicates femoral component internal rotation requiring revision
When & Why
Indications. Symptomatic end-stage knee arthritis that has failed conservative management (activity modification, analgesia, physiotherapy, weight optimisation, intra-articular corticosteroid or viscosupplementation). The common disease categories are: - Primary osteoarthritis — the most common indication (about 85 percent of TKAs), typically tricompartmental disease with pain and functional limitation.
- Inflammatory arthritis — rheumatoid, psoriatic or ankylosing spondylitis with severe joint destruction.
- Post-traumatic arthritis — following tibial plateau, distal femur or patellar fracture with malunion or articular incongruity.
- Avascular necrosis — multifocal or involving multiple compartments.
- Failed osteotomy — progressive arthritis after high tibial or distal femoral osteotomy, or a failed unicompartmental knee arthroplasty progressing to multicompartmental disease.
- Secondary indications — septic arthritis sequelae (after eradication of infection), haemophilic arthropathy, and selected neuropathic (Charcot) joints with preserved sensation. Contraindications. Absolute: active infection (local or systemic — requires a two-stage revision if the knee is infected), an absent or irreparably disrupted extensor mechanism, severe peripheral vascular disease with an ischaemic leg needing vascular surgery first, and a neuropathic joint with complete sensory loss (unacceptably high failure rate). Relative (optimise first): age less than 60 with high activity demands (consider osteotomy), severe bone loss (may need stems, augments or a hinged prosthesis), morbid obesity (BMI greater than 40 — increases infection and wound complications), active smoking (cessation 6 weeks preoperatively), a poor soft-tissue envelope (prior incisions, skin grafts), and chronic pain syndromes such as CRPS. Assess the whole patient, not just the joint. Before committing, optimise modifiable risk: glycaemic control, smoking cessation, weight, skin integrity and any dental or urinary foci of infection. Mark all prior incisions — use the most lateral usable incision, or a new midline incision if existing incisions are more than 6cm apart, to protect the skin bridge and avoid necrosis. Consent specifically for infection (superficial 2-4 percent, deep 0.5-2 percent), stiffness and the possible need for manipulation under anaesthesia, venous thromboembolism (symptomatic VTE 2-5 percent, fatal PE 0.1-0.2 percent), peroneal nerve palsy (especially in valgus correction greater than 15 degrees), bleeding and transfusion, and the realistic expectation that a 60-year-old has roughly a 15 percent lifetime revision risk. Setup. Supine on a standard table with a foot support or side post that allows knee flexion beyond 120 degrees. Apply a sterile thigh tourniquet high on the thigh with adequate padding, exsanguinate by elevation for 2 minutes or an Esmarch bandage (avoid Esmarch with malignancy, infection or severe vascular disease), and inflate to 100mmHg above systolic (minimum 250, typically 300mmHg, maximum 350mmHg) — the lowest effective pressure is best, with a time limit of about 90 minutes.
The Operation
The goal is to resurface the arthritic femur, tibia and (selectively) patella through a medial parapatellar exposure, restore a neutral mechanical axis, set correct femoral rotation, balance symmetric rectangular flexion-extension gaps, and fix the components with modern cement technique. The exposure is the foundation — laid out in full below (and in depth on the medial parapatellar approach to the knee page).
Operative sequence
- Supine with a foot support or side post allowing flexion beyond 120 degrees, neutral hip rotation.
- Sterile thigh tourniquet high on the thigh, well padded; exsanguinate and inflate to 100mmHg above systolic (typically 300mmHg).
- Keep tourniquet time under 90 minutes; release before closure for hemostasis. Modern tourniquet-less TKA reduces pain and improves early ROM at the cost of more blood loss and operative time — offset by tranexamic acid.
- Mark the patella borders, tibial tubercle and joint line.
- A midline longitudinal incision from 5-6cm above the superior pole of the patella to 2cm below the tibial tubercle (12-15cm total). The midline vertical incision preserves both medial and lateral skin blood supply and is critical in revision where multiple incisions exist.
- Sharp incision through skin and subcutaneous tissue to deep fascia, keeping skin flaps thick to avoid necrosis; the infrapatellar branch of the saphenous nerve is usually sacrificed — counsel the patient about numbness.
- Incise the quadriceps tendon 5mm medial to midline, starting about 5cm proximal to the patella.
- Continue distally along the medial border of the patella, staying 5mm medial to its edge and incorporating the medial retinaculum, then curve distally at the inferior pole to the anteromedial tibial plateau, ending 5mm medial to the tibial tubercle at the joint line.
