Open or percutaneous release of the A1 pulley for stenosing flexor tenosynovitis | intermediate
- Finger surface landmark = the DISTAL PALMAR CREASE: the A1 pulley begins just distal to it, over the metacarpal head (Chung, cadaveric). The finger MCP flexion crease lies DISTAL to the joint over the proximal phalanx (A2 region) and is not the A1 landmark, so mark the distal palmar crease or the palpable metacarpal head.
- Thumb A1 pulley proximal edge lies only about 3.5 mm distal to the thumb MCP flexion crease (Buldu, cadaveric). In OPEN thumb release the ULNAR digital nerve is closest to the pulley (about 2 mm) and is at greatest risk; in PERCUTANEOUS release the RADIAL digital nerve, which crosses the flexor tendon just proximal to the A1 pulley, is most at risk.
- Corticosteroid injection resolves symptoms in roughly 60 to 90 percent of cases short-term, but recurrence is common by one year, especially in diabetics and multi-digit disease. A Cochrane review shows open surgery has markedly lower recurrence than injection (8/140 vs 50/130 at 6 to 12 months, RR 0.17).
- Complete A1 release is verified when the flexor tendon glides smoothly through the sheath with full passive and active flexion and extension — any residual catching must be addressed before closure.
- Diabetic patients have lower injection success (30 to 50 percent at one year) and warrant an earlier surgical threshold; paediatric trigger thumb (Notta's node) is observed initially — about a third resolve spontaneously, and an IP flexion contracture greater than 30 degrees rarely resolves and favours earlier release.
When & Why
Indication. Symptomatic trigger finger or thumb — painful catching or locking at the MCP level, tenderness over the A1 pulley at the metacarpal head, and reproduction of triggering on flexion and extension — after a fair trial of non-operative treatment. Surgery is offered for a Grade IV trigger (fixed flexion not passively reducible), failure or recurrence after two corticosteroid injections, recurrence within 6 months of a second injection, or a paediatric trigger thumb persisting beyond around 3 years of age. Absolute indications
- Grade IV trigger (locked digit in fixed flexion, not passively reducible)
- Failed conservative treatment after two corticosteroid injections
- Recurrence within 6 months of a second injection
- Paediatric trigger thumb persisting beyond 3 years of age (Notta's node) Relative indications
- Patient preference for definitive treatment over repeat injections
- Grade III triggering after a failed single injection
- Multiple digit involvement with significant functional impairment
- Suspected concomitant flexor sheath pathology (nodule, ganglion) needing open exploration Contraindications. Absolute: an active flexor sheath infection (Kanavel signs positive — this needs urgent washout, never an injection or pulley release) and uncontrolled anticoagulation in the setting of a percutaneous release. Relative: Grade I to II triggering with no prior trial of injection (try injection first), pregnancy (defer unless severe), and an active psoriatic or rheumatoid flare (optimise medical management first). Try non-operative treatment first. A corticosteroid injection resolves symptoms in roughly 60 to 90 percent of trigger digits in the short term, but recurrence is common within a year and is higher in diabetics and multi-digit disease; two injections are a reasonable maximum before offering surgery, and a third adds little benefit. The standard technique is about 1 mL of triamcinolone acetonide 40 mg/mL (or methylprednisolone) with 0.5 mL of 1 percent lidocaine injected into the flexor tendon sheath at the A1 level — confirm the needle is intra-sheath and not intratendinous by watching it move with passive tendon excursion before injecting. A Cochrane review (Leow 2021) found injected NSAIDs offer little benefit over glucocorticoid, and a static MCP extension or blocking splint is a low-risk adjunct for mild Grade I to II disease but is generally less effective than injection alone. Open or percutaneous? Both are appropriate in a suitable finger. The choice is guided by the digit, the setting and surgeon preference:
High complete-release rate with low recurrence, direct visualisation of the neurovascular bundles — particularly valuable in the thumb — and it allows inspection and excision of associated tenosynovial pathology. The long-standing standard.
High success in the index, middle and ring fingers, with lower cost, faster recovery and no formal incision. A meta-analysis of 8 RCTs (Casey 2024, 548 patients) found no significant difference from open release in revision, complication or pain rates.
