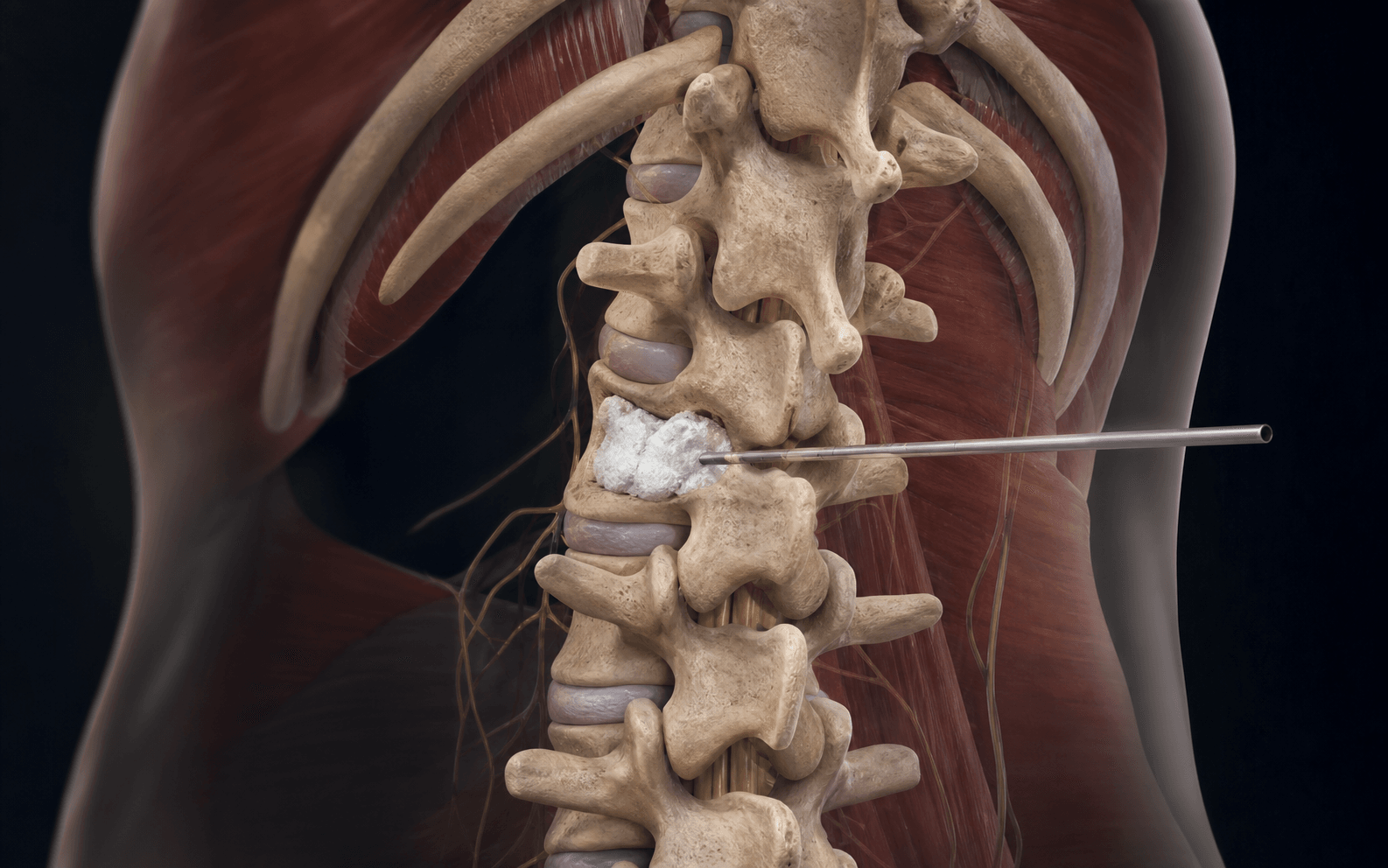
Fluoroscopically guided transpedicular PMMA cement augmentation for refractory painful vertebral compression fractures · advanced
- Patient selection is everything: focal fracture-level pain that correlates precisely with the level of marrow oedema on STIR MRI. Diffuse back pain or absence of oedema predicts a poor response and should prompt reconsideration of the procedure.
- Continuous lateral fluoroscopy during cement injection is mandatory to detect early extravasation into the epidural space, foramina or venous plexus before it becomes clinically significant. AP views alone are insufficient.