- Staying 5mm medial (not on the edge) preserves the patella's lateral blood supply — the lateral superior and inferior genicular arteries form the extraosseous ring that dominates patellar perfusion.
The patella is perfused predominantly from the lateral side via the genicular arterial ring. An arthrotomy placed too lateral, or an aggressive lateral release, devascularises the patella and risks AVN and fracture. Stay 5mm medial to the patellar edge to keep the lateral supply intact.
Patellar devascularisation if the arthrotomy is too lateral or the lateral release is excessive; damage to the patellar tendon if the incision drifts distally or medially onto the tendon substance.
- Subperiosteal elevation of the medial meniscus, capsule and deep MCL off the proximal tibia; release Hoffa's fat pad from the inferior pole and anterior tibia.
- Evert the patella laterally with gentle traction, displacing it onto the lateral femoral condyle.
- If the patella will not evert easily, STOP — forced eversion avulses the patellar tendon or fractures the patella. Instead extend the arthrotomy proximally into vastus lateralis (an inverted-V) or release the lateral retinaculum directly on bone, only the minimum needed (typically 2-3cm). Lateral release is a direct open extension, not percutaneous pie-crusting (which causes haematoma and risks the lateral genicular artery). It is needed in less than 10 percent of primary TKAs when femoral rotation is correct.
Forced eversion avulses the patellar tendon from the tibial tubercle or fractures the patella — both catastrophic and needing immediate repair with suture anchors, bone tunnels or tension-band wiring. Never force a patella that resists eversion; extend the arthrotomy or release the lateral retinaculum first.
- Excise the ACL from its femoral origin (lateral wall of the intercondylar notch) and tibial insertion; remove the anterior horns of both menisci.
- Clear soft tissue from the anterior tibia and distal femur with a periosteal elevator and electrocautery.
- Remove peripheral osteophytes from both femoral condyles, both tibial plateaus and the intercondylar region BEFORE the bone cuts — this creates space for the saw and prevents osteophyte impingement giving a false sense of balance. Clear both gutters completely. Stay on bone medially to protect the MCL; use curved osteotomes posteriorly to protect the popliteal artery.
- Apply an extramedullary or intramedullary tibial guide aligned to the mechanical axis (centre of ankle to centre of knee); set varus-valgus to 0 degrees.
- Set posterior slope to 3-7 degrees (typically 5 degrees, matching native slope which averages 7 degrees, range 0-13 — match within 2 degrees). Resect 8-10mm from the least-worn (lateral) plateau.
- Excessive slope (greater than 7 degrees) causes PCL impingement and flexion instability in CR knees and cam-post dislocation in PS knees; insufficient slope (less than 3 degrees) limits hyperextension and causes posterior cam-post impingement in PS knees.
The popliteal artery lies 10-15mm posterior to the capsule at the joint line. Complete the posterior tibial cut with an oscillating saw — never plunge. Curved osteotomes and a posterior retractor placed on bone protect the vessel during posterior osteophyte removal.
- Enter the femoral canal via the intercondylar notch, anterior to the PCL insertion; insert the intramedullary rod.
- Set the distal femoral cutting guide to 5-7 degrees valgus from the anatomic axis (typically 6 degrees) to give a cut perpendicular to the mechanical axis. Resect 9-10mm from the most worn condyle, measuring both.
- Excessive valgus (greater than 8 degrees) causes medial laxity; insufficient (less than 4 degrees) leaves residual varus and medial overload. Adjust for native alignment (more valgus cut in a native valgus knee). Fat embolism is rare with modern small-diameter rods.
- Insert a 10mm spacer block between the cuts with the knee in full extension; apply varus and valgus stress.
- Goal: symmetric 1-2mm laxity medially and laterally (a rectangular gap). Varus with medial tightness releases sequentially — deep MCL (meniscotibial ligament), then posterior capsule, then superficial MCL proximal fibres, then pes anserinus. Valgus with lateral tightness releases sequentially — ITB, lateral capsule, popliteus, LCL, lateral gastrocnemius head.
Valgus correction is harder and riskier than varus. Extensive lateral release (including the LCL for severe deformity) risks a common peroneal nerve palsy (2-5 percent when the deformity exceeds 15 degrees valgus). Limit acute correction, consider staged correction for deformity greater than 20 degrees, keep the knee flexed during closure to relax the nerve, and counsel the patient preoperatively. Consider a constrained implant if instability persists.
- Measure the AP dimension, choosing a size that neither notches anteriorly nor overhangs posteriorly (downsize if between sizes).
