Subcutaneous, intramuscular or submuscular (Learmonth) transposition of the ulnar nerve for cubital tunnel syndrome where in-situ decompression is insufficient · advanced
- Anterior transposition is indicated when simple in-situ decompression is insufficient: nerve subluxation over the medial epicondyle, prior medial epicondyle malunion with valgus deformity, revision surgery after failed in-situ release, throwing athletes requiring nerve stability, and severe disease (McGowan grade II-III or Dellon stage 3) with marked intrinsic wasting.
- Five proximal-to-distal compression sites must ALL be released: (1) Arcade of Struthers, (2) medial intermuscular septum, (3) cubital tunnel retinaculum (Osborne's band), (4) floor of the cubital tunnel groove, and (5) the aponeurosis between the two heads of flexor carpi ulnaris. Missing any site risks persistent or recurrent symptoms.
- The medial intermuscular septum must be EXCISED (a 2-3 cm window resected) — not simply released or incised. A retained septal edge kinks the nerve when it is transposed anteriorly, because the nerve now passes through the septal opening at an angle rather than running parallel to it as it did in its native anatomical position.
- The ulnar nerve receives a segmental extrinsic blood supply from the superior and inferior ulnar collateral arteries, the posterior ulnar recurrent artery, and the ulnar artery. During mobilisation the vasa nervorum must be preserved; over-dissection (skeletonisation) risks devascularisation, post-ischaemic fibrosis, and worse outcomes. The nerve should be mobilised only as far as necessary for the transposition.
- “The elbow flexion test is the most sensitive provocative test for cubital tunnel syndrome: hold the elbow in full flexion with the wrist extended for 60 seconds. Sensitivity approximately 89%, specificity approximately 99% (Elhassan et al.). A positive test reproduces paraesthesiae in the ulnar nerve distribution.
- “The medial antebrachial cutaneous nerve (MABC) runs 2-3 cm anterior to the medial epicondyle and is vulnerable during the proximal skin incision and deep dissection. Entrapment or laceration produces a painful neuroma that can be more debilitating than the original cubital tunnel symptoms. Identify it early and protect it throughout.
- “In submuscular (Learmonth) transposition, the flexor-pronator mass origin is detached from the medial epicondyle en masse — not individual muscle releases. The ulnar collateral ligament (UCL) of the elbow lies deep to the common flexor origin and must be protected. Repair is with suture anchors or transosseous drill holes.
- “Articular branches to the elbow joint leave the ulnar nerve proximal to the cubital tunnel. These must be preserved during nerve mobilisation — division produces medial elbow pain and a sense of joint instability post-operatively that can mimic UCL insufficiency.
When & Why
Indication. Anterior transposition of the ulnar nerve is reserved for cubital tunnel syndrome where simple in-situ decompression is insufficient. The core principle is identical in every case — release all five compression sites and move the nerve to a tension-free bed — but transposition (rather than leaving the nerve in place) is chosen for specific reasons. Absolute indications for transposition over in-situ release
- Ulnar nerve subluxation or partial dislocation over the medial epicondyle on elbow flexion — in-situ release destabilises the nerve further and leaves it snapping over the epicondyle in its native groove.
- Prior medial epicondyle fracture with malunion or valgus deformity — the bony geometry of the cubital tunnel is altered and simple decompression does not address the structural abnormality.
- Revision cubital tunnel surgery after failed in-situ decompression — transposition moves the nerve out of scar tissue and residual compression; repeat in-situ release has poor outcomes.
- Severe cubital tunnel syndrome with marked intrinsic wasting (McGowan grade III, Dellon stage 3) — the nerve needs a protected, tension-free bed.
- Throwing athletes or overhead-sport patients where the nerve must be stabilised to tolerate repeated valgus stress and elbow flexion. Relative indications. Moderate disease (McGowan grade II) in a patient whose occupation demands reliable grip strength; an elbow contracture requiring simultaneous capsular release (transposition avoids tethering the nerve during that release); bony pathology in the cubital tunnel (osteophytes, synovial chondromatosis, loose bodies); or patient preference after informed discussion of the trade-offs. Contraindications. Active infection at the medial elbow, and severe medical comorbidity precluding tourniquet use and anaesthesia, are absolute. Mild disease (McGowan grade I), a poor soft-tissue envelope from prior surgery or trauma, and a previous medial epicondylectomy (altered bony anatomy) are relative. Clinical assessment before deciding. Confirm cubital tunnel syndrome with a positive elbow flexion test (the most sensitive provocative test) and a Tinel sign at the cubital tunnel, then specifically assess for nerve subluxation by palpating the nerve while passively flexing the elbow — the finding that most often converts a planned in-situ release into a transposition. Try conservative treatment first for mild disease. Night-time elbow extension splinting at 30 to 45 degrees of flexion, nerve gliding exercises and activity modification improve approximately 50 to 70 percent of mild cases; surgery follows failure of 3 to 6 months of consistent non-operative care, or any progressive neurological deficit. Which operation? The decision. For primary, idiopathic disease without subluxation, simple in-situ decompression is a reasonable first choice (simpler, faster, lower morbidity). Anterior transposition is preferred when a specific indication is present — and the choice of transposition bed (subcutaneous versus submuscular/Learmonth) depends on the indication and surgeon preference.