- Cement extravasation causing neural compression occurs in up to 5 percent of cases when performed without real-time monitoring; venous cement embolism to the lungs is reported in 3 to 26 percent on post-procedure CT but is usually asymptomatic.
- Sham-controlled trials (INVEST, VERTOS IV) showed no benefit of vertebroplasty over sham at 1 to 6 months for pain or function in the overall population; benefit is seen only in carefully selected patients with acute fractures less than 6 to 8 weeks old and severe focal pain.
- Inject high-viscosity, doughy PMMA only and stop the instant any posterior or lateral leak appears on lateral fluoro. Low-viscosity injection and chasing fill volume are the two behaviours that cause symptomatic leaks and embolism.
When & Why
Indication. A painful osteoporotic (or selected pathological) vertebral compression fracture with focal tenderness exactly at the fracture level, MRI confirmation of marrow oedema on STIR, and severe pain that has failed conservative care. Selection is the whole game — get it right and the procedure works; get it wrong and it offers no benefit over a sham injection. Absolute indications - Painful osteoporotic vertebral compression fracture with focal tenderness at the fracture level.
- MRI confirmation of marrow oedema (hyperintensity on STIR) at the symptomatic level.
- Failure of conservative management for more than 6 to 8 weeks with severe pain (VAS greater than 7) limiting mobilisation.
- Selected pathological fractures (myeloma, metastasis) with focal pain and no epidural tumour mass. Relative indications - Acute fracture less than 6 weeks old with severe pain where early mobilisation is critical (hospitalised, multi-morbid patients).
- Kummell disease — delayed vertebral collapse with an intravertebral cleft showing fluid signal on MRI.
- Progressive height loss or kyphosis threatening respiratory function in frail patients. Absolute contraindications - Active spinal infection (discitis, osteomyelitis, epidural abscess).
- Epidural tumour or retropulsed bone fragment causing greater than 50 percent canal compromise with neurological deficit.
- Coagulopathy that cannot be corrected (INR greater than 1.5, platelets less than 50,000).
- Allergy to PMMA cement components. Relative contraindications - Diffuse, non-focal back pain without a clear single-level correlate.
- Absence of marrow oedema on STIR MRI (a chronic fracture).
- More than three levels requiring treatment in a single session (increased cement load and leak risk).
- Severe cardiopulmonary disease precluding prone positioning. The one decision: vertebroplasty or kyphoplasty. Both work when the patient is well selected; the long-term pain and functional outcomes are equivalent. The choice turns on whether you need height restoration and how leak-averse you must be:
No cavity — cement fills the existing fracture lines. Faster (25 to 35 minutes a level), cheaper, but a higher leak rate (15 to 30 percent). The default for the frail elderly patient where the goal is rapid pain relief and mobilisation.
A balloon tamp creates a controlled cavity first, giving moderate height restoration (20 to 30 percent in acute fractures) and a lower leak rate (8 to 15 percent). More expensive and slower. Chosen when height restoration matters — greater than 30 percent height loss in a younger patient.
Consent. Quantify the risks explicitly: a 10 to 20 percent risk of cement leak (most asymptomatic), a 3 to 26 percent risk of pulmonary cement embolism on CT (usually asymptomatic), a 1 to 2 percent risk of neurological deficit requiring decompression, a 10 to 20 percent adjacent-level fracture risk, and the possibility of no pain relief at all. Setup. Prone on a radiolucent table with chest and pelvic bolsters to allow gentle extension and partial fracture reduction. Local anaesthesia with sedation (midazolam, fentanyl) is standard; general anaesthesia for anxious patients or multilevel procedures. Antibiotic prophylaxis (cefazolin 2 g IV) about 30 minutes before skin. Confirm the C-arm can reach true AP and lateral projections of the target level before you prep — if you cannot see both, do not proceed.
The Operation
The goal: drive a needle safely through the pedicle into the anterior third of the collapsed vertebral body and deposit high-viscosity PMMA under continuous lateral fluoroscopy, stopping the moment any cement tracks where it should not. The exposure is fluoroscopic, not surgical — and the pedicle is both the corridor and the cage that protects the neural structures. Relevant anatomy for transpedicular access. Thoracic pedicles (T4 to T9) are narrowest in the mediolateral dimension (4 to 6 mm) and their medial wall lies closest to the dural sac. Lumbar pedicles are larger (8 to 12 mm) and more forgiving. The pedicle axis angles 10 to 15 degrees medial in the lumbar spine and 5 to 10 degrees in the thoracic. The transverse process is the posterior landmark; the superior articular facet sits immediately lateral to the entry point. Large basivertebral veins within the body drain posteriorly through the basivertebral foramen into the epidural plexus and on into the azygos system — the main conduit for venous cement embolism, and the reason viscosity control and volume discipline matter.