- Set rotation from THREE landmarks that should agree within 2 degrees: 1. Whiteside's line — the AP axis from the deepest trochlear groove to the intercondylar notch; the component should be parallel. 2. Transepicondylar axis — the line joining the epicondyles; the most anatomical reference but hard to palpate reliably. 3. 3 degrees external rotation from the posterior condylar axis — the most reliable single landmark (posterior condyles are easy to identify).
- If they conflict, use the combination — typically 3 degrees external to the posterior condyles, confirming parallel to Whiteside's line. The transepicondylar axis is especially valuable in valgus knees where the lateral condyle is hypoplastic and the posterior condylar axis is unreliable.
Femoral rotation is critical for patellar tracking and flexion-gap balance. Internal rotation causes lateral maltracking, anterior knee pain and flexion instability — the leading cause of painful TKA and revision for pain. Always mark all three landmarks and use the combination; never rely on one alone.
Internal rotation causes patellar maltracking, flexion instability and chronic pain requiring revision; excessive external rotation causes medial flexion laxity.
- Apply the 4-in-1 cutting block at the chosen size and rotation, secured with two pins; verify rotation visually against Whiteside's line and the transepicondylar axis.
- Make the anterior cut, then the posterior condylar cuts, then the anterior and posterior chamfers. The posterior condylar cut defines the flexion gap — excessive resection opens it (flexion instability), insufficient resection closes it (stiffness). In asymmetric posterior wear (common in varus), consider asymmetric resection or a posterior-referencing system.
- Insert 10mm spacer blocks between the tibial cut and femoral condyles at 90 degrees; check medial and lateral gaps are equal with 1-2mm laxity (rectangular) and equal in size to the extension gap (both about 10mm).
- Flexion tighter than extension: downsize the femur, resect more posterior condyle, or release the posterior capsule. Extension tighter than flexion: resect more distal femur, release further, or upsize the insert.
- CR if the PCL is intact, functional and appropriately tensioned — preserves native kinematics, more bone stock, no cam-post wear; tension is tuned with tibial slope (more slope relaxes the PCL).
- PS if the PCL is deficient, worn, arthritic or excessively tight — excise it and prepare the intercondylar box with a sagittal saw for the cam-post mechanism. CR and PS use different femoral components (not interchangeable) — decide before the femoral cuts. Major registries show broadly equivalent survivorship; choose on PCL quality and surgeon familiarity.
- Measure native thickness; resect cartilage and bone to leave 12-15mm, aiming for a composite (bone plus button) equal to native plus or minus 2mm.
- Free-hand or guided resection cutting medial and lateral facets equally; drill three peg holes for the button. Over-stuffing raises patellofemoral pressure and causes pain and maltracking; under-stuffing reduces the extensor moment arm and risks fracture. Never leave less than 10mm of bone.
- Insert femoral, tibial, insert (thickness from the gap assessment) and patellar trials; reduce the knee.
- Confirm greater than 120 degrees flexion, full extension without lift-off or hyperextension, symmetric stability throughout the range, and a patella that stays centred in the groove with no lateral subluxation or tilt.
- This is the last chance before cementing. Lateral maltracking in terminal extension indicates femoral internal rotation — re-cut the femur; a lateral release alone will not fix it. Never cement a suboptimal trial.
- Remove all trials. Pulse-lavage every bone surface with at least 3 litres of saline at high pressure to remove blood, marrow fat and debris.
- Dry the bone with laparotomy sponges under pressure until no blood is visible; pack with dry sponges, consider epinephrine-soaked sponges (1:500,000) for persistent ooze. Wet bone halves cement penetration — this step directly determines long-term fixation.
- Vacuum-mix the cement (reduces porosity) and wait for dough stage (forms a ball without sticking to gloves).
- Pressurise cement into the bone with a gun (penetration 2-5mm), and apply cement to BOTH the bone surface and the implant undersurface to create a continuous mantle. Insert the component before polymerisation and hold it still during cure (6-8 minutes) — movement ruins the mantle. Adequate penetration and mantle thickness reduce progressive radiolucent lines and tibial debonding.
Cemented fixation remains the most reliable category in most national registries (roughly 90-93 percent survival at 15 years). Cementless TKA performs well only with specific modern designs and good bone quality, so reserve it for selected patients rather than routine use.
- Cement in sequence — tibial tray first (align with the medial third of the tibial tubercle and the second toe), then femur (seated on all five cuts at the set rotation), then patellar button (three pegs fully seated, centred). Remove excess cement continuously before it cures — posterior extrusion can compress the popliteal vessels.