- In-situ decompression
- Mild-moderate primary disease, no subluxation
- Subcutaneous transposition
- Subluxating nerve, revision, valgus, athletes
- Submuscular (Learmonth)
- Revision cases, severe disease, athletes needing deep cover
- Medial epicondylectomy
- Primary disease with normal medial epicondyle anatomy
- In-situ decompression
- Simple
- Subcutaneous transposition
- Moderate
- Submuscular (Learmonth)
- Complex
- Medial epicondylectomy
- Moderate
- In-situ decompression
- 6-8 cm
- Subcutaneous transposition
- 10-12 cm
- Submuscular (Learmonth)
- 12-15 cm
- Medial epicondylectomy
- 8-10 cm
- In-situ decompression
- Low (2-5%)
- Subcutaneous transposition
- Moderate (5-10%)
- Submuscular (Learmonth)
- Moderate-high (8-15%)
- Medial epicondylectomy
- Moderate (5-10%)
- In-situ decompression
- Native cubital tunnel (decompressed)
- Subcutaneous transposition
- Subcutaneous pocket anterior to the epicondyle
- Submuscular (Learmonth)
- Deep to the flexor-pronator mass
- Medial epicondylectomy
- Native tunnel (bony decompression)
- In-situ decompression
- 2-4 weeks
- Subcutaneous transposition
- 4-6 weeks
- Submuscular (Learmonth)
- 6-12 weeks
- Medial epicondylectomy
- 4-6 weeks
- In-situ decompression
- Low (minimal mobilisation)
- Subcutaneous transposition
- Moderate (more mobilisation)
- Submuscular (Learmonth)
- Higher (extensive mobilisation)
- Medial epicondylectomy
- Low (minimal mobilisation)
- In-situ decompression
- None
- Subcutaneous transposition
- None
- Submuscular (Learmonth)
- Low (if flexor-pronator detachment compromises the UCL)
- Medial epicondylectomy
- Low (reduced medial epicondyle strength for valgus)
- In-situ decompression
- 5-15%
- Subcutaneous transposition
- 3-10%
- Submuscular (Learmonth)
- 3-8%
- Medial epicondylectomy
- 5-12%
- In-situ decompression
- 75-90%
- Subcutaneous transposition
- 80-95%
- Submuscular (Learmonth)
- 80-95%
- Medial epicondylectomy
- 75-90%
Consent specifically for: incomplete relief or recurrence (5 to 15 percent), temporary or permanent worsening of ulnar nerve function (less than 2 percent), medial forearm numbness or a painful MABC neuroma (2 to 5 percent), wound infection (less than 2 percent), elbow stiffness or flexion contracture, and possible revision surgery. Setup. Supine, arm abducted 90 degrees on a hand table, forearm supinated with the elbow facing upward, upper-arm tourniquet (250 mmHg). General or regional (axillary or supraclavicular) anaesthesia. Examine under anaesthesia for subluxation and range of motion before draping, and document any instability or loose bodies.
The Operation
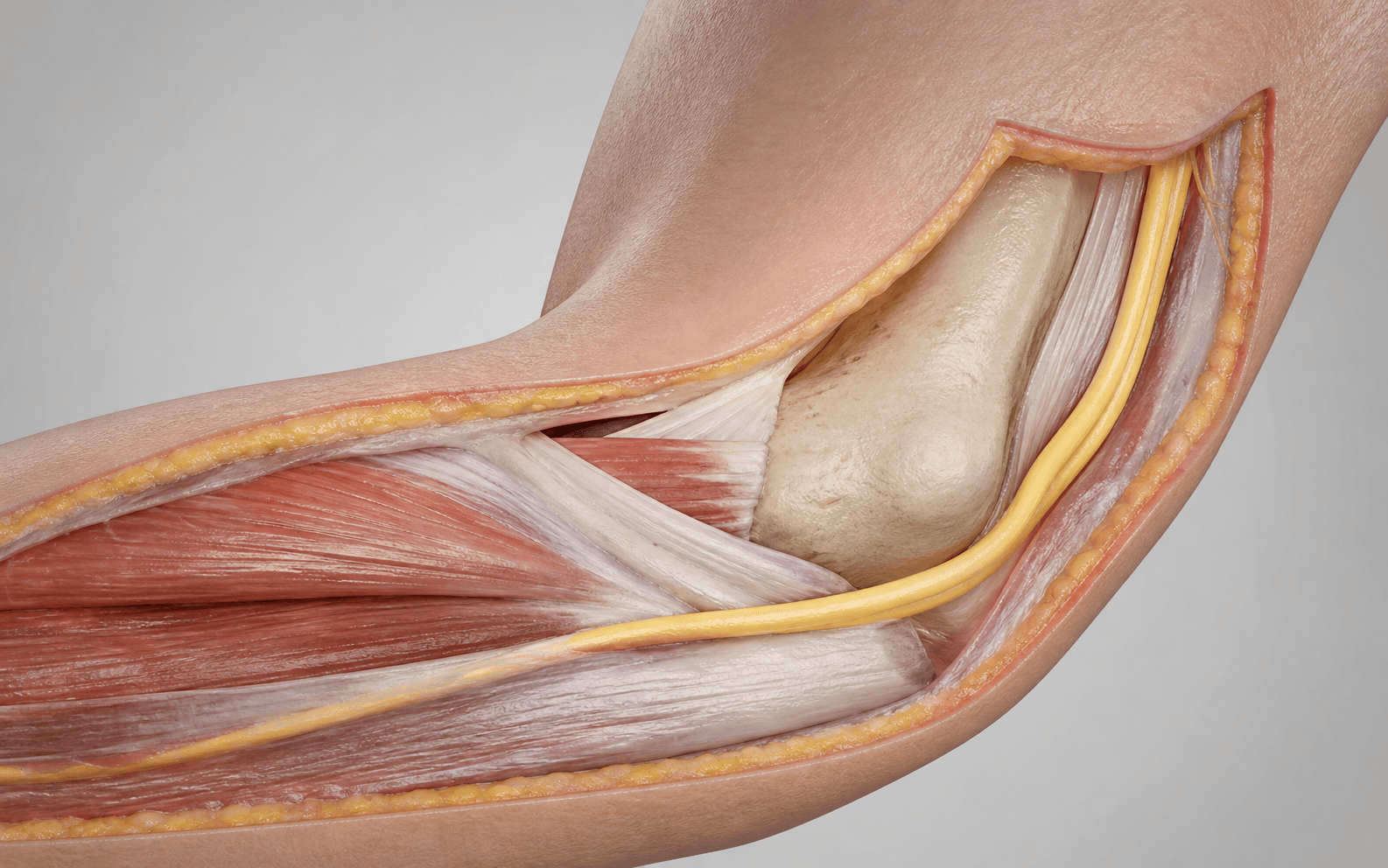
The goal: release all five sites of ulnar nerve compression from the arcade of Struthers to the flexor carpi ulnaris (FCU) heads, mobilise the nerve while preserving its blood supply, and transpose it to a tension-free bed anterior to the medial epicondyle — subcutaneous (under a fascial sling) or submuscular (the Learmonth procedure, deep to the detached and reattached flexor-pronator mass). The exposure is the Hotchkiss medial approach, laid out step by step below; identifying and protecting the nerve and its danger structures is the whole game.
Operative sequence — Hotchkiss medial approach
- Supine, arm on a hand table abducted 90 degrees, forearm supinated, elbow facing up; upper-arm tourniquet at 250 mmHg; general or regional block.
- Examine under anaesthesia: palpate the nerve in the groove, test for subluxation on passive flexion, and document range of motion and any instability.
