En-bloc resection with a cuff of normal tissue and reconstruction for bone and soft-tissue sarcoma · advanced
- A WIDE margin removes the tumour surrounded by a continuous cuff of normal tissue but stays within the compartment — this is the goal for most sarcomas. A MARGINAL margin passes through the reactive zone and leaves satellite lesions; an INTRALESIONAL margin enters the tumour itself.
- Limb salvage is now achieved in 90-95% of extremity sarcomas with SURVIVAL EQUIVALENT to amputation — the landmark Rosenberg NCI randomised trial showed no overall survival difference between limb-sparing surgery plus radiotherapy and amputation.
- The biopsy tract is contaminated with tumour cells and MUST be excised en bloc with the specimen — a poorly placed or transverse biopsy can convert a salvageable limb into an amputation.
- Barrier tissues (fascia, periosteum, joint capsule, vessel adventitia) act as a thick anatomical margin — a thin cuff of intact fascia is oncologically equivalent to a much greater thickness of muscle or fat.
- “Margins are described three ways in modern practice: the Enneking system (intralesional / marginal / wide / radical), the R-classification (R0 = microscopically clear, R1 = microscopic positive, R2 = macroscopic residual), and a metric distance in millimetres qualified by the tissue at the margin.
- “Neoadjuvant chemotherapy is the standard of care for osteosarcoma and Ewing sarcoma; neoadjuvant radiotherapy improves local control in soft-tissue sarcoma and can downstage a tumour to make salvage possible.
- “Indications for amputation include unreconstructable neurovascular involvement, no viable bone or soft-tissue reconstruction, recurrent tumour after salvage, infection, failed salvage, and informed patient choice — not tumour size alone.
- “Function is reported with the Musculoskeletal Tumor Society (MSTS) score; modern endoprosthetic and allograft reconstructions achieve good functional outcomes, but reconstruction is secondary to achieving an adequate oncological margin.
When & Why
When and why you operate. Wide local excision with limb salvage is the operative goal for almost all extremity bone and soft-tissue sarcomas in which an adequate (wide) oncological margin can be obtained and a functional limb reconstructed. The single decision that matters is whether a wide margin is achievable and the limb reconstructable — not the size of the tumour or a belief that amputation buys survival. Limb salvage is now the default. Approximately 90 to 95 percent of extremity sarcomas are now treated with limb salvage rather than amputation, a shift driven by effective neoadjuvant chemotherapy, modern imaging, reconstruction options and radiotherapy. Survival is equivalent between limb-sparing surgery (with adjuvant therapy) and amputation: the landmark Rosenberg / NCI randomised trial (Rosenberg et al., 1982, Ann Surg, PMID 7114936) randomised 43 adults with high-grade extremity soft-tissue sarcoma to amputation versus limb-sparing surgery plus radiotherapy and found no difference in 5-year overall survival (88 percent amputation versus 83 percent limb-sparing) or disease-free survival, with a higher but acceptable local recurrence rate in the limb-sparing arm. On multivariate analysis the only correlate of local recurrence was a positive resection margin — confirming that the margin, not salvage versus amputation, drives local control. When amputation is indicated. Amputation is reserved for situations where an adequate (wide) margin cannot be achieved or a functional, durable limb cannot be reconstructed: - Unreconstructable neurovascular involvement — circumferential encasement of the major neurovascular bundle that cannot be resected and reconstructed
- No viable reconstruction — insufficient bone stock or soft-tissue cover to reconstruct a functional limb
- Recurrent tumour after previous limb-sparing surgery
- Infection complicating the tumour bed or a failed reconstruction (e.g. infected endoprosthesis)
- Failed limb salvage — non-union, implant failure, chronic infection rendering the limb non-functional
- Pathological fracture with widespread contamination in selected cases
- Informed patient choice — a patient may prefer a durable, single-stage amputation over a prolonged salvage pathway
- Tumour size alone — large tumours are frequently salvageable if a margin is achievable
- A single major nerve sacrifice — a limb can remain functional after sacrifice of one major motor nerve with reconstruction or orthotics
- Major vessel involvement that is reconstructable — vascular resection with bypass or interposition graft allows salvage
Neoadjuvant therapy shapes the plan. - Chemotherapy (bone sarcoma): neoadjuvant chemotherapy is standard of care for high-grade osteosarcoma and for Ewing sarcoma. It treats micrometastatic disease, allows assessment of histological response (percentage tumour necrosis) in the resection specimen — a powerful prognostic factor — and may shrink the soft-tissue component to facilitate a wide margin. A poor histological response (less than 90 percent necrosis in osteosarcoma) is associated with worse outcome.