- After the cement has fully polymerised (8-10 minutes), snap in the polyethylene insert and confirm the locking mechanism is engaged. Reduce the knee and confirm greater than 120 degrees flexion, full extension to 0 degrees, no impingement and stability throughout, with varus-valgus testing in flexion and extension. If ROM or stability is suboptimal, identify and correct the cause now — it cannot be easily fixed after cementing.
Once cement cures, malposition is very hard to correct and requires complete component removal with bone loss. Confirm rotation, sizing, gaps and tracking at the trial stage, before cementing.
- Release the tourniquet, wait 5-10 minutes for reactive hyperaemia, and systematically cauterise arterial then venous then capillary bleeders, paying attention to the gutters, quadriceps and capsular edges. Check distal pulses — an absent pulse needs immediate exploration.
- Irrigate thoroughly with 3 litres of saline. Drain placement is controversial — modern trials show no benefit and possible increased infection risk; omit it if hemostasis is excellent, or use a single deep drain removed by 24 hours.
- Close the medial arthrotomy watertight with a continuous No. 1 Vicryl from the tibial plateaus proximally (figure-of-8 to the quadriceps if extended), then subcutaneous 2-0 Vicryl, then skin (staples or subcuticular 3-0 Monocryl). Apply a sterile compression dressing.
Across the operation, five structures are at consistent risk: the popliteal artery (10-15mm posterior to the capsule — avoid hyperextension beyond 10 degrees, use curved osteotomes and bone-on-bone posterior retractors); the common peroneal nerve (wraps the fibular neck 20-30mm distal to the head — limit acute valgus correction to 15 degrees, 2-5 percent palsy risk in severe valgus); the infrapatellar branch of the saphenous nerve (crosses at the joint line — numbness in 30-50 percent, counsel preoperatively, avoid sharp transection); the medial collateral ligament (superficial fibres insert 50mm below the joint line, deep fibres on the plateau edge — release deep before superficial, never release the distal superficial insertion); and the patellar blood supply (lateral genicular arteries — stay 5mm medial to the patella, limit the lateral release). Full detail is summarised in Viva and Exam Focus.
Aftercare & Complications
Rehabilitation. Remove the bulky dressing at 24 hours and apply a lighter dressing. Begin ROM immediately — early motion is critical to prevent arthrofibrosis; the goal is 90 degrees flexion by discharge and 110 degrees by 6 weeks. Continuous passive motion is no longer routinely recommended; physiotherapy-directed active-assisted ROM is preferred. Mobilise weight-bearing as tolerated with a frame on day 1, progressing to crutches or a stick by day 2-3, with modern enhanced-recovery protocols emphasising same-day mobilisation and, in selected patients, day-case TKA. Driving resumes at 4-6 weeks (right-sided TKA affects brake reaction time); low-impact sport (golf, swimming, cycling) is encouraged, high-impact (running, tennis) discouraged. VTE prophylaxis combines mechanical (graduated stockings, intermittent pneumatic compression) and chemical prophylaxis using an individual risk-benefit assessment (AAOS/ACCP, NICE). Agents in common use include LMWH (e.g. enoxaparin 40mg subcutaneous daily), a DOAC (e.g. rivaroxaban 10mg daily) or aspirin, typically for about 14 days after TKA (longer after hip arthroplasty or for high-risk patients). The registry-nested CRISTAL randomised trial found aspirin had a HIGHER 90-day symptomatic VTE rate than enoxaparin after hip or knee arthroplasty (3.45 percent versus 1.82 percent) — so aspirin monotherapy should not be assumed equivalent to LMWH. Tranexamic acid (commonly 15mg/kg or 1g IV, often one dose pre-incision and one at closure; topical and oral routes are also effective) reduces blood loss and transfusion without increasing VTE risk and is endorsed by the combined AAOS/AAHKS/Hip Society/Knee Society/ASRA guideline — routine unless contraindicated. Complications
- Recognition
- ROM less than 90 degrees flexion at 6 weeks; goniometer assessment; radiographs to rule out malposition
- Prevention
- Early aggressive ROM from day 1, adequate pain control, avoid over-stuffing, ensure good tracking
- Management
- Intensive physiotherapy first-line; MUA if less than 90 degrees at 6-12 weeks (about 70 percent effective); arthroscopic/open lysis of adhesions if MUA fails or after 12 weeks; revision if malposition
- Recognition
- Buckling, recurrent effusions, pain; varus-valgus laxity greater than 5mm
- Prevention
- Meticulous gap balancing with spacer blocks at 0 and 90 degrees; equal rectangular gaps; correct rotation
- Management
- Strengthening and bracing (rarely successful); revision to thicker insert or constrained component; correct malrotation
- Recognition
- Start-up or activity-related pain; progressive radiolucent lines greater than 2mm, subsidence or migration