Use caution. The radial digital nerve crosses just proximal to the pulley, so for the thumb prefer an open release or an ultrasound-guided percutaneous release, never a blind needle release.
- Open release
- 99-100%
- Percutaneous (finger)
- 97-100%
- Percutaneous (thumb)
- 90-97% (ultrasound-guided)
- Open release
- less than 1%
- Percutaneous (finger)
- 2-5%
- Percutaneous (thumb)
- 3-7%
- Open release
- less than 0.1% (direct vision)
- Percutaneous (finger)
- 0.3-1%
- Percutaneous (thumb)
- up to 5% without ultrasound
- Open release
- 3-7 days
- Percutaneous (finger)
- 1-3 days
- Percutaneous (thumb)
- 1-3 days
- Open release
- 5-10%
- Percutaneous (finger)
- minimal
- Percutaneous (thumb)
- minimal
- Open release
- theatre or clinic
- Percutaneous (finger)
- clinic / WALANT
- Percutaneous (thumb)
- clinic with ultrasound
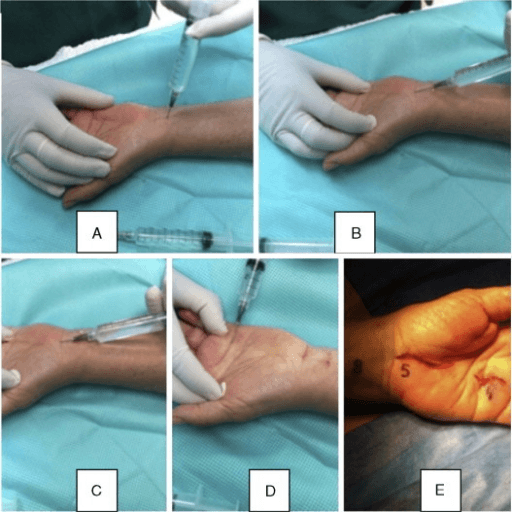
Consent. Counsel specifically on digital nerve injury (less than 0.1 percent for an open finger, 0.5 to 2 percent for an open thumb, and higher for a percutaneous thumb without ultrasound), incomplete release (1 to 2 percent open), wound infection (less than 1 percent), scar sensitivity, and a temporary 10 to 25 percent grip-strength reduction that recovers over 3 to 6 months. Setup. Supine with the arm abducted 90 degrees on a hand table and the forearm supinated. WALANT is strongly preferred — 2 to 3 mL of 1 percent lidocaine with 1:100,000 epinephrine injected subcutaneously 15 to 20 minutes before incision; no tourniquet is required, but if one is used a forearm tourniquet at 200 mmHg is more comfortable. The awake patient confirms resolution of the triggering by active flexion before skin closure.