- Radiotherapy (soft-tissue sarcoma): neoadjuvant or adjuvant radiotherapy markedly improves local control in soft-tissue sarcoma and is a cornerstone of limb-sparing strategy. Pre-operative radiotherapy uses a lower dose and smaller field (better long-term limb function and less fibrosis) but a higher acute wound complication rate; post-operative radiotherapy uses a larger field and higher dose with fewer acute wound problems — a recognised trade-off (O'Sullivan et al., 2002, Lancet, PMID 12103287; wound complications 35 percent pre-operative versus 17 percent post-operative). Radiotherapy can downstage a borderline tumour and convert an otherwise unresectable lesion into one amenable to wide local excision. Never operate before staging and MDT. Definitive surgery is never performed before complete staging and multidisciplinary review: - Local staging: MRI of the whole involved bone and adjacent joints (extent, compartment, neurovascular relationship, skip lesions)
- Systemic staging: CT chest (lungs are the commonest metastatic site), whole-body bone scan or FDG-PET
- Biopsy: image-guided core or open, longitudinal, in line with the definitive incision, performed at the treating unit
- Grade: histological grade (and for bone sarcoma the surgical stage by the Enneking/MSTS staging system) drives the margin and adjuvant plan
- Limb Salvage
- Equivalent (Rosenberg NCI RCT)
- Amputation
- Equivalent
- Limb Salvage
- Slightly higher (mitigated by radiotherapy)
- Amputation
- Lowest
- Limb Salvage
- Required — a wide margin must be obtainable
- Amputation
- Used when a wide margin is not achievable
- Limb Salvage
- Reconstructable involvement acceptable
- Amputation
- Unreconstructable circumferential encasement
- Limb Salvage
- Generally good (MSTS); depends on reconstruction
- Amputation
- Prosthetic-dependent; durable, fewer reoperations
- Limb Salvage
- Higher (implant failure, infection, nonunion)
- Amputation
- Lower long-term surgical burden
The Operation
The goal. Expose the tumour through a planned longitudinal incision, remove it en bloc with a continuous cuff of normal tissue while excising the biopsy tract, protect or reconstruct the neurovascular bundle, confirm clear margins on the specimen, and only then reconstruct the skeletal and soft-tissue defect. Achieving the oncological margin always takes priority over the reconstruction.