- Prevention
- Third-generation cement technique; mechanical axis within plus or minus 3 degrees; appropriate patient selection
- Management
- Exclude infection first (ESR, CRP, aspiration); revision with cement removal, re-cemention, augments, graft or stems for bone loss
- Recognition
- Superficial: erythema, discharge, cellulitis within 30 days. Deep: pain, fever, raised ESR/CRP, effusion, loosening; aspiration 90 percent sensitive off antibiotics
- Prevention
- Preoperative optimisation (glycaemic control, smoking cessation, weight loss); prophylactic antibiotic (cefazolin 2g) within 60 minutes of incision; modern theatre ventilation; watertight closure
- Management
- Superficial: oral antistaphylococcal antibiotics and wound care. Deep acute (less than 3 weeks, well-fixed): DAIR with polyethylene exchange plus targeted IV antibiotics. Deep chronic: two-stage revision with antibiotic-loaded spacer and reimplantation once controlled
- Recognition
- Anterior knee pain, sensation of shifting, lateral subluxation, positive apprehension; tilt or subluxation on sunrise view, malrotation on CT
- Prevention
- Correct femoral rotation (3 degrees external, parallel to Whiteside's line); avoid internal rotation; restore native patellar thickness; centred button
- Management
- Conservative (VMO strengthening) rarely durable; lateral release if not done (high failure alone); revision of an internally rotated femoral component is definitive; tibial tubercle medialisation for severe cases
- Recognition
- Intraoperative fracture during eversion/resection, or postoperative anterior knee pain with an extensor lag
- Prevention
- Avoid over-resection (minimum 10mm bone); symmetric resection; gentle eversion; limit lateral release
- Management
- Non-displaced with intact extensor mechanism: cast or brace 6 weeks. Displaced or extensor disruption: tension-band or cerclage ORIF. Loose button or comminuted: partial/complete patellectomy with button removal
- Recognition
- Acute pain, inability to weight-bear, deformity; classify with Lewis-Rorabeck (femur) or Felix (tibia)
- Prevention
- Avoid anterior femoral notching; careful insertion; address osteoporosis; avoid postoperative trauma
- Management
- Stable component: protected weight-bearing or ORIF with a locking plate. Loose component: revision with long-stemmed components plus fixation, grafting as needed
- Recognition
- Inability to straight-leg raise, palpable defect, patella alta (tendon) or baja (quadriceps); MRI confirms
- Prevention
- Careful tissue handling; avoid forced eversion; protect the tendon during tibial preparation; repair any avulsion immediately
- Management
- Acute (less than 2 weeks): primary repair with No. 5 non-absorbable suture plus allograft augmentation, brace 6 weeks. Chronic: Achilles or extensor-mechanism allograft reconstruction; accept limited outcomes
- Recognition
- Foot drop, sensory loss over the dorsum and first web space; EMG/NCS grades the injury (highest in valgus correction greater than 15 degrees)
- Prevention
- Limit acute valgus correction to 15 degrees; graduated lateral releases; avoid hyperextension during closure; minimise tourniquet time; counsel high-risk patients
- Management
- Expectant initially (about 80 percent resolve by 6 months); AFO for foot drop; physiotherapy to prevent equinus; nerve conduction at 6 weeks and 3 months; consider fibular-tunnel decompression at 3-6 months if no recovery (controversial)
- Recognition
- DVT: swelling, pain, warmth; duplex diagnostic. PE: dyspnoea, chest pain, tachycardia, hypoxia; CTPA diagnostic
- Prevention
- Mechanical prophylaxis from admission; early mobilisation; chemical prophylaxis (LMWH, DOAC or aspirin) about 14 days by risk; CRISTAL showed aspirin inferior to enoxaparin, so prefer LMWH/DOAC in higher-risk patients
- Management
- Therapeutic anticoagulation (LMWH bridging to warfarin INR 2-3, or a DOAC such as rivaroxaban 15mg twice daily for 3 weeks then 20mg daily) for at least 3 months; respiratory support and thrombolysis for massive PE; IVC filter if anticoagulation is contraindicated
Registry perspective on complications (global). Cumulative figures vary modestly between registries (NJR, AJRR, AOANJRR, NZJR, SHAR) and with implant and patient mix, but the consistent messages are: an overall revision rate of roughly 6-8 percent at 15 years; aseptic loosening as a leading mode of late revision, markedly reduced since the 1990s with modern cement technique and implant design; infection typically around 1 percent cumulatively but consistently among the top reasons for revision and the dominant reason for early revision; instability underscoring the importance of gap balancing and rotation; cemented fixation remaining the benchmark while cementless results are design-dependent; CR versus PS broadly equivalent; and patellar resurfacing showing a small reduction in re-operation for anterior knee pain, with practice varying widely between countries.