Operative sequence — transpedicular vertebroplasty
- Prone on a radiolucent table; chest and pelvic bolsters allow gentle extension and partial fracture reduction. Arms tucked or abducted; head neutral in foam or Mayfield support.
- Confirm the C-arm has unobstructed access for true AP and lateral projections of the target level before prepping.
- Local with sedation is standard; general anaesthesia for anxious patients or multilevel work. Cefazolin 2 g IV about 30 minutes before skin.
- Obtain a true AP view with the vertebral endplates perfectly superimposed and the spinous process centred — this confirms correct rotation and level.
- Mark the skin entry point 1 to 2 cm lateral to the pedicle shadow (more lateral in the thoracic spine to achieve the correct medial trajectory).
- Cross-check the level on the lateral view and by palpating bony landmarks. Wrong-level injection is a never-event.
- Infiltrate skin, fascia and periosteum with 1 percent lidocaine.
- On true AP the entry point is the superolateral corner of the pedicle shadow (the 10 o'clock position on the right, 2 o'clock on the left).
- Advance an 11- or 13-gauge Jamshidi needle to engage bone.
- Once the tip engages bone, switch to a true lateral view.
- Advance in 2 to 3 mm increments, confirming on BOTH AP and lateral that the tip stays inside the pedicle silhouette at every step.
- The medial wall is the critical cortex. When the tip reaches the posterior vertebral body wall on lateral, it must still be within the pedicle on AP — only then may you enter the body.
- For a bilateral technique, repeat on the contralateral side.
- Advance 3 to 5 mm beyond the posterior wall into the anterior third of the vertebral body on lateral view — the safe fill zone.
- Remove the trocar and insert the working cannula.
- Mix PMMA to a high-viscosity, doughy consistency — thick enough to stand in a peak on the mixing bowl (typically 4 to 6 minutes after mixing). Never inject runny cement.
- Load into 1 mL syringes. High viscosity is the single biggest leak-prevention measure you control.
- Under CONTINUOUS lateral fluoroscopy, inject slowly — about 0.1 to 0.2 mL per minute.
- Watch for any posterior or lateral extravasation or venous filling. The moment you see it, STOP, leave the needle in situ 30 to 60 seconds and let the cement set to plug the leak pathway. Do not chase fill volume.
- Typical fill: 4 to 6 mL in a lumbar vertebra, 2 to 4 mL in a thoracic vertebra.
- Once the cement has set (usually 8 to 12 minutes), rotate the needle 360 degrees and withdraw slowly while the cement is still soft — to avoid pulling a cement tail into the soft tissues.
- Close the skin with adhesive strips or a single absorbable suture; apply a sterile dressing.
- Obtain a post-procedure CT (or cone-beam CT) before the patient leaves the suite to document cement distribution and detect clinically silent leaks.
- Assess lower-limb neurology and a pain score. Admit overnight for multilevel procedures or any detected leak.
- Structure at risk
- Spinal canal — the cord or cauda equina
- Structure at risk
- The exiting nerve root in the foramen
- Structure at risk
- Segmental artery and nerve root
- Structure at risk
- Aorta, vena cava or iliac vessels (especially at L4 to L5)
Low-viscosity cement injection dramatically increases extravasation risk. Never continue injecting after seeing posterior extravasation on fluoro in the hope of better fill — stop and let it set. Remember the anterior third of the body is the safe fill zone; posterior fill raises leak risk. And do not barrel through a multilevel case without pausing between levels to let each level's cement set.
Never inject cement until it is thick enough to stand in a peak on the mixing bowl. Inject under continuous lateral fluoro with your finger on the plunger, ready to stop instantly. The moment you see any posterior haze or venous filling, stop and wait 30 seconds — often the cement sets enough to plug the leak pathway. It is far better to leave the vertebra half-filled than to cause a symptomatic epidural leak.
The transpedicular route keeps the needle inside bone right up to the body, shielding the canal. Reserve the parapedicular (extrapedicular) route for narrow upper-thoracic pedicles or when instrumentation blocks the pedicle: it passes lateral to the pedicle between the rib head and body, carrying a higher risk of pneumothorax and segmental vessel injury.