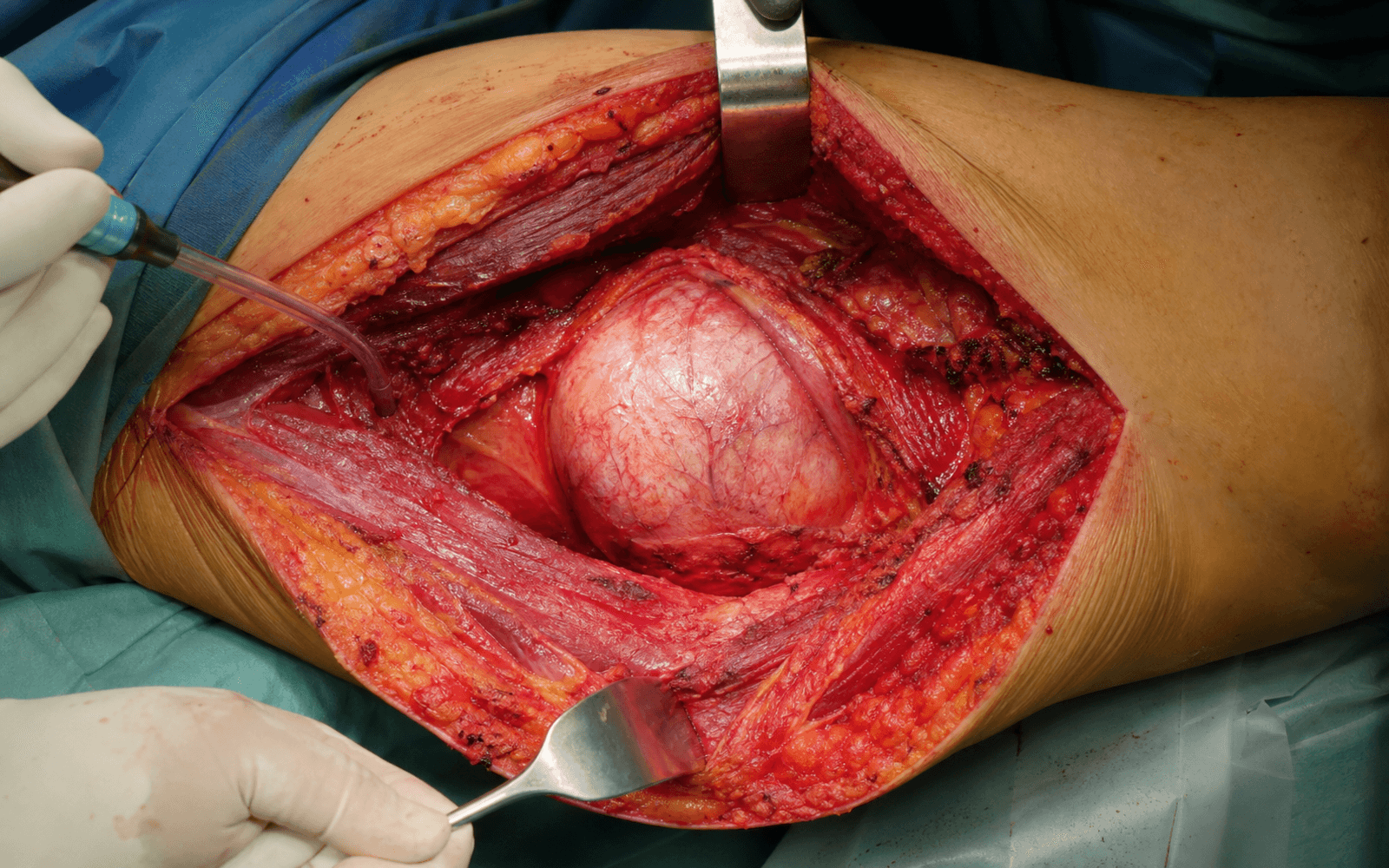
What a wide margin means in practice. You dissect in normal tissue throughout, never exposing the tumour surface, keeping a continuous cuff around the whole lesion. Where the tumour abuts a barrier such as fascia, periosteum, joint capsule or vessel adventitia, that intact layer IS the margin — a thin cuff of intact fascia is oncologically superior to a much greater thickness of fat or muscle. The full Enneking definitions (intralesional / marginal / wide / radical) and the three ways of quantifying a margin are set out in Background & Evidence below.

Operative sequence — en-bloc wide local excision
- Resection levels are planned from the staging MRI of the whole bone and adjacent joint: the compartment, neurovascular relationship, skip lesions and the biopsy tract are all mapped before incision. Reconstruction is planned in advance (implant sized, allograft ordered, plastic-surgery flap arranged).
- Position the patient to access the whole compartment and, where relevant, a flap donor site. A tourniquet may be used for distal limb work but is exsanguinated by elevation only — never by an Esmarch wrap over the tumour, to avoid mechanical tumour embolisation.