Viva & Exam Focus
ROTATIONROTATION — femoral component rotational landmarks
BALANCEDBALANCED — gap balancing technique in TKA
- Location
- 10-15mm posterior to the posterior capsule at the joint line, closely adherent in the popliteal fossa; most at risk during posterior osteophyte removal
- How to protect it
- Avoid hyperextension beyond 10 degrees during exposure; curved osteotomes for posterior osteophytes; posterior retractors placed on bone; oscillating saw (never plunge) to complete the posterior cut
- Location
- Wraps the fibular neck 20-30mm distal to the fibular head; tethered at the fibular tunnel, vulnerable to stretch in valgus correction
- How to protect it
- Limit acute valgus correction to 15 degrees; graduated lateral releases rather than complete LCL release; keep the knee flexed during closure; counsel preoperatively (2-5 percent neuropraxia in severe valgus); consider staged correction beyond 20 degrees
- Location
- Main nerve crosses the medial incision at the joint line; the infrapatellar branch travels anteriorly across the field to the anterior knee skin
- How to protect it
- Accept numbness as expected (30-50 percent of patients); counsel preoperatively; avoid sharp transection (crush or cauterise branches to reduce neuroma); a vertical midline incision reduces branch injury
- Location
- Superficial fibres insert about 50mm below the joint line on the medial tibial metaphysis; deep fibres insert directly on the tibial plateau edge
- How to protect it
- Sequential graduated release — deep MCL (meniscotibial ligament) before superficial; subperiosteal elevation preserves fibre continuity; never release the distal superficial insertion (causes valgus instability); release proximal fibres from the medial epicondyle if needed for severe varus
- Location
- Lateral superior and inferior genicular arteries form an anastomosis supplying the patella from the lateral side; vulnerable to devascularisation if the arthrotomy is too lateral or the lateral release excessive
- How to protect it
- Arthrotomy 5mm medial to the patellar border preserves the lateral supply; limit the lateral retinacular release to the minimum needed for eversion (avoid extensive pie-crusting); maintain superior and inferior attachments; consider leaving the patella unresurfaced if the supply is compromised
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“You are performing a primary TKA via a medial parapatellar approach. After completing the bone cuts and trialling, the patella tracks laterally during the last 30 degrees of extension. What is the most likely cause and how do you address it intraoperatively?”
“You completed a primary TKA with good intraoperative ROM (0 to 130 degrees) and stable components, but on postoperative day 3 the patient flexes only to 70 degrees and is in significant pain. What are your differentials and management?”
“A 58-year-old with a severe 20-degree valgus deformity needs a TKA. What are the specific challenges and risks versus a varus deformity, how do you counsel the patient, and what is your balancing strategy?”
Indications
- Primary osteoarthritis (about 85 percent of TKAs) — tricompartmental disease failing conservative care
- Inflammatory arthritis (RA, psoriatic, AS) with severe destruction
- Post-traumatic arthritis after tibial plateau, distal femur or patellar fracture malunion
- Failed osteotomy (HTO, DFO) or unicompartmental arthroplasty with progression
Critical rotational landmarks (draw these)
- Whiteside's line — AP axis from the deepest trochlear groove to the intercondylar notch (component parallel)
- Transepicondylar axis — joining the epicondyles (most anatomical, hard to palpate)
- 3 degrees external rotation from the posterior condylar axis — most reliable single landmark
- All three should agree within 2 degrees — if conflict, use the combination (3 degrees external, confirm with Whiteside's line)
Gap balancing
- Equal, rectangular gaps — about 10mm with 1-2mm laxity in both flexion (90 degrees) and extension (0 degrees)
- Flexion tighter than extension: downsize the femur or resect more posterior condyle
- Extension tighter than flexion: resect more distal femur or release further
- Varus releases medial (deep MCL, then posterior capsule, then superficial MCL, then pes); valgus releases lateral (ITB, capsule, popliteus, LCL, gastrocnemius)
Third-generation cement technique
- Pulsatile lavage with at least 3 litres of saline
- Complete bone drying until no blood is visible
- Pressurised cement with a gun (penetration 2-5mm)
- Cement on BOTH bone surface and implant undersurface
- Insert before polymerisation and hold still during cure (6-8 minutes)