Aftercare & Complications
Immediate post-procedure protocol - Bed rest for 2 hours, then mobilise as tolerated with the physiotherapist.
- Pain score and neurological observations every 4 hours for 24 hours.
- Post-procedure CT before discharge or within 24 hours.
- Analgesia: paracetamol, NSAIDs if tolerated, a short course of opioid if needed.
- Start the osteoporosis work-up and treatment before discharge (DEXA, vitamin D, calcium, an anti-resorptive or anabolic agent). Follow-up & rehabilitation - Review at 2 weeks (wound check, pain score, mobility) and again at 6 weeks.
- Physiotherapy: core stabilisation, posture re-education and gait training. Avoid heavy lifting and flexion for 6 to 8 weeks.
- Standing radiographs at 6 weeks and 3 months to monitor for adjacent fracture or progressive kyphosis.
- Long-term osteoporosis management is the single most important determinant of outcome — the procedure treats the fracture, not the underlying disease. Complications
- Recognition
- Posterior cement on lateral fluoro or post-op CT; deficit if large
- Prevention
- High-viscosity cement, slow injection, continuous lateral fluoro, stop at any posterior haze
- Management
- Small and asymptomatic: observe with serial neuro checks; greater than 50 percent canal compromise or progressive deficit: urgent laminectomy and cement removal
- Recognition
- Immediate radicular pain or weakness in the exiting nerve root
- Prevention
- Stay within the pedicle; high-viscosity cement only
- Management
- Small: nerve-root block and observe; progressive deficit: foraminotomy and cement excision
- Recognition
- Often silent and found on CT; symptomatic: dyspnoea, hypoxia, chest pain
- Prevention
- High viscosity, slow injection, watch for venous filling on fluoro, limit volume
- Management
- Supportive; anticoagulate a large central embolus; fatal embolism is rare but reported
- Recognition
- Cement in the disc space on CT
- Prevention
- Often unavoidable through a fracture line
- Management
- No specific treatment; may accelerate adjacent disc degeneration
- Recognition
- New focal pain at a neighbouring level, usually within 1 year
- Prevention
- Optimise osteoporosis therapy; counsel pre-operatively
- Management
- Analgesia and bracing; repeat augmentation only if selection criteria are met
- Recognition
- Increasing pain and inflammatory markers 2 to 8 weeks post-op
- Prevention
- Strict sterile technique; treat UTI or skin infection first
- Management
- Biopsy, targeted antibiotics, sometimes debridement
- Recognition
- Transient hypotension or, rarely, anaphylaxis during injection
- Prevention
- Have resuscitation equipment immediately available
- Management
- Supportive; standard anaphylaxis management
- Recognition
- New deficit during needle advancement
- Prevention
- True AP and lateral at every step; stay within the pedicle silhouette
- Management
- Urgent decompression if a deficit develops
Viva & Exam Focus
VERTEXVERTEX — core technical principles
LEAKSLEAKS — recognition and immediate response to extravasation
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old woman with known osteoporosis has 7 weeks of severe mid-thoracic pain after a minor fall. She localises the pain precisely to T8, VAS 8 out of 10 at rest, and struggles to mobilise. STIR MRI shows marrow oedema at T8 only. Analgesia, bracing and physiotherapy have not helped. Is she a candidate for vertebroplasty, and what specific risks would you discuss?”
“During cement injection for an L1 vertebroplasty you see, on continuous lateral fluoroscopy, a small amount of cement tracking posteriorly toward the posterior vertebral wall. The patient is awake and reports no new leg symptoms. What is your immediate response and subsequent management?”