- Plan a longitudinal incision incorporating the entire biopsy tract, which is excised en bloc with an ellipse of skin. The tract is regarded as contaminated and is never separated from the specimen.
- The exposure is the whole game: a well-placed longitudinal biopsy in line with the incision lets you excise the tract with minimal extra tissue loss; a transverse or off-axis prior biopsy may force you to take far more skin, or abandon salvage.
- Entering or separating the biopsy tract from the specimen — re-contaminates the field with tumour cells
- A poorly placed prior biopsy outside the resection envelope — may make en-bloc excision and salvage impossible
- Spilling tumour from a friable soft-tissue mass — converts a wide margin into an intralesional one
- Dissect in normal tissue throughout, never exposing the tumour surface. Where possible, follow barrier planes (intact fascia, periosteum, joint capsule, vessel adventitia) which provide a robust margin with minimal tissue sacrifice.
- Plan the dissection planes to keep a continuous cuff of normal tissue around the whole tumour. The moment tumour is seen at the dissection surface, the wide-margin principle has failed and more tissue must be taken.
- Identify and protect the major neurovascular bundle proximal and distal to the tumour. If the tumour abuts but does not encase the bundle, dissect on the adventitial barrier. If a vessel is involved, plan resection and interposition or bypass grafting. A single major nerve may be sacrificed (with reconstruction or orthotic planning) if required for a clear margin.
- Dissecting onto tumour to "save" a vessel or nerve — converts a wide margin to marginal or intralesional
- Failing to recognise circumferential encasement that is unreconstructable — recognise the need to convert to amputation
- Tourniquet exsanguination by Esmarch over the tumour — risk of mechanical tumour embolisation
- Resect the bone at the pre-planned level, measured from the whole-bone MRI to clear any skip lesions with a safe margin. Send the medullary resection margin for frozen section or histology to confirm clearance — a positive marrow margin means taking more bone before reconstruction.
- For peri-articular tumours, decide between an intra-articular and an extra-articular (en-bloc joint) resection depending on joint contamination.
My bone cut level is planned from the whole-bone MRI, not from a plain film, because osteosarcoma skips. I confirm the medullary margin is clear before I reconstruct — a positive marrow margin means I take more bone.
- Deliver the specimen en bloc, orientate it with sutures or clips and ink it, so the pathologist can report margins by surface and produce an R-classification with metric distances. Communicate areas of concern (closest margin, named structures) directly to pathology.
- Reconstruct only after the margin is secured. Reconstruction (endoprosthesis, allograft, composite, vascularised graft, rotationplasty, or soft-tissue flap cover) is planned in advance and is detailed in the table below. Achieving the oncological margin always takes priority over the reconstruction.

Reconstruction options. Once a wide margin is secured, the skeletal and soft-tissue defect is reconstructed. The choice depends on the site, the size of the defect, whether the joint is sacrificed, the patient's age and growth potential, and life expectancy. An endoprosthesis gives immediate stability and early function but has a finite lifespan; an allograft (osteoarticular, intercalary, or as a prosthetic composite) is biological and restores bone stock but risks nonunion and fracture; a vascularised fibula provides living bone that hypertrophies and is valuable in irradiated or long segmental defects; rotationplasty is a durable biological option in young children.