Five danger zones
- Popliteal artery (10-15mm posterior) — avoid hyperextension beyond 10 degrees, curved osteotomes, bone-on-bone retractors
- Common peroneal nerve (fibular neck) — limit valgus correction to 15 degrees, 2-5 percent palsy in severe valgus
- Infrapatellar branch of the saphenous nerve — accept 30-50 percent numbness, counsel preoperatively
- MCL — release deep before superficial, never the distal superficial insertion
- Patellar blood supply — arthrotomy 5mm medial to the patella, limit the lateral release
Registry survivorship (NJR, AJRR, AOANJRR, NZJR, SHAR)
- Cemented fixation is the benchmark — roughly 90-93 percent all-cause survival at 15 years
- CR versus PS broadly equivalent — choose on PCL quality and surgeon familiarity
- Patellar resurfacing slightly reduces re-operation for anterior knee pain; practice varies widely
- Leading revision reasons: infection, aseptic loosening, instability, unexplained pain (often malrotation)
Common complications
- Stiffness (5-10 percent) — most common; MUA if less than 90 degrees at 6-12 weeks (about 70 percent effective)
- Instability (1-3 percent) — gap mismatch; thicker insert or constrained implant
- Infection (superficial 2-4 percent, deep 0.5-2 percent) — acute DAIR, chronic two-stage revision
- Patellar maltracking (1-5 percent) — femoral internal rotation; revision is definitive
- Peroneal nerve palsy (0.3-5 percent) — about 80 percent resolve by 6 months; AFO for foot drop
Postoperative protocols (AAOS/ACCP, NICE)
- VTE prophylaxis — mechanical plus chemical (LMWH, DOAC or aspirin) by risk assessment, about 14 days; CRISTAL showed aspirin inferior to enoxaparin
- Early ROM — 90 degrees by discharge, 110 degrees by 6 weeks
- Tranexamic acid — reduces blood loss and transfusion with no added VTE risk (routine use)
- Weight-bearing as tolerated on day 1 — immediate mobilisation reduces VTE and stiffness
Background & Evidence
Global epidemiology and registry survivorship. TKA is among the most commonly performed elective orthopaedic operations, with continued growth driven by ageing populations — over 100,000 primary TKAs are recorded annually in the UK NJR alone. Primary osteoarthritis accounts for greater than 90 percent of primary TKAs in most registries; the mean age is in the late 60s (typical range 40-90 years) with a steadily increasing proportion of patients younger than 60. Across major registries (NJR for England, Wales, NI and IoM; AJRR in the US; AOANJRR in Australia; NZJR in New Zealand; SHAR in Sweden), cemented fixation is the best-performing category with all-cause survivorship of roughly 90-93 percent at 15 years and a cumulative revision rate of roughly 6-8 percent at 10-15 years. CR and PS designs show broadly equivalent survivorship; cementless results are design-dependent; and patellar resurfacing shows a small reduction in re-operation for anterior knee pain, with practice varying widely between countries. Functional outcomes. Mean Oxford Knee Score improves by about 17 points (preop 22 to postop 39 out of 48); WOMAC improves about 60 percent for pain and 55 percent for function. Patient satisfaction at one year is high (about 82 percent very satisfied, 15 percent satisfied, 3 percent dissatisfied). Mean postoperative flexion is about 115 degrees (goal greater than 110 degrees for daily activities) with a mean 2-degree flexion contracture; preoperative ROM is the most important predictor, and maximal improvement is achieved by 6 months with little gain after 12 months. At one year about 85 percent walk unlimited distances, 70 percent manage stairs normally, and 80 percent of those working preoperatively return to work. Survivorship is about 95 percent at 10 years, 92 percent at 15 years, 88 percent at 20 years and 82 percent at 25 years; a 60-year-old has roughly a 15 percent revision risk by age 75. Evidence-based practice points. - Cement technique (Level I-II): modern third-generation technique improves interdigitation and reduces progressive radiolucent lines and aseptic loosening; vacuum mixing reduces porosity; thin or poorly penetrated cement and tibial debonding are recognised contributors to early loosening.
- Gap balancing versus measured resection (Level II): ligament-based versus bone-based techniques show no significant difference in outcomes, though gap balancing may reduce instability — surgeon preference.
- Tourniquet use (Level I): traditional tourniquet use reduces blood loss and improves visualisation; tourniquet-less TKA reduces pain and improves early ROM and recovery at the cost of more operative time and blood loss (offset by tranexamic acid) — trend toward tourniquet-less, both acceptable.