The Operation
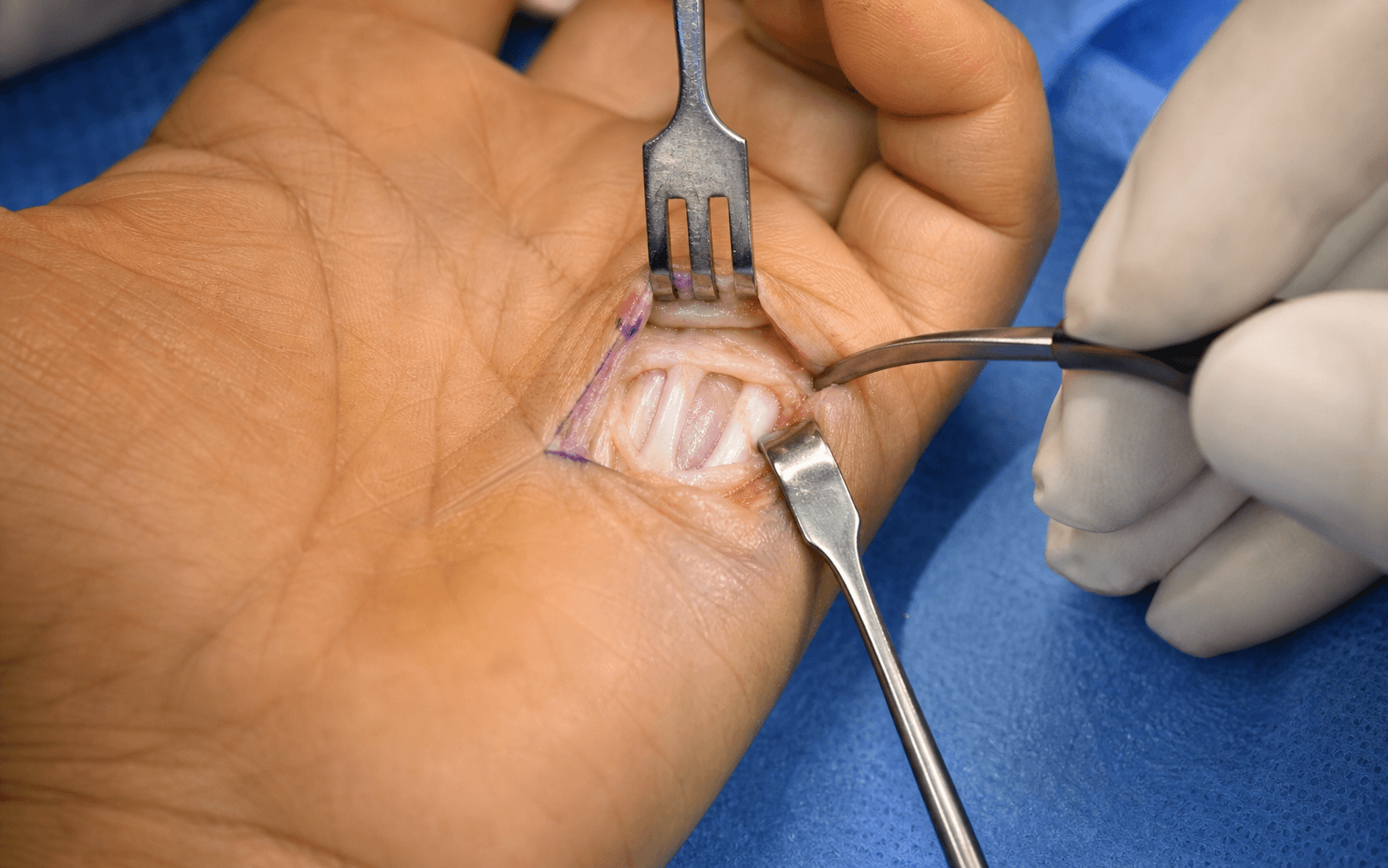
The goal is to divide the thickened A1 pulley completely from its proximal to distal margin while protecting the flanking digital nerves and the underlying flexor tendon, then confirm smooth tendon gliding before closure. The exposure is laid out in full in the steps below.

Open A1 pulley release
- Supine, arm on a hand table, forearm supinated.
- WALANT preferred: 2 to 3 mL of 1 percent lidocaine with 1:100,000 epinephrine, 15 to 20 minutes before incision. No tourniquet is needed; if used, a forearm tourniquet at 200 mmHg.
- Loupe magnification (minimum 2.5x) for the thumb, where the digital nerves are closest to the pulley.
- Flex and extend the digit to confirm triggering, then palpate the metacarpal head (the bony prominence of the knuckle in extension).
- Finger: mark a transverse incision at the distal palmar crease over the palpable metacarpal head — the A1 pulley begins just distal to the distal palmar crease. Do NOT centre on the finger MCP flexion (digital) crease, which lies distal to the joint over the proximal phalanx. A short longitudinal or oblique incision is an acceptable alternative.
- Thumb: mark a transverse or gently curved incision at the MCP flexion crease (the A1 proximal edge lies about 3.5 mm distal to it) under loupe magnification.
- Incise the skin sharply with a number 15 blade and deepen through subcutaneous fat with spreading scissors in line with the digit, protecting superficial veins.
- Finger: identify the digital neurovascular bundles 4 to 6 mm lateral to the sheath and retract them with skin hooks or vessel loops.