- Best suited to
- Adult long-bone metaphyseal / articular defect
- Key advantage
- Immediate stability, early function
- Main drawback
- Finite lifespan, loosening, infection
- Best suited to
- Articular defect, young patient, bone-stock need
- Key advantage
- Biological, restores bone and attachments
- Main drawback
- Nonunion, fracture, joint degeneration
- Best suited to
- Diaphyseal defect, joints preserved
- Key advantage
- Restores bone stock, joints spared
- Main drawback
- Nonunion, slow incorporation, infection
- Best suited to
- Proximal femur / humerus / tibia
- Key advantage
- Durable joint plus tendon reattachment
- Main drawback
- Combines failure modes of both
- Best suited to
- Long segmental / irradiated defect
- Key advantage
- Living bone, hypertrophies, heals
- Main drawback
- Microsurgery, donor morbidity, slow
- Best suited to
- Young children, distal femur
- Key advantage
- Durable, biological, allows growth
- Main drawback
- Cosmetic / psychological adjustment

Aftercare & Complications
Functional outcome. Function after limb salvage is reported with the Musculoskeletal Tumor Society (MSTS) score, which rates pain, function, emotional acceptance, and (for the lower limb) support, walking and gait, or (for the upper limb) hand positioning, dexterity and lifting ability. The Toronto Extremity Salvage Score (TESS) is a complementary patient-reported measure. Modern endoprosthetic and biological reconstructions generally achieve good MSTS scores, though function is site-dependent and must be balanced against durability.
- Typical setting
- Inadequate (marginal / R1) margin; high-grade tumour
- Recognition
- New mass or pain in the resection bed; MRI shows nodular enhancement; rising activity on surveillance imaging
- Prevention and management
- Prevention: achieve a wide R0 margin; excise biopsy tract en bloc; adjuvant radiotherapy / chemotherapy. Management: re-staging, MDT review, wider re-excision or amputation, further adjuvant therapy
- Typical setting
- Especially after pre-operative radiotherapy
- Recognition
- Wound dehiscence, skin or flap necrosis, prolonged drainage in an irradiated field
- Prevention and management
- Prevention: well-vascularised flap cover, avoid tension, careful timing relative to radiotherapy. Management: debridement, vacuum dressing, free or pedicled flap reconstruction
- Typical setting
- Endoprosthesis, long operative time, immunosuppression from chemo
- Recognition
- Pain, swelling, sinus, raised inflammatory markers; positive aspirate or cultures
- Prevention and management
- Prevention: antibiotic prophylaxis, meticulous technique, silver-coated implants in selected cases. Management: DAIR versus staged revision; chronic infection of a megaprosthesis can necessitate amputation
- Typical setting
- Host-graft junction, irradiated bone, intercalary allograft
- Recognition
- Persistent pain, no bridging callus on serial radiographs at host-graft junction
- Prevention and management
- Prevention: stable fixation, bone grafting of junctions, vascularised augmentation (Capanna). Management: revision fixation and grafting, conversion to vascularised reconstruction
- Typical setting
- Endoprosthesis, high-demand or young patient over time
- Recognition
- Progressive pain, radiolucent lines, component fracture or migration on radiographs
- Prevention and management
- Prevention: correct implant selection and fixation; activity counselling. Management: revision arthroplasty / endoprosthesis exchange
- Typical setting
- Osteoarticular / intercalary allograft, irradiated field
- Recognition
- Acute pain and deformity; fracture line through the allograft on radiograph
- Prevention and management
- Prevention: protected weight-bearing, internal fixation / plate spanning. Management: ORIF, allograft revision or conversion to APC / endoprosthesis
- Typical setting
- Physeal sacrifice in a growing child
- Recognition
- Progressive discrepancy on serial scanograms
- Prevention and management
- Prevention: expandable prosthesis, rotationplasty, contralateral epiphysiodesis planning. Management: lengthening of expandable implant, equalisation procedures
Viva & Exam Focus
MARGINSMARGINS — Enneking and oncological margin principles
SALVAGESALVAGE — deciding limb salvage versus amputation
The trap: a marginal excision passes through the reactive zone (the inflammatory pseudocapsule around the tumour) and leaves behind satellite nodules and skip lesions. It looks complete to the eye but is oncologically inadequate. The fix: aim for a wide margin — a continuous cuff of normal tissue around the entire tumour and its pseudocapsule, never dissecting onto the tumour surface.