- Make a longitudinal incision centred on the medial epicondyle, 8 cm proximal and 6 cm distal along the nerve's course, curving slightly posteriorly at the epicondyle to follow the cubital tunnel.
- Raise full-thickness skin flaps and identify the MABC in the proximal subcutaneous fat — it crosses about 2 to 3 cm anterior to the epicondyle; loop it with a vessel loop before deepening the dissection. Extend at least 8 cm proximal so the arcade of Struthers can be reached.
- Find the ulnar nerve posterior to the medial intermuscular septum in the proximal arm — a yellow-white cord running with the superior ulnar collateral artery; loop it gently.
- Dissect distally to the arcade of Struthers (a fascial band from the septum to the triceps fascia, about 8 cm proximal to the epicondyle). Pass scissors beneath it medial-to-lateral, confirm the nerve is clear, and divide it sharply under direct vision.
- Confirm the nerve is freely mobile proximal to the arcade. This is the most commonly missed compression site — the first thing to look for once the nerve is found proximally.
- Identify the septum — the thick fibrous sheet between the anterior and posterior compartments; the nerve passes through it about 2 to 3 cm proximal to the epicondyle.
- EXCISE a 2 to 3 cm window of septum with rongeurs or scissors — do NOT merely incise it. After transposition the nerve angles through the opening at almost 90 degrees; any retained edge acts as a fulcrum and kinks the nerve during flexion.
- Run a finger through the defect to confirm it is smooth and wide with no sharp edge remaining.
- Divide Osborne's ligament (the cubital tunnel retinaculum) along its full length from medial epicondyle to olecranon, exposing the nerve in the groove.
- Mobilise the nerve from the tunnel floor with gentle blunt dissection, preserving every visible vascular pedicle (vasa nervorum) and fascial attachment. Do not skeletonise the nerve circumferentially — work progressively, a few millimetres at a time, protecting any yellowish feeding vessel within a thin fascial cuff.
- Identify and preserve the articular branches (supplying the capsule and UCL) and protect the FCU motor branch (arising within or just distal to the tunnel).
- Never handle the nerve with forceps — use a vessel loop for retraction.
- Continue distally to where the nerve passes between the humeral and ulnar heads of FCU; release the aponeurotic arch connecting the two heads completely.
- Extend the release until the nerve is freely mobile with no residual tethering bands — usually 4 to 5 cm distal to the medial epicondyle.
- Subcutaneous: develop a subcutaneous pocket anterior to the epicondyle between the flexor-pronator fascia and the skin, generous enough to accommodate the nerve without tension.
- Submuscular (Learmonth): detach the common flexor-pronator origin from the medial epicondyle en masse as a single sleeve, staying in the subperiosteal plane to protect the UCL underneath; reflect it anteriorly to create a deep bed for the nerve.
- Lay the nerve smoothly in its new bed without tension, angulation or rotation.
- For a submuscular transposition, verify the nerve lies comfortably with the elbow in both full flexion and full extension before reattaching the flexor-pronator mass.
- Subcutaneous: create a fascial sling from the superficial antebrachial fascia sutured to the subcutaneous tissue on the medial side of the epicondyle — loose enough for 1 to 2 cm of nerve excursion through flexion-extension, tight enough to prevent posterior subluxation. A Z-plasty of the fascia is an alternative.