- Tranexamic acid (Level I): commonly 15mg/kg or 1g IV (often one dose pre-incision and one at closure), with topical and oral routes equally effective; significantly reduces blood loss and transfusion with no increased VTE risk; routine use unless contraindicated.
- Drain use (Level I): modern evidence shows no benefit for infection, blood loss or ROM and possible harm (retrograde contamination) — selective use or avoidance.
- VTE prophylaxis (Level I): combine mechanical and chemical prophylaxis by individual risk-benefit assessment; agents include LMWH, a DOAC or aspirin for about 14 days after TKA. The CRISTAL RCT found aspirin inferior to enoxaparin (3.45 percent versus 1.82 percent symptomatic VTE) — aspirin monotherapy is not equivalent to LMWH.
- Enhanced recovery (Level II): preoperative education, multimodal analgesia, opioid minimisation, immediate mobilisation and early discharge reduce length of stay, complications and cost with maintained outcomes; now standard internationally, with growing use of day-case TKA in selected patients.
References
The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty
- Defined Whiteside's line (the AP axis) from the deepest part of the trochlear groove to the centre of the intercondylar notch as a reference for femoral component rotation
- Using the AP axis rather than the posterior condylar axis significantly reduced patellar tracking problems requiring realignment in valgus knees
- In the AP-axis group, two-year follow-up showed no patellar instability
Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis
- In 75 cadaveric femora, the posterior condylar axis was internally rotated relative to the surgical epicondylar axis by a mean of 3.5 degrees in males
- Females showed a smaller mean posterior condylar angle (0.3 degrees internal rotation)
- Provides the anatomical basis for adding approximately 3 degrees of external rotation to the posterior condylar axis when setting the femoral component
Gap balancing versus measured resection technique for total knee arthroplasty
- Fluoroscopic analysis of TKA performed by gap balancing versus measured resection during a deep knee bend
- Condylar lift-off greater than 1mm occurred in 45-60 percent of measured-resection knees but in none of the gap-balanced knees
- Gap balancing produced better coronal-plane stability
The Efficacy of Tranexamic Acid in Total Knee Arthroplasty: A Network Meta-Analysis
- Network meta-analysis of 67 studies underpinning the combined AAOS/AAHKS/Hip Society/Knee Society/ASRA guideline
- Topical, IV and oral tranexamic acid were all superior to placebo for reducing blood loss and transfusion, with no formulation clearly superior
- Higher or repeat dosing did not significantly improve blood-sparing effect
Effect of Aspirin vs Enoxaparin on Symptomatic Venous Thromboembolism in Patients Undergoing Hip or Knee Arthroplasty: The CRISTAL Randomized Trial
- Registry-nested cluster-randomised trial of 9711 patients across 31 hospitals comparing aspirin with enoxaparin for VTE prophylaxis after THA or TKA
- 90-day symptomatic VTE was 3.45 percent with aspirin versus 1.82 percent with enoxaparin (difference 1.97 percent; 95 percent CI 0.54-3.41 percent)
- Aspirin failed non-inferiority; enoxaparin was significantly superior
The effect of post-operative mechanical axis alignment on the survival of primary total knee replacements after a follow-up of 15 years
- 501 primary TKAs followed for 15 years, divided into neutral mechanical axis (within plus or minus 3 degrees) versus maligned (greater than 3 degrees deviation)
- 33 of 458 TKAs (7.2 percent) were revised for aseptic loosening
- A neutral mechanical axis showed only a weak, non-significant trend toward improved survival (p = 0.47)
Total knee arthroplasty
- Classic description of the measured resection technique and component alignment principles for total knee arthroplasty
- Established the operative framework — bone cuts, gap assessment, component rotation and cement fixation — that still underpins modern TKA
Radiolucent lines around knee arthroplasty components: a narrative review
- Reviews the cement-bone interface, radiolucent lines, tibial debonding and aseptic loosening around knee arthroplasty components
- Links inadequate cement penetration and mantle thickness to progressive radiolucent lines and early failure
The use of tourniquet may influence the cement mantle thickness under the tibial implant during total knee arthroplasty
- Comparative study of cement mantle thickness, radiolucent lines and tourniquet use in TKA
- Tourniquet use was associated with measurable differences in the cement mantle beneath the tibial tray
Registry sources. National Joint Registry (NJR) for England, Wales, Northern Ireland, Isle of Man and Guernsey; American Joint Replacement Registry (AJRR); Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR); New Zealand Joint Registry (NZJR); Swedish Knee Arthroplasty Register (SHAR) — annual reports used as the cross-registry source for TKA survivorship, fixation, CR/PS and patellar resurfacing data.