Principle: the biopsy needle or incision track is seeded with tumour cells and is part of the tumour for resection purposes. Risk: a transverse, poorly sited, or surgeon-placed biopsy outside the planned resection envelope can make en-bloc excision impossible and force amputation. Biopsy should be longitudinal, in line with the definitive incision, and ideally performed at the treating sarcoma unit.
Concept: fascia, periosteum, joint capsule, tendon and vessel adventitia resist tumour penetration and act as a thick margin. Implication: a thin but intact layer of fascia at the margin is more protective than a much larger thickness of fat or muscle. Margin adequacy must be interpreted in the context of the tissue present at the closest point.
The evidence: the Rosenberg NCI randomised trial and subsequent series show limb salvage plus radiotherapy gives the SAME overall survival as amputation, with higher local recurrence but no survival penalty. The trap: recommending amputation believing it offers a survival advantage — it does not, provided an adequate margin can be achieved by salvage.
Why it matters: osteosarcoma produces skip metastases within the same bone or across the joint. Resection planned on a localised image alone risks transecting tumour. Implication: the whole bone and adjacent joint must be imaged (MRI) before planning resection levels, and staging (chest CT, bone scan or PET) completed before any definitive surgery.
Principle: sarcoma surgery is planned by a specialist multidisciplinary team after biopsy, local staging (MRI) and systemic staging (chest CT, bone scan or PET). The trap: an unplanned excision (a "whoops" procedure) of an unsuspected sarcoma converts the bed into a contaminated field, frequently necessitates wider re-excision or radiotherapy, and worsens local control.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 16-year-old presents with a high-grade osteosarcoma of the distal femur. Staging shows no metastases. Walk me through how you decide between limb salvage and amputation, and what an adequate surgical margin means.”
“A patient is referred after an 'unplanned excision' of a thigh lump by a general surgeon that turned out to be a high-grade soft-tissue sarcoma. The biopsy was a transverse incision. Why is this a problem and how do you manage it?”
“You have resected a proximal tibial osteosarcoma in a 22-year-old and achieved a wide margin. Talk me through the reconstruction options and their trade-offs, and how you would counsel the patient on amputation as an alternative.”
Enneking surgical margins
- Intralesional: through tumour — leaves macroscopic disease (R2), debulking only
- Marginal: through reactive zone — leaves satellite / skip lesions, inadequate for high-grade sarcoma
- Wide: cuff of normal tissue all around, intracompartmental — the GOAL for most sarcomas
- Radical: whole compartment removed — maximally morbid, rarely needed
- Wide margin plus adjuvant therapy has replaced routine radical resection
Quantifying the margin
- R0 = microscopically clear; R1 = microscopic positive; R2 = macroscopic residual
- Metric margin = distance in mm, ALWAYS qualified by the tissue at the closest point
- Barrier tissues (fascia, periosteum, capsule, vessel adventitia) act as a thick margin
- A thin intact fascial cuff is oncologically superior to a thicker cuff of fat or muscle
- Orientate and ink the en-bloc specimen so pathology can report margins by surface
Staging before surgery
- Local: MRI of the WHOLE involved bone and adjacent joint (skip lesions, compartment, NV relations)
- Systemic: chest CT (commonest met site = lung), bone scan or FDG-PET
- Biopsy: longitudinal, in line with the definitive incision, at the treating sarcoma unit
- Never operate before complete staging and MDT discussion
- Avoid the unplanned 'whoops' excision — it contaminates the bed and worsens local control
Limb salvage versus amputation
- 90-95% of extremity sarcomas now salvaged
- Survival EQUIVALENT to amputation (Rosenberg NCI RCT) — salvage is the default
- Local recurrence slightly higher after salvage but no survival penalty with radiotherapy
- Amputation indications: unreconstructable NV involvement, no reconstruction, recurrence, infection, failed salvage, patient choice
- Tumour size alone, single nerve sacrifice, and reconstructable vessel involvement do NOT mandate amputation