Patient selection
- Focal fracture-level tenderness that exactly matches the pain
- MRI STIR marrow oedema at the symptomatic level is mandatory
- Fracture less than 6 to 8 weeks old with VAS greater than 7 out of 10
- Failure of conservative care for more than 6 weeks
- Selected pathological fractures without a large epidural mass
Imaging
- Pre-op: standing films plus MRI with STIR to confirm oedema and exclude other pathology
- Intra-op: true AP and lateral; needle must stay within the pedicle silhouette on both
- Continuous lateral fluoroscopy during injection is non-negotiable
- Post-op CT within 24 hours to detect silent leaks
- Absence of STIR oedema predicts poor response — do not proceed
Approach & trajectory
- Transpedicular is standard; parapedicular for narrow or blocked pedicles
- Entry point: superolateral corner of the pedicle shadow (10 o'clock right, 2 o'clock left)
- Advance in 2 to 3 mm increments, checking AP and lateral at every step
- Tip must reach the anterior third of the body before injection
- Thoracic pedicles (T4 to T9) are narrowest — highest medial-breach risk
Cement injection
- High-viscosity doughy PMMA only — low viscosity drives extravasation
- Inject slowly (0.1 to 0.2 mL/min) under continuous lateral fluoroscopy
- Volume: 4 to 6 mL lumbar, 2 to 4 mL thoracic; do not chase volume
- Stop instantly at any posterior, foraminal or venous extravasation
- Wait 30 to 60 seconds after a small leak — cement may set and seal it
Complications & aftercare
- Cement extravasation 15 to 30 percent; symptomatic neural compression about 1 percent
- Pulmonary embolism 3 to 26 percent on CT, symptomatic less than 1 percent
- Adjacent-level fracture 10 to 20 percent within 1 year
- Bed rest 2 hours then mobilise; post-op CT before discharge
- Start osteoporosis pharmacotherapy before discharge
Background & Evidence
Epidemiology. Vertebral compression fractures are the commonest osteoporotic fracture and a leading cause of pain, kyphosis and loss of independence in older adults. Most heal or settle with conservative care; vertebroplasty is reserved for the minority that remain severely and focally painful, with imaging evidence of an unhealed fracture. Why it works. Injecting PMMA into a compressed vertebral body stabilises the fractured trabeculae and reduces the micromotion that drives mechanical pain. STIR marrow oedema is the imaging correlate of an acute, unhealed, painful fracture — its presence identifies the level that will respond, and its absence means the fracture is chronic and cement will not help. The sham-trial controversy. Vertebroplasty became controversial after the 2009 sham-controlled trials (INVEST, and the Kallmes trial) showed no benefit over a sham procedure at 1 week, 1 month and 6 months for pain or function in unselected patients, with both groups improving substantially. VERTOS IV (2018) confirmed no difference versus sham at 1 and 6 months in the overall population, though its subgroup analysis suggested possible benefit in the most acute and painful fractures. The consistent lesson is that the original trials enrolled many patients with chronic fractures and diffuse pain, diluting any treatment effect; with strict selection — acute fracture, severe focal pain, clear STIR oedema — vertebroplasty gives clinically meaningful relief. This refined indication set, not the choice between vertebroplasty and kyphoplasty, is the key determinant of outcome.
- Vertebroplasty
- None — cement fills existing fracture lines
- Kyphoplasty
- Balloon tamp creates a controlled cavity
- Vertebroplasty
- Minimal (5 to 10 percent)
- Kyphoplasty
- Moderate (20 to 30 percent in acute fractures)
- Vertebroplasty
- 15 to 30 percent (higher without viscosity control)
- Kyphoplasty
- 8 to 15 percent (lower due to the cavity)
- Vertebroplasty
- 25 to 35 minutes per level
- Kyphoplasty
- 40 to 60 minutes per level
- Vertebroplasty
- Lower (no balloon kit)
- Kyphoplasty
- Higher (balloon and inflation system)
- Vertebroplasty
- Acute painful VCF with oedema, frail patient, cost-sensitive setting
- Kyphoplasty
- Greater than 30 percent height loss, younger patient, need for height restoration
References
A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures
INVEST trial: 78 patients randomised to vertebroplasty or a sham procedure. No significant difference in pain or disability scores at 1 week, 1 month or 6 months. Established the sham-controlled evidence that drove re-evaluation of patient selection criteria.
A randomized trial of vertebroplasty for osteoporotic spinal fractures
78 patients; no benefit of vertebroplasty over sham at 1 month for pain or function. Both groups improved substantially, highlighting a strong placebo effect and prompting widespread re-appraisal of indications and technique.
Vertebroplasty versus sham procedure for painful osteoporotic vertebral fractures (VERTOS IV)
VERTOS IV trial: 180 patients with acute fractures less than 6 weeks old and severe pain. No difference versus sham at 1 and 6 months in the overall population; subgroup analysis suggested possible benefit in the most acute and painful fractures.
Pulmonary cement embolism after percutaneous vertebroplasty
Retrospective review of patients with post-procedure CT. Pulmonary cement embolism detected in 4.6 percent on routine CT, all asymptomatic. Highlighted the need for post-procedure CT and awareness of the venous leak pathway.