- Submuscular: reattach the flexor-pronator origin with two suture anchors (typically 5.0 mm) and/or number 2 braided suture through transosseous tunnels; confirm the repair is not so tight that it compresses the nerve against the epicondyle.
- Passively flex and extend the elbow through a full range while watching the nerve glide.
- Check for kinking at the proximal margin (residual septal edge or fascial band), kinking at the distal margin (unexcised FCU aponeurosis), subluxation back into the tunnel (inadequate sling), and compression beneath the muscle (submuscular repair too tight). Test at the extremes — subtle kinking may appear only at full flexion.
- Do NOT accept any catching or kinking. Address the cause — usually a residual septal edge proximally — and repeat until the nerve glides perfectly smoothly.
- Release the tourniquet; achieve meticulous haemostasis with bipolar diathermy (septal edges, periosteum of the epicondyle, flexor-pronator fascia). Irrigate.
- Close the deep fascia (2-0 Vicryl if opened), subcutaneous tissue (3-0 Vicryl) and skin (4-0 nylon interrupted or subcuticular).
- Apply a soft, well-padded posterior splint with the elbow at 90 degrees of flexion and the forearm in neutral rotation — not compressing the transposed nerve.
- MABC (2-3 cm anterior to the epicondyle) — laceration causes a painful neuroma worse than the original symptoms; identify and loop it early.
- Vasa nervorum — over-dissection devascularises the nerve; mobilise only as far as needed and preserve every visible feeding vessel.
- UCL (deep to the flexor-pronator origin) — stay strictly subperiosteal during the Learmonth detachment.
- FCU motor branch — division causes loss of wrist flexion with ulnar deviation.
After transposition the ulnar nerve passes through the septal opening at almost 90 degrees from its old path. A retained septal edge is the single commonest cause of persistent post-operative compression. Excise a full 2-3 cm window with rongeurs and run a finger through the defect before accepting it.
After positioning the nerve, flex and extend the elbow through full range at least three times, watching the proximal and distal transitions. Any catching or kinking — usually a residual septal edge proximally or an unexcised fascial band distally — must be corrected before closure. Never accept anything less than perfectly smooth gliding; it directly predicts the clinical outcome.
In revision surgery the cubital tunnel bed is scarred and the subcutaneous tissue is disrupted, so placing the nerve deep to the flexor-pronator mass gives it a fresh, well-padded biological cushion away from superficial scar. In throwing athletes the same deep cover best tolerates repeated valgus load — and the flexor-pronator detachment gives access for simultaneous UCL reconstruction if needed.
Aftercare & Complications
Rehabilitation. Submuscular transposition demands longer protection of the flexor-pronator repair than subcutaneous transposition.
- Subcutaneous transposition
- Posterior splint, elbow at 90 degrees, forearm neutral, 7-10 days; finger and wrist motion from day 1; elevate for the first 48 hours
- Submuscular (Learmonth)
- Posterior splint at 90 degrees for 10-14 days; finger motion from day 1; the flexor-pronator repair needs longer protection
- Subcutaneous transposition
- Splint off, active-assisted then active elbow ROM; no resisted forearm pronation or wrist flexion for 4 weeks (protects the sling)
- Submuscular (Learmonth)
- Splint off at 10-14 days, active-assisted ROM; protect the flexor-pronator repair — no resisted grip, pronation or wrist flexion for 4-6 weeks
- Subcutaneous transposition
- Progressive grip and pinch, forearm pronation-supination, wrist strengthening; gradual return to activities of daily living
- Submuscular (Learmonth)
- Same programme, begun once the repair is protected; supervised hand therapy throughout
- Subcutaneous transposition
- Full activity and non-throwing sport at 8-12 weeks
- Submuscular (Learmonth)
- Full activity at 12-16 weeks; throwing athletes at 4-6 months via a supervised throwing programme
- Subcutaneous
- 7-10 days
- Submuscular (Learmonth)
- 10-14 days
- Subcutaneous
- 4-6 weeks
- Submuscular (Learmonth)
- 6-8 weeks
- Subcutaneous
- 2-3 weeks
- Submuscular (Learmonth)
- 3-4 weeks
- Subcutaneous
- 2-4 weeks
- Submuscular (Learmonth)
- 3-5 weeks
- Subcutaneous
- 2-3 weeks
- Submuscular (Learmonth)
- 3-4 weeks
- Subcutaneous
- 8-12 weeks
- Submuscular (Learmonth)
- 12-16 weeks
- Subcutaneous
- 8-12 weeks
- Submuscular (Learmonth)
- 12-16 weeks
- Subcutaneous
- 12-16 weeks
- Submuscular (Learmonth)
- 4-6 months
Neurological recovery. Ulnar nerve regeneration proceeds at approximately 1 mm per day (roughly 1 inch per month). Sensory recovery is faster than motor: paraesthesiae typically improve within the first 3 months, and light touch and pain recover before two-point discrimination, which may never normalise in severe (McGowan grade III) disease. Intrinsic muscle re-innervation may take 6 to 18 months, and patients with pre-operative wasting may not fully recover bulk despite good re-innervation. Younger age, shorter symptom duration, milder pre-operative disease, primary (not revision) surgery and the absence of diabetes favour recovery; advanced age, symptoms over 2 to 3 years, severe wasting, revision surgery and peripheral neuropathy predict poorer recovery. Nerve conduction studies at 3 to 6 months document improving conduction velocity and CMAP amplitudes — persistent focal slowing at the transposition site suggests residual compression (kinking, inadequate release, or scar). Complications.