Neoadjuvant therapy
- Chemotherapy standard for osteosarcoma and Ewing sarcoma — treats micrometastases
- Histological necrosis (less than 90% in osteosarcoma = poor response) is prognostic
- Radiotherapy improves local control in soft-tissue sarcoma and can downstage to allow salvage
- Pre-op radiotherapy: lower dose / smaller field, better function but more wound problems
- Post-op radiotherapy: larger field / higher dose, fewer acute wound problems (O'Sullivan trial)
Operative principles
- 1. Excise the biopsy tract EN BLOC with the specimen — never open into it
- 2. Dissect in normal tissue, follow barrier planes, never expose the tumour surface
- 3. Protect or reconstruct major NV bundle; reconstructable vessel involvement is salvageable
- 4. Plan bone cuts from whole-bone MRI; confirm medullary margin (frozen section)
- 5. Orientate, ink and communicate the specimen to pathology
- 6. Reconstruct only after the margin is secured — margin takes priority
Reconstruction options
- Endoprosthesis: immediate stability, early function; finite life, loosening, infection (commonest in adults)
- Osteoarticular / intercalary allograft: biological, restores bone stock; nonunion, fracture, infection
- Allograft-prosthetic composite: durable joint plus tendon reattachment (proximal femur / humerus / tibia)
- Vascularised fibula: living bone, hypertrophies, good for irradiated / long defects (Capanna with allograft)
- Rotationplasty: durable biological option in young children (distal femur), allows growth
Complications & outcomes
- Local recurrence: from inadequate margin / high grade — wider re-excision or amputation
- Wound / flap failure: especially after pre-operative radiotherapy — plan flap cover
- Periprosthetic infection: major late failure of endoprosthesis, can lead to amputation
- Nonunion / allograft fracture / aseptic loosening: revision, fixation, conversion to APC
- Function reported with the MSTS score (and TESS); proximal tibia needs gastrocnemius flap cover
Background & Evidence
Epidemiology. Approximately 90 to 95 percent of extremity sarcomas are now treated with limb salvage rather than amputation, a shift driven by effective neoadjuvant chemotherapy, modern imaging, reconstruction options and radiotherapy. Local recurrence after salvage is somewhat higher than after amputation, but with adjuvant radiotherapy and chemotherapy the difference does not translate into a survival disadvantage. Enneking surgical margins (classification). The Enneking classification defines the relationship of the plane of dissection to the tumour and its reactive (pseudocapsular) zone. It applies to both bone and soft-tissue sarcoma and underpins all sarcoma surgery. A wide margin removes the tumour, its reactive zone, and a continuous cuff of surrounding normal tissue while remaining intra-compartmental — the standard target. A radical (whole-compartment) resection is rarely required because adjuvant radiotherapy and chemotherapy supplement a wide margin for local control.
- Dissection plane
- Within the tumour
- Residue (R-class)
- R2 (macroscopic)
- Typical use
- Debulking, palliation, planned for benign curettage only
- Dissection plane
- Through reactive zone
- Residue (R-class)
- Often R1 (microscopic)
- Typical use
- Acceptable for benign / low-grade lesions, inadequate for high-grade sarcoma
- Dissection plane
- Normal-tissue cuff, intracompartmental
- Residue (R-class)
- R0 when complete
- Typical use
- Standard for most bone and soft-tissue sarcoma
- Dissection plane
- Whole compartment
- Residue (R-class)
- R0
- Typical use
- Rarely needed — extensive compartmental contamination
Quantifying the margin — three languages. - Enneking (anatomical relationship): intralesional → marginal → wide → radical, describing the dissection plane relative to the reactive zone.
- R-classification (residual disease): R0 — no residual tumour, microscopically clear margin; R1 — microscopic residual tumour at the margin (tumour cells at the inked edge); R2 — macroscopic residual tumour left in situ.
- Metric margin (distance, qualified by tissue): the closest distance from tumour to the inked specimen edge, reported in millimetres AND qualified by the tissue at that point. There is no single universally agreed threshold distance — the nature of the barrier tissue is as important as the number.