- Thumb: identify BOTH digital nerves before any pulley work — the radial nerve crosses the flexor tendon just proximal to the A1, and the ulnar nerve hugs the ulnar border (cadaveric mean about 1.95 mm away) and is the closest structure to the dividing blade.
- Deepen to the A1 pulley — a distinct thickened white fibrous band with transverse fibres lying over the flexor tendon.
- Identify the proximal and distal edges of the A1.
- Confirm the A2 pulley immediately distal and mark the A1-to-A2 boundary with a small clip so the A2 is not inadvertently divided.
- With a number 15 blade or tenotomy scissors, insert a fine elevator beneath the proximal margin first, then divide the pulley longitudinally in the midline from proximal to distal under direct vision.
- Advance the blade along the pulley surface, directing it away from the underlying tendon.
- Thumb: divide in the midline with both nerves protected, keeping the blade angled away from the ulnar border (where the ulnar nerve lies closest) and ensuring the crossing radial nerve is clear before dividing.
- With the wound open, actively flex and passively extend the digit — under WALANT the patient actively flexes and extends and confirms the triggering has resolved.
- The tendon must glide smoothly with no snapping, catching or triggering.
- If catching persists, check for a residual distal A1 tether, A2 proximal margin catching, an FDS-FDP mismatch at the chiasma of Camper (rare), or a large tenosynovial nodule needing excision.
- Close the skin with 4-0 non-absorbable interrupted sutures (nylon or Prolene) in the finger, or 4-0 absorbable sutures in children.
- Apply a non-adherent dressing — no splint is required.
- Encourage immediate active mobilisation from day 1.

In the thumb BOTH digital nerves lie close to the A1 pulley. The ulnar nerve (cadaveric mean 1.95 mm) is the closest structure to the blade in an open release; the radial nerve crosses the flexor tendon just proximal to the pulley and is most at risk in a percutaneous release. Identify both under direct vision, keep the blade angled away from the ulnar border, and never perform a blind percutaneous thumb release without ultrasound guidance.
The finger MCP flexion crease overlies the proximal phalanx (A2 region), distal to the joint — centring on it misses the proximal A1 and risks an incomplete release. Use the distal palmar crease or the palpable metacarpal head, and re-confirm the level by palpation with the joint in extension, especially in an obese hand.
Only the A1 is released. Mark the A1-to-A2 boundary before cutting — extending the division into the A2 proximal margin causes bowstringing. Divide the full length of the A1 but stop at the A2.
An awake patient who actively flexes and extends through the sheath confirms, before closure, that the triggering has resolved. Any residual catching means the release is incomplete — most often a small tether at the distal A1 margin.
In the thumb I use minimum 2.5x loupes, look first for the radial digital nerve crossing proximal to the pulley, then for the ulnar nerve at the ulnar border, protect both with a vessel loop, and divide in the midline keeping the blade away from the ulnar border under direct vision throughout.
Percutaneous needle release Indications. A Grade II to III trigger finger (not the thumb without ultrasound), patient preference, a clinic setting, or multiple digits. Avoid it in Grade IV fixed triggering, a previous failed release, or suspected tenosynovial pathology. Technique
- Mark the A1 level at the distal palmar crease or palpated metacarpal head.
- Infiltrate 1 to 2 mL of WALANT subcutaneously.
- Insert an 18-gauge needle through the skin into the sheath at the proximal A1 margin, bevel parallel to the tendon.
- Confirm intrasheath position — the needle moves with tendon excursion.
- Rotate the bevel to cut perpendicular to the transverse pulley fibres and make 3 to 5 controlled sweeping cuts from proximal to distal.
- Ask the patient to actively flex and extend — confirm resolution of triggering; if it persists, advance to the distal margin and repeat.

I do not perform a blind percutaneous release in the thumb — the radial digital nerve crosses just proximal to the pulley and can be transected before the needle reaches it. For the thumb I use an open release, or an ultrasound-guided percutaneous release, identifying both digital nerves first.