- Incidence
- 5-15% (higher in revision)
- Recognition
- Ongoing or recurrent paraesthesiae; persistent weakness or wasting; failure to improve after the initial post-operative recovery
- Prevention and management
- Prevention: complete release of all five sites, adequate septal excision, smooth passage verified on the sweep test. Management: nerve conduction studies at 3 months; MRI for scar or neuroma; revision with a different transposition technique if objective compression persists
- Incidence
- Uncommon — incidence uncertain
- Recognition
- Post-operative worsening worse than the pre-operative state; poor recovery of conduction velocities; new Tinel along the transposed course
- Prevention and management
- Prevention: minimise circumferential mobilisation; preserve visible vasa nervorum; mobilise only as far as necessary. Management: close clinical and neurophysiological monitoring; revision is rarely helpful — consider grafting if a devascularised segment is identified
- Incidence
- 2-5% if septal excision is incomplete
- Recognition
- Symptoms reproduced on elbow flexion; new Tinel at the proximal or distal margin; focal slowing at the transition point on nerve conduction studies
- Prevention and management
- Prevention: adequate septal excision (2-3 cm window); the intraoperative flexion-extension sweep test; smooth passage at both margins. Management: revision to release the kinking structure — usually a residual septal edge or unexcised fascial band
- Incidence
- 2-5%
- Recognition
- Burning, electric-shock pain in the medial forearm; Tinel over the antecubital region; sensory disturbance in the medial forearm
- Prevention and management
- Prevention: identify and protect the MABC early; gentle retraction with a vessel loop. Management: local anaesthetic and steroid injection; desensitisation therapy; surgical excision with proximal burial into muscle if refractory
- Incidence
- Less than 2%
- Recognition
- New or worsened intrinsic weakness; new sensory loss in the ring and little fingers; worsened two-point discrimination
- Prevention and management
- Prevention: handle the nerve only with vessel loops; never use forceps; preserve the blood supply; protect the FCU motor branch. Management: expect some temporary worsening from surgical handling; monitor with serial examinations and nerve studies; investigate for mechanical compression if no improvement by 3-6 months
- Incidence
- 5-10% (higher with submuscular)
- Recognition
- Loss of elbow extension greater than 15-30 degrees; difficulty fully extending at the first post-operative review
- Prevention and management
- Prevention: early post-operative mobilisation (within 1-2 weeks for subcutaneous; 2-3 weeks for submuscular); supervised hand therapy. Management: structured physiotherapy and progressive extension splinting; capsular release if greater than 30 degrees persists beyond 3 months
- Incidence
- Less than 2%
- Recognition
- Erythema, warmth, swelling or purulent discharge at the incision; fever; raised inflammatory markers
- Prevention and management
- Prevention: sterile technique; perioperative antibiotics for high-risk patients (diabetes, immunosuppression); meticulous haemostasis. Management: wound swab and oral antibiotics for superficial infection; washout and IV antibiotics for deep infection
- Incidence
- Rare
- Recognition
- Sudden pain and crepitus during anchor placement or rehabilitation; loss of the flexor-pronator attachment; fracture through the epicondyle on radiograph
- Prevention and management
- Prevention: use appropriately sized suture anchors for the bone quality; avoid aggressive drilling. Management: fixation of the fragment with screws; reattachment of the flexor-pronator mass; delayed mobilisation
- Incidence
- 3-5% with an inadequate sling
- Recognition
- Snapping sensation over the medial epicondyle on flexion; palpable nerve subluxation; reproduction of symptoms
- Prevention and management
- Prevention: adequate fascial sling; verify stability on the intraoperative flexion-extension sweep. Management: revision with sling reinforcement or conversion to a submuscular transposition
Special situations Revision cubital tunnel surgery. Revision after failed in-situ release is harder — scar tissue makes the nerve hazardous to identify and mobilise, the extrinsic blood supply may already be compromised, and outcomes are worse regardless of technique. The definitive revision procedure is anterior transposition, usually submuscular (Learmonth), which moves the nerve entirely out of the scarred cubital tunnel bed into a fresh, protected position deep to the flexor-pronator mass; repeat in-situ release has significantly worse outcomes. Obtain MRI and nerve conduction studies with inching first to localise persistent compression and identify scar. Counsel the patient that revision improvement rates are about 60 to 80 percent (versus 80 to 95 percent for primary transposition), recovery is slower, and complete resolution is less likely. Throwing athletes. In overhead athletes, repeated valgus stress and elbow flexion place the nerve under repetitive compression and stretch, and subluxation is common — so transposition (preferably submuscular, for the deepest cover) is preferred over in-situ release. Assess the UCL carefully: many throwers with cubital tunnel symptoms also have UCL insufficiency (the valgus-extension-overload spectrum), and the flexor-pronator detachment for a Learmonth transposition gives access for simultaneous UCL reconstruction if needed. Return to throwing follows a staged 4 to 6 month programme — flat-ground throwing at 3 to 4 months, mound throwing and competition at 4 to 6 months. Double crush (cubital tunnel plus Guyon's canal). The ulnar nerve can be compressed at both the cubital tunnel and Guyon's canal, giving mixed proximal and distal signs. Localise with nerve conduction studies; if both sites are confirmed, address the cubital tunnel (anterior transposition) and decompress Guyon's canal — anterior transposition does NOT decompress the wrist, which needs a separate incision.