A 1 mm margin of intact fascia is oncologically superior to a 10 mm margin of fat. Barrier tissues — fascia, periosteum, joint capsule, vessel adventitia — resist tumour penetration and act as a thick margin. When reporting a margin, always state both the distance and the tissue present at the closest point.
Reactive zone and skip lesions. - The reactive zone is the oedematous, inflamed, neovascularised tissue around the tumour, containing microscopic satellite tumour nodules.
- Skip metastases are discontiguous tumour deposits within the same bone (intra-osseous skip) or across the adjacent joint (trans-articular skip) — characteristic of osteosarcoma.
- This is why the whole bone and adjacent joint must be imaged (MRI) before deciding resection levels — a localised image will miss a skip lesion and lead to an inadequate margin. Enneking / MSTS surgical staging. Sarcomas are stratified by grade (I low, II high), compartmental status (A intracompartmental, B extracompartmental) and metastasis (III). Each stage links to a recommended surgical margin, allowing protocols to be compared. Key evidence. The foundation of modern limb-salvage surgery is the Rosenberg / NCI randomised trial (1982), which established that limb-sparing surgery plus radiotherapy gives survival equivalent to amputation and identified the surgical margin as the key determinant of local control. Enneking's staging system (1980) provides the margin and staging language used worldwide. O'Sullivan and colleagues (2002) defined the radiotherapy-timing trade-off. Mankin's multicentre study (1996) showed that a poorly performed biopsy can compromise outcome, supporting biopsy at the treating unit. Bielack's analysis of 1,702 patients with osteosarcoma (2002) established histological response to neoadjuvant chemotherapy and a complete surgical margin as the dominant prognostic factors.
References
The treatment of soft-tissue sarcomas of the extremities: prospective randomized evaluations of limb-sparing surgery plus radiation therapy compared with amputation and the role of adjuvant chemotherapy
- 43 adults with high-grade extremity soft-tissue sarcoma randomised (2:1) to limb-sparing resection plus radiotherapy versus amputation; all received adjuvant chemotherapy
- No difference in 5-year overall survival (83% limb-sparing vs 88% amputation) or disease-free survival (71% vs 78%)
- Four local recurrences in the limb-sparing arm versus none after amputation, but no survival penalty
- On multivariate analysis the only correlate of local recurrence was a positive resection margin
A system for the surgical staging of musculoskeletal sarcoma
- Defines surgical margins by the relationship of the dissection plane to the tumour, its reactive zone and the compartment: intralesional, marginal, wide and radical
- Stratifies sarcomas by grade (I low, II high), compartmental status (A intracompartmental, B extracompartmental) and metastasis (III)
- Links each stage to a recommended surgical margin, allowing protocols to be compared
Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: a randomised trial
- 190 patients randomised to pre-operative (50 Gy / 25 fractions) versus post-operative (66 Gy / 33 fractions) radiotherapy
- Wound complications within 120 days were higher with pre-operative radiotherapy: 35% versus 17% (p=0.01)
- Pre-operative radiotherapy uses a lower dose and smaller field, trading early wound morbidity for better long-term function and less fibrosis
The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society
- 597 musculoskeletal sarcoma biopsies reviewed across 21 institutions; diagnostic error rate 17.8%
- A biopsy problem forced a different or more complex operation in 19.3% and changed the outcome (disability, recurrence, death) in 10.1%
- Errors, complications and adverse outcome changes were 2 to 12 times more frequent when biopsy was done at the referring institution rather than the treating centre (p less than 0.001)
Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols
- 1,702 patients with high-grade osteosarcoma; actuarial 10-year overall survival 59.8%
- Good histological response to neoadjuvant chemotherapy carried far better survival than poor response (73.4% vs 47.2%, p less than 0.0001)
- Surgical remission (macroscopically complete resection) versus incomplete resection: 64.8% vs 14.6% survival
- Surgical margin / completeness and histological response emerged as the dominant prognostic factors on multivariate analysis