Portal Anatomy | Palmer TFCC Classification | Geissler SL Grading | TFCC Repair vs Debridement | Ganglion Decompression | advanced
- 3-4 portal is the standard VIEWING portal — between EPL (3rd compartment) and EDC (4th compartment), ulnar to Lister's tubercle
- Palmer Class 1B = TFCC foveal avulsion — REPAIRABLE (arthroscopic or open repair). Class 1A = central perforation — DEBRIDEMENT ONLY (avascular zone)
- Geissler Grade III to IV scapholunate instability requires surgical intervention — Grades I to II are managed conservatively
- Traction: 5 to 10 lb (2 to 4 kg) through finger traps on index and middle fingers, 1.9 mm or 2.4 mm arthroscope
- “EPL rupture is the most feared complication of wrist arthroscopy — EPL enters 3-4 portal immediately; retract it before portal insertion
- “TFCC central perforations (1A) cannot be repaired — the central disc is avascular; debridement is the only option
- “Midcarpal portals (MCR, MCU) are essential for SL and LT ligament assessment — radiocarpal portals alone are insufficient
- “Ganglion stalk from SL interval is visualised directly through 3-4 portal and decompressed arthroscopically without open incision
When & Why
What it is. Wrist arthroscopy provides diagnostic and therapeutic access to the radiocarpal and midcarpal joints with minimal soft-tissue morbidity. Osterman first established the technique for TFCC diagnosis and treatment in 1990, and it has since become the gold standard for assessing intrinsic carpal ligament injuries and TFCC tears — it is both the definitive diagnostic test and a treatment platform in the same setting. Established indications. 1. TFCC injuries (Palmer Class 1, traumatic).
- Class 1B foveal avulsion: arthroscopic repair to the fovea is first-line treatment
- Class 1A central perforation: arthroscopic debridement to a stable rim
- Ulnar impaction syndrome (Class 2C to 2E): arthroscopic debridement with or without ulnar shortening osteotomy
- Diagnosis of ulnar-sided wrist pain refractory to conservative management 2. Scapholunate (SL) ligament injuries.
- Geissler Grade III to IV: arthroscopic assessment guides treatment (K-wire stabilisation, open SL repair)
- Gold standard for dynamic instability staging — superior to MRI for functional assessment
- Assessment before planned SL reconstruction 3. Dorsal ganglion decompression.
- Recurrent ganglion after aspiration
- Patient preference for a smaller incision
- Ganglion stalk visualised and decompressed from the SL interval through the 3-4 portal
- Recurrence 20 to 30 percent arthroscopic versus 5 to 10 percent open — counsel patients pre-operatively 4. Loose body removal.
- Post-traumatic loose bodies in the radiocarpal or midcarpal compartments
- Synovial osteochondromatosis of the wrist 5. Adjunctive and other procedures.
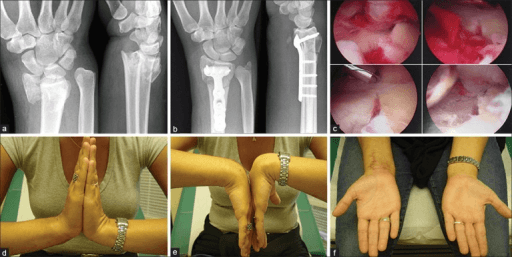
- Distal radius fracture assessment — concurrent arthroscopy confirms articular reduction (arthroscopic-assisted fixation)
- Lunotriquetral ligament injuries
- Radiocarpal joint synovectomy (rheumatoid arthritis) Diagnostic accuracy — why arthroscopy wins. Wrist arthroscopy remains the gold standard for intrinsic ligament and TFCC assessment. Compared with other modalities: | Modality | SL Tear Sensitivity | TFCC Tear Sensitivity | Limitations | |---------|--------------------|-----------------------|-------------| | Plain X-ray | Poor (only detects established SLAC) | Not visible | Only static bony alignment | | MRI (non-arthrogram) | 57 to 78 percent | 60 to 75 percent | Operator dependent; small ligaments near resolution limit | | MR arthrogram | 79 to 88 percent | 84 to 92 percent | Invasive (intra-articular injection); best non-arthroscopic test | | CT arthrogram | 75 to 85 percent | 80 to 90 percent | Radiation, invasive | | Wrist arthroscopy | Near 100 percent (gold standard) | Near 100 percent (gold standard) | Invasive, requires anaesthesia and theatre | For exam candidates: MR arthrogram is the best pre-operative investigation before wrist arthroscopy for suspected TFCC or SL injury. Arthroscopy then provides the definitive diagnosis and allows concurrent treatment. Pre-operative workup. All patients undergoing arthroscopy for ligament or TFCC pathology should have:
- Weight-bearing AP and lateral wrist X-ray (assess carpal alignment, SL gap, DISI)
- Ulnar variance measurement (positive variance suggests ulnar impaction, relevant to degenerative TFCC disease)
- MR arthrogram (best pre-operative imaging for soft-tissue structures)
- Clinical examination: fovea sign (ulnar-sided TFCC foveal avulsion), scaphoid shift test (SL instability), DRUJ stress test Consent specifically for EPL rupture (the signature complication, less than 1 percent), dorsal sensory radial or ulnar nerve injury (numbness or neuroma), post-operative stiffness, infection, fluid extravasation, and — for ganglion decompression — a 20 to 30 percent recurrence rate (higher than open excision). Setup. Supine, shoulder adducted, arm on a board or in a traction tower; upper-arm tourniquet to 250 mmHg. Apply finger traps to the index and middle fingers and 5 to 10 lb (2 to 4 kg) of longitudinal traction, which opens the radiocarpal joint to a working space of about 3 to 4 mm. Keep total traction time under 90 minutes to avoid nerve injury.
The Operation
The goal: safely establish the dorsal portals around the extensor tendons, inspect the radiocarpal and then the midcarpal joint systematically, grade any SL or TFCC injury, and perform the indicated procedure — debridement, repair, ganglion decompression or loose-body removal — while protecting the EPL, the dorsal sensory nerves and the joint surfaces. The exposure is the portals: getting them right, in the right order, is the whole game.
Operative sequence
- Supine, arm on a board or in a vertical traction tower; upper-arm tourniquet to 250 mmHg; exsanguinate with Esmarch or arm elevation.
- Finger traps to index and middle fingers (ring and little fingers for some ulnar-sided procedures); apply 5 to 10 lb (2 to 4 kg) of longitudinal traction to open the radiocarpal joint.
- Before draping, mark the landmarks: Lister's tubercle (3rd compartment, EPL), radial styloid, ulnar styloid, the ECU tendon groove, and every planned portal site.
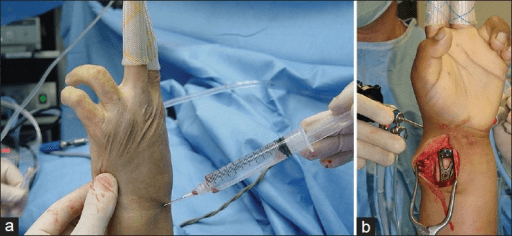
- Insert a 21-gauge needle at the planned 3-4 portal site with the wrist in traction.
- Inject 5 to 8 mL of saline into the radiocarpal joint. Backflow of clear saline into the syringe when the piston is released confirms intra-articular placement.
- This distension confirms anatomy, creates working space, and lifts soft tissues away from the trocar.
- Stab incision through skin only at the 3-4 site (between EPL and EDC, just ulnar to Lister's tubercle). Use a curved mosquito or blunt trocar with gentle spreading down to the extensor retinaculum — this protects the EPL from inadvertent laceration.
- Enter the radiocarpal joint with a 1.9 mm or 2.4 mm blunt trocar directed about 10 degrees proximally (toward the forearm).
- Connect the arthroscope to fluid (gravity or low-pressure pump) and the camera. Confirm intra-articular position by identifying the distal radius articular surface and the proximal carpal row.
- The EPL tendon passes directly beneath this portal — identify and retract it before trocar insertion (see the safety alert below).
- Under direct arthroscopic vision through the 3-4 portal, insert a 21-gauge spinal needle at the planned 4-5 site (between EDC and EDM). Confirm position on the monitor as the needle enters the joint.
- Stab the skin and pass a blunt trocar into the radiocarpal joint under vision.
- This portal gives access to the TFCC, the SL interval from the radiocarpal side, and is used for the probe and working instruments.
- Insert an 18-gauge needle at the 6R portal (radial to the ECU tendon) for outflow or a second instrument.
- This portal also allows TFCC viewing from the ulnar side and is used for suture passage in TFCC repair.
- Reserve the 6U portal (ulnar to ECU) for outside-in TFCC repair suture passage — it carries the highest dorsal sensory ulnar nerve risk.