Viva & Exam Focus
FOCUSFOCUS — five sites of ulnar nerve compression at the elbow
TRANSLATETRANSLATE — steps of anterior transposition
Critical danger structures and exam traps.
Location. A fascial band about 8 cm proximal to the medial epicondyle, from the medial intermuscular septum to the triceps fascia; the nerve passes beneath it before entering the cubital tunnel. The trap. The most proximal and most commonly missed compression site — if not divided, the nerve stays tethered proximally and cannot be transposed without tension. The fix. Expose the nerve at least 8 cm proximal to the epicondyle and divide the arcade under direct vision before any transposition.
The critical step. The septum is a tough fibrous sheet between the anterior and posterior compartments; the nerve passes through it just proximal to the medial epicondyle. Why excise, not incise. In its native position the nerve crosses the septum roughly perpendicular to the fibres; after transposition it angles through the opening, so any retained edge creates a sharp kink during flexion. The fix. Excise a full 2-3 cm window with rongeurs and run a finger through the defect to feel for any residual edge.
Anatomy. The nerve receives segmental feeding vessels along its course: the superior and inferior ulnar collateral arteries, the posterior ulnar recurrent artery, and the ulnar artery distal to the cubital tunnel. The risk. Aggressive circumferential mobilisation strips the vasa nervorum, devascularising a segment; post-ischaemic fibrosis produces a scarred, non-conducting nerve with worse outcomes than the original compression. The fix. Mobilise only as far as necessary; preserve visible fascial attachments and vascular pedicles; never skeletonise the nerve circumferentially.
Location. The MABC pierces the deep fascia about 2-3 cm anterior to the medial epicondyle and runs subcutaneously over the medial forearm, which it supplies. The risk. It crosses the field and is vulnerable to the incision, retractor placement and deep dissection; laceration or entrapment produces a burning, electric-shock neuroma of the medial forearm that patients find worse than their original symptoms. The fix. Identify the MABC in the proximal incision before deepening dissection; retract it gently with a vessel loop; if it must be divided (rare), bury the proximal stump in muscle.
The problem. After transposition the nerve changes direction at both ends of its new course; an acutely angulated transition or a retained structure (septal edge, fascial band) creates a sharp corner that kinks during flexion — compression worse than the original pathology. The fix. Perform the elbow flexion-extension sweep test: passively flex and extend while watching the nerve. It must glide smoothly without catching at either margin. If kinking is seen, release the tether — usually a residual septal edge, an unexcised band, or an inadequately released Osborne's ligament.
Location. One to three small articular branches leave the nerve proximal to the cubital tunnel and supply the medial elbow capsule and the UCL complex. The risk. Aggressive mobilisation divides these branches; patients develop post-operative medial elbow pain and a sense of instability on valgus stress that can be mistaken for UCL injury. The fix. Identify the branches during proximal mobilisation and preserve them where possible; if division is unavoidable, warn the patient about medial elbow discomfort that may take weeks to months to settle.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old professional baseball pitcher presents with a 6-month history of progressive paraesthesiae in the ring and little fingers of his throwing arm, worse during and after pitching. Examination reveals mild intrinsic weakness (Froment sign positive), no significant wasting, and a positive elbow flexion test at 30 seconds. Nerve conduction studies show moderate slowing across the cubital tunnel. He also reports medial elbow pain during the late cocking phase of pitching. How do you manage him?”
“A 55-year-old woman presents 18 months after an in-situ cubital tunnel decompression on her dominant hand. She had initial improvement for 6 months but now has recurrent paraesthesiae and progressive intrinsic weakness. Nerve conduction studies show persistent moderate slowing across the cubital tunnel. She works as a typist and is frustrated with the recurrence. What are your surgical options and how would you proceed?”
“You are performing an anterior subcutaneous transposition for cubital tunnel syndrome. After transposing the nerve anterior to the medial epicondyle and constructing a fascial sling, you notice that the nerve kinks at the proximal margin when you flex the elbow past 90 degrees. What has gone wrong and how do you fix it?”