Aftercare & Complications
Rehabilitation | Phase | Timing | Management | |-------|--------|-----------| | Immediate | Day 0 to 2 | Non-adherent dressing, no splint; elevate above the heart for 48 hours; begin active flexion and extension of the released digit from day 1 | | Early | Day 2 to 14 | Light activities and driving when a safe grip is possible; paracetamol or NSAIDs (opioids rarely needed); sutures out at 10 to 14 days | | Return to function | 1 to 6 weeks | Office work within 1 week, manual work 2 to 3 weeks; full grip strength by 4 to 6 weeks | | Hand therapy | As indicated | Pre-existing PIP flexion contracture, scar tenderness beyond 4 weeks, stiffness at 4 to 6 weeks, or diabetic multi-digit disease | Grip strength is reduced by 10 to 25 percent for up to 3 to 4 months after open release and returns to baseline in most patients by 3 to 6 months — explain this before surgery. Most patients return to desk work within a week and to manual work by 2 to 3 weeks. Complications
- Recognition
- Immediate sensory loss or numbness in the nerve distribution (less than 0.1 percent open finger, 0.5 to 2 percent open thumb, up to 5 percent percutaneous thumb without ultrasound)
- Prevention and management
- Identify nerves under direct vision before dividing; avoid blind percutaneous thumb release. Primary neurorrhaphy if recognised intraoperatively; if delayed, explore and repair or graft with sensory re-education
- Recognition
- Persistent triggering on active flexion after surgery (1 to 2 percent open)
- Prevention and management
- Verify smooth gliding under direct vision and with WALANT active flexion before closure. If catching persists at 2 to 4 weeks, return to theatre for open revision release
- Recognition
- Visible and palpable tendon bow on flexion with weak grip (less than 0.5 percent, from inadvertent A2 release)
- Prevention and management
- Mark the A1-to-A2 boundary before cutting and release only the A1. Usually tolerated; severe symptomatic cases may need A2 reconstruction with a tendon graft
- Recognition
- Erythema, warmth, swelling, purulent discharge (less than 1 percent)
- Prevention and management
- Sterile WALANT technique and meticulous haemostasis. Wound swab and oral antibiotics (cefalexin); deep infection needs washout, IV antibiotics, and exclusion of flexor sheath involvement
- Recognition
- Tender scar with limited active flexion despite full passive ROM at 6 to 8 weeks (5 to 15 percent)
- Prevention and management
- Transverse incision, early mobilisation, scar massage from 2 weeks. Silicone gel and hand therapy; steroid injection for a hypertrophic scar; rarely surgical revision
- Recognition
- Return of triggering at 6 to 24 months (less than 1 percent open, 3 to 7 percent percutaneous)
- Prevention and management
- Complete A1 release verified intraoperatively. A single repeat injection may be tried; refractory cases need revision open release with tenosynovectomy
- Recognition
- Painful swollen digit with bruising and stiffness (1 to 3 percent)
- Prevention and management
- Haemostasis before closure and a compressive dressing for 24 hours. Most resolve with elevation and ice; a large stiff haematoma may need washout to prevent adhesions
- Recognition
- Inability to fully extend the PIP (rare; more common in missed Grade IV)
- Prevention and management
- Release before Grade IV develops and mobilise early. Established contracture: night extension splinting; if greater than 30 degrees and persistent beyond 6 months, consider volar plate release
Viva & Exam Focus
PULLEYPULLEY — A1 pulley release
TRIGGERTRIGGER — clinical assessment
The finger MCP flexion crease overlies the proximal phalanx, distal to the joint, not the A1 pulley. Centre the incision on the distal palmar crease or palpable metacarpal head, or the proximal A1 is missed and the release is incomplete.
de Quervain's is pain over the radial styloid with a positive Finkelstein test (APL and EPB in the first dorsal compartment). Trigger finger is catching or locking at the MCP level from A1 stenosis around FDS and FDP. Dupuytren's is a palmar cord causing progressive MCP and PIP flexion contracture (fascia, not tendon).
Kanavel's four signs — semi-flexed posture, fusiform swelling, tenderness along the whole flexor sheath, and pain on passive extension — mean a septic flexor sheath, a surgical emergency. Trigger finger is intermittent snapping at the MCP level with localised A1 tenderness and no systemic features. Never inject a septic sheath.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old woman with Type 2 diabetes has a trigger ring finger. She has had two corticosteroid injections over 18 months — relief lasted 4 to 6 months after the first and only 6 weeks after the second — and now has Grade III triggering. How do you manage her?”
“You are about to perform a trigger thumb release on a 45-year-old woman with Grade III triggering of the right thumb. Talk me through the specific precautions for the thumb compared to a trigger finger.”
“A patient is 6 weeks post open A1 pulley release for a trigger ring finger. The triggering has resolved, but they have significantly reduced grip strength compared with the other hand. How do you explain this and what is the management?”
Indication and diagnosis
- Grade IV fixed flexion is an absolute indication; also failed two injections or recurrence within 6 months of the second
- Paediatric trigger thumb persisting beyond around 3 years
- Green grading: I pain only, II catching, III locking reducible, IV fixed flexion
- Tenderness is localised to the A1 over the metacarpal head, not the whole sheath
Surface landmark
- Finger: centre on the DISTAL PALMAR CREASE or metacarpal head, not the digital crease which is distal to the joint
- Thumb: A1 proximal edge about 3.5 mm distal to the MCP crease
- Confirm the level by palpating the metacarpal head with the joint in extension
The operation
- WALANT preferred — the awake patient confirms resolution intraoperatively
- Divide the A1 completely from proximal to distal; mark the A1-to-A2 boundary
- Verify smooth gliding with WALANT active flexion before closure
- Immediate mobilisation from day 1, no splint
Danger structures
- Thumb ulnar digital nerve is closest in OPEN release
- Thumb radial digital nerve is most at risk in PERCUTANEOUS release
- The A2 pulley must be preserved (bowstringing)
- Flexor sheath infection (Kanavel) is a surgical emergency, never an injection
Non-operative treatment
- Corticosteroid injection 60 to 90 percent short-term, recurrence common by one year
- Two injections maximum before surgical referral
- Splinting is an adjunct, not equivalent to injection
- Diabetics have lower success (30 to 50 percent at one year)
Complications
- Digital nerve injury: less than 0.1 percent open finger, up to 5 percent percutaneous thumb without ultrasound
- Incomplete release 1 to 2 percent open — verify with WALANT
- Bowstringing less than 0.5 percent from inadvertent A2 release
- Recurrence less than 1 percent open, 3 to 7 percent percutaneous
Special cases
- Paediatric thumb: observe, about a third resolve; IP contracture over 30 degrees favours surgery; 95 to 98 percent surgical success
- Diabetic: earlier surgery, perioperative antibiotics, 14-day sutures, screen all digits
- Percutaneous release is acceptable for Grade II to III fingers but not the thumb without ultrasound
Background & Evidence
Epidemiology and risk factors. Trigger finger is a common stenosing flexor tenosynovitis, most frequent in middle-aged women with a peak between 40 and 60 years, and strongly associated with diabetes mellitus, hypothyroidism, rheumatoid arthritis and renal dialysis. Diabetic patients are affected far more often than the general population and frequently have multiple digit involvement (up to 4 to 5 digits). Pathoanatomy. A size mismatch develops between a thickened, nodular flexor tendon (FDS and FDP in the fingers; FPL alone in the thumb) and a thickened, stenotic A1 pulley, producing catching and then locking at the MCP level. The tendon nodule is termed Notta's node in children. Histology of the A1 pulley correlates with the clinical grade (Drossos), showing fibrocartilaginous metaplasia rather than pure inflammation.
- Clinical feature
- Pain and tenderness over the A1; no mechanical symptoms
- Typical management
- Splint, NSAIDs, corticosteroid injection
- Clinical feature
- Catching, but the patient can actively extend
- Typical management
- Corticosteroid injection; repeat or surgery if it fails
- Clinical feature
- Locking that requires passive extension
- Typical management
- Corticosteroid injection; surgery if recurrent or Grade IV develops
- Clinical feature
- Fixed flexion contracture, not passively reducible
- Typical management
- Surgical release
Pulley anatomy (reference). The flexor tendon sheath contains five annular and three cruciate pulleys. In trigger finger ONLY the A1 is released; the A2 and A4 are critical and must be preserved, and the cruciate pulleys can all be divided without biomechanical consequence.