Indications for transposition (over in-situ release)
- Ulnar nerve subluxation over the medial epicondyle on elbow flexion — in-situ release destabilises the nerve
- Prior medial epicondyle malunion with valgus deformity — structural abnormality of the cubital tunnel
- Revision cubital tunnel surgery after failed in-situ decompression — transposition preferred (submuscular)
- Throwing athletes — the nerve must be stabilised for repeated valgus stress and elbow flexion
- Severe disease (McGowan grade III, Dellon stage 3) with marked intrinsic wasting
Five sites of compression (FOCUS)
- F — Fascial bands / Arcade of Struthers (8 cm proximal to the medial epicondyle)
- O — Osborne's ligament / cubital tunnel retinaculum (roof of the tunnel)
- C — Cubital tunnel groove (bony floor — osteophytes, loose bodies)
- U — Ulnar nerve between the two heads of FCU (distal aponeurotic arch)
- S — Septum / medial intermuscular septum (MUST be excised, not just incised)
Surgical anatomy
- The cubital tunnel narrows by approximately 55% at full elbow flexion (Vanderpool et al.) — explains nocturnal and flexion-provoked symptoms
- Segmental blood supply: SUCA, IUCA, posterior ulnar recurrent artery, ulnar artery — preserve vasa nervorum during mobilisation
- Articular branches supply the elbow capsule and UCL — division causes post-operative medial elbow pain
- The MABC crosses the field 2-3 cm anterior to the medial epicondyle — laceration produces a painful neuroma
- The FCU motor branch arises within or just distal to the cubital tunnel — protect it to prevent wrist-flexion weakness
Technique — critical steps
- Expose the nerve 8 cm proximal to the epicondyle to release the arcade of Struthers
- Identify and protect the MABC with a vessel loop before deepening dissection
- Release all five compression sites from the arcade of Struthers to the FCU heads
- EXCISE (not incise) a 2-3 cm window of medial intermuscular septum — prevents post-transposition kinking
- Preserve vasa nervorum: minimise circumferential mobilisation, retain fascial attachments carrying vessels
- Submuscular (Learmonth): detach the flexor-pronator origin en masse, protect the UCL, reattach with suture anchors
- Subcutaneous: a fascial sling from the antebrachial fascia prevents subluxation back into the cubital tunnel
- Elbow flexion-extension sweep test: the nerve MUST glide smoothly with no kinking at either margin
In-situ vs transposition vs epicondylectomy
- In-situ decompression: simplest, lowest morbidity, for mild-moderate primary disease without subluxation
- Subcutaneous transposition: moderate complexity, fascial sling required, for subluxation and valgus deformity
- Submuscular (Learmonth) transposition: most complex, deepest cover, preferred for revision and athletes
- Medial epicondylectomy: decompresses by removing the bony ridge; risk of medial epicondyle tenderness and valgus instability
- Evidence: multiple RCTs and meta-analyses show broadly comparable outcomes for in-situ and transposition in primary disease without specific indications
Complications
- Persistent or recurrent symptoms: 5-15% (higher in revision) — complete release of all five sites is the best prevention
- Nerve devascularisation: preserve vasa nervorum — over-dissection is the biggest technical error
- Nerve kinking at the margins: incomplete septal excision is the commonest cause — the sweep test catches it intraoperatively
- MABC neuroma: 2-5% — identify and protect the MABC; produces burning medial forearm pain if injured
- Elbow stiffness: 5-10% — early mobilisation; higher rate with the submuscular technique
Post-operative rehabilitation
- Subcutaneous: splint 7-10 days, active ROM from 2 weeks, full activity at 8-12 weeks
- Submuscular: splint 10-14 days, protect the flexor-pronator repair 4-6 weeks, full activity at 12-16 weeks
- Throwing athletes: a 4-6 month staged throwing programme, mound return at 4-6 months
- Nerve regeneration: approximately 1 mm per day; motor recovery 12-18 months; sensory recovery 3-6 months
- Revision recovery is slower — counsel that improvement rates are lower than for primary surgery
Classification systems
- McGowan I: intermittent paraesthesiae, no detectable weakness; II: detectable intrinsic weakness; III: constant symptoms, marked wasting
- Dellon 1: paraesthesiae provokable by elbow flexion; 2: measurable sensory deficit; 3: constant symptoms with motor wasting
- Elbow flexion test: 60 seconds, full flexion, wrist extended — sensitivity approximately 89%, specificity approximately 99%
- Nerve conduction studies: confirm the diagnosis, grade severity, localise compression, exclude a double crush at Guyon's canal
Background & Evidence
Surgical anatomy. The ulnar nerve (C8, T1, from the medial cord) runs in the posterior compartment of the arm behind the medial intermuscular septum and anterior to the medial head of triceps. Around the mid-arm it pierces the septum into the anterior compartment, then descends on the posterior surface of the septum into the groove between the medial epicondyle and the olecranon — the cubital tunnel — before exiting between the two heads of FCU to lie deep to FCU and superficial to flexor digitorum profundus, alongside the ulnar artery. The cubital tunnel is a fibro-osseous groove: the floor is the posterior medial epicondyle and olecranon (with the UCL complex deep to it), the roof is Osborne's ligament (the cubital tunnel retinaculum, spanning the medial epicondyle to the olecranon), and the walls are the medial epicondyle and the olecranon. On elbow flexion the tunnel narrows — its volume falls by approximately 55 percent at full flexion (Vanderpool et al., cadaveric study) — and intraneural pressure rises, which is why symptoms are provoked by flexion and are often nocturnal. The arcade of Struthers, a fascial band from the septum to the triceps fascia about 8 cm proximal to the epicondyle and present in about 70 percent of specimens, tethers the nerve proximally and must be released. After transposition the nerve passes through the septal opening at a new angle, which is precisely why the septum must be excised rather than merely incised. The five sites of potential compression, with the surgical action required at each:
- Location
- About 8 cm proximal to the medial epicondyle
- What compresses
- Fascial band over the nerve
- Surgical action
- Identify and divide under direct vision
- Location
- 2-3 cm proximal to the medial epicondyle
- What compresses
- A retained septal edge constricts the transposed nerve
- Surgical action
- EXCISE a 2-3 cm window of septum
- Location
- Over the groove between the epicondyle and olecranon
- What compresses
- Tautens with flexion and narrows the tunnel
- Surgical action
- Release along its full length
- Location
- Between the epicondyle and olecranon
- What compresses
- Osteophytes, loose bodies, bony irregularity
- Surgical action
- Inspect and debride if bony pathology is present
- Location
- Between the two FCU heads (humeral and ulnar)
- What compresses
- The fascial arch over the nerve as it enters the forearm
- Surgical action
- Release the connecting aponeurosis completely
Blood supply. The ulnar nerve receives named segmental arterial branches that enter the epineurium and form longitudinal anastomoses:
- Level of contribution
- Proximal arm — accompanies the nerve in the posterior compartment
- Level of contribution
- Distal arm — via its posterior branch, anastomoses with the SUCA
- Level of contribution
- Near the cubital tunnel — sends branches to the nerve at the elbow
- Level of contribution
- Forearm — provides distal supply via multiple branches
The clinical implication is that during mobilisation the vasa nervorum entering from these arteries are at risk; the segment between the SUCA/IUCA contributions and the cubital tunnel is the most vulnerable to devascularisation because it lies between two arterial territories. Preserve visible vascular pedicles and fascial connections, and mobilise only as far as necessary. Branches at the elbow. One to three articular branches arise proximal to the cubital tunnel and supply the medial capsule, olecranon tip and UCL complex; division produces post-operative medial elbow pain and a vague sense of instability. The motor branch to FCU arises within or just distal to the tunnel (occasionally 2-4 cm proximal) and must be protected — its division causes loss of wrist flexion with ulnar deviation. The MABC (C8, T1, medial cord) crosses the field about 2-3 cm anterior to the epicondyle and supplies the medial forearm; laceration causes a painful neuroma. Surface anatomy. The medial epicondyle (the centre of the incision), the olecranon tip, the intercondylar line (about 2 cm proximal to the epicondyle, a reference for the arcade of Struthers), the nerve palpable in the groove just posterior to the epicondyle (a Tinel sign here is positive in about 70 percent of symptomatic elbows but is less specific than the elbow flexion test), and the FCU mass (the nerve exits between its heads about 2-3 cm distal to the epicondyle). Classification systems.
- Severity
- Mild
- Clinical features
- Intermittent paraesthesiae in the ulnar distribution, no measurable motor weakness, no sensory loss on testing
- Severity
- Moderate
- Clinical features
- Intermittent paraesthesiae with demonstrable intrinsic weakness (Froment sign positive), possible measurable sensory deficit
- Severity
- Severe
- Clinical features
- Constant paraesthesiae, marked intrinsic wasting and weakness, clawing of the ring and little fingers, impaired dexterity
- Severity
- Mild
- Clinical features
- Paraesthesiae provokable by the elbow flexion test; no measurable sensory loss and no motor abnormality
- Severity
- Moderate
- Clinical features
- Intermittent symptoms with a measurable sensory deficit (increased two-point discrimination or diminished light touch), mild or no weakness
- Severity
- Severe
- Clinical features
- Constant paraesthesiae, measurable motor weakness with intrinsic wasting, abnormal nerve conduction studies
Key evidence. Multiple randomised controlled trials and systematic reviews (Bartels 2005; Macadam 2008; Caliandro 2016 Cochrane; Zlowodzki 2007 AAOS meta-analysis) show broadly comparable outcomes for simple in-situ decompression and anterior transposition in primary, idiopathic disease without subluxation — with decompression offering shorter operative time and fewer early complications. Transposition is therefore reserved for its specific indications (subluxation, revision, valgus deformity, severe disease, throwing athletes). Between the transposition techniques, subcutaneous transposition is simpler and lower morbidity (the nerve sits in a subcutaneous pocket under a fascial sling), while submuscular (Learmonth) gives deeper, more secure cover beneath the detached and reattached flexor-pronator mass at the cost of more dissection and longer recovery, and is preferred for revision cases and throwing athletes. Intramuscular transposition (the nerve buried in a groove within the flexor-pronator mass) is an intermediate, less-used option with a theoretical risk of muscle scarring around the nerve.
References
Prospective randomised controlled study comparing simple decompression versus anterior subcutaneous transposition for idiopathic neuropathy of the ulnar nerve at the elbow
- Randomised controlled trial of 152 patients with idiopathic cubital tunnel syndrome
- No significant difference in clinical outcome between simple decompression and anterior subcutaneous transposition at a minimum 1-year follow-up
- Anterior transposition had a higher early complication rate including wound problems and haematoma
Simple decompression versus anterior subcutaneous and submuscular transposition of the ulnar nerve for cubital tunnel syndrome: a meta-analysis
- Meta-analysis of randomised controlled trials comparing simple decompression with anterior subcutaneous transposition
- No statistically significant difference between techniques in clinical improvement or patient satisfaction
- Simple decompression had shorter operative time and a lower early complication rate
Treatment for ulnar neuropathy at the elbow
- Cochrane systematic review and meta-analysis of surgical interventions for cubital tunnel syndrome
- Limited evidence that any one surgical technique is superior to another for most patients
- Simple decompression is associated with the fastest recovery and lowest complication rate among the techniques reviewed
Anterior transposition compared with simple decompression for treatment of cubital tunnel syndrome. A meta-analysis of randomised, controlled trials
- Meta-analysis conducted for the AAOS Clinical Practice Guideline on treatment of cubital tunnel syndrome
- Reviewed both randomised and non-randomised studies of simple decompression, anterior transposition and medial epicondylectomy
- All three techniques produced improvement in the majority of patients; evidence was insufficient to demonstrate clear superiority of one technique