- Location
- MCP joint (metacarpal head)
- Length
- 8 to 10 mm
- Significance
- Pathological in trigger finger — released at surgery
- Location
- Proximal half of proximal phalanx
- Length
- 15 to 17 mm
- Significance
- Critical — must NOT be released (bowstringing)
- Location
- PIP joint
- Length
- 2 to 3 mm
- Significance
- Expendable
- Location
- Middle of middle phalanx
- Length
- 7 to 9 mm
- Significance
- Critical — must NOT be released
- Location
- DIP joint
- Length
- 2 to 3 mm
- Significance
- Expendable
Neurovascular anatomy (reference). In the finger the digital nerves run 4 to 6 mm lateral to the sheath in the mid-lateral line and are relatively protected at the A1 level. In the thumb they are far closer: the ulnar digital nerve a mean of 1.95 mm and the radial 3.40 mm from the pulley (Buldu), and the radial nerve crosses the flexor tendon just proximal to the A1. This is why the at-risk nerve in the thumb depends on the technique — ulnar in an open release, radial in a percutaneous release. Key evidence. The Cochrane review (Fiorini 2018, 14 trials, 1260 participants) found open surgery had markedly lower recurrence than corticosteroid injection (8/140 vs 50/130 at 6 to 12 months, RR 0.17) at the cost of more early palmar pain. A meta-analysis of 8 RCTs (Casey 2024, 548 patients) found no significant difference between open and percutaneous A1 release in revision, complication or pain rates, so both are appropriate in suitable fingers. Benson and Ptaszek (1997) supported proceeding to surgery after a failed injection given the permanency of relief, and Hutchinson (2021) established the natural history of paediatric trigger thumb — about 32 percent resolve spontaneously by 5 years, but an IP contracture greater than 30 degrees rarely does.
References
Open versus percutaneous release of trigger finger: meta-analysis
Meta-analysis of 8 randomised controlled trials (548 patients; 278 percutaneous, 270 open). No significant difference between open and percutaneous A1 pulley release in revision, complication or pain rates. Both are appropriate surgical options in suitable fingers.
Surgery for trigger finger (Cochrane systematic review)
14 trials, 1260 participants (1361 trigger fingers). Open surgery had markedly lower recurrence than steroid injection (8/140 vs 50/130 at 6 to 12 months, RR 0.17) but caused more early palmar pain in the first post-operative week (RR 3.69); evidence graded low quality.
Injection versus surgery in the treatment of trigger finger
Comparative review of 109 trigger fingers. Surgical A1 pulley release offered greater permanency of symptom relief than repeat injection, supporting surgery as a reasonable next step after a single failed corticosteroid injection.
Correlations between clinical presentations of adult trigger digits and histologic aspects of the A1 pulley
Prospective cohort correlating A1 pulley histology (fibrocartilaginous metaplasia) with the clinical grade of triggering.
References to avoid complications in releases of the trigger thumb: a cadaveric study
Dissection of 20 thumbs. The ulnar digital nerve lies closer to the pulley (mean 1.95 mm) than the radial (mean 3.40 mm) — most at risk in OPEN release; the radial nerve crosses proximal to the A1 — most at risk in PERCUTANEOUS release. The proximal A1 edge lies about 3.5 mm distal to the MCP crease.
The natural history of pediatric trigger thumb in the United States
Prospective cohort of 78 children (93 thumbs), mean age 20 months, followed a mean 4.3 years. 32 percent resolved spontaneously by 5 years; each degree of initial IP flexion reduced resolution by 3 percent, and contractures greater than 30 degrees resolved in only about 2.5 percent. Bilateral involvement increased the likelihood of surgery.
Efficacy of cortisone injection in treatment of trigger fingers and thumbs
Key early series establishing the efficacy of corticosteroid injection for trigger finger and thumb.
Diagnostic and therapeutic value of injection for trigger finger and thumb
Original description of the Green grading classification (I to IV) used clinically to stage triggering.
Conservative management of trigger finger
Natural history and the non-operative management evidence base for trigger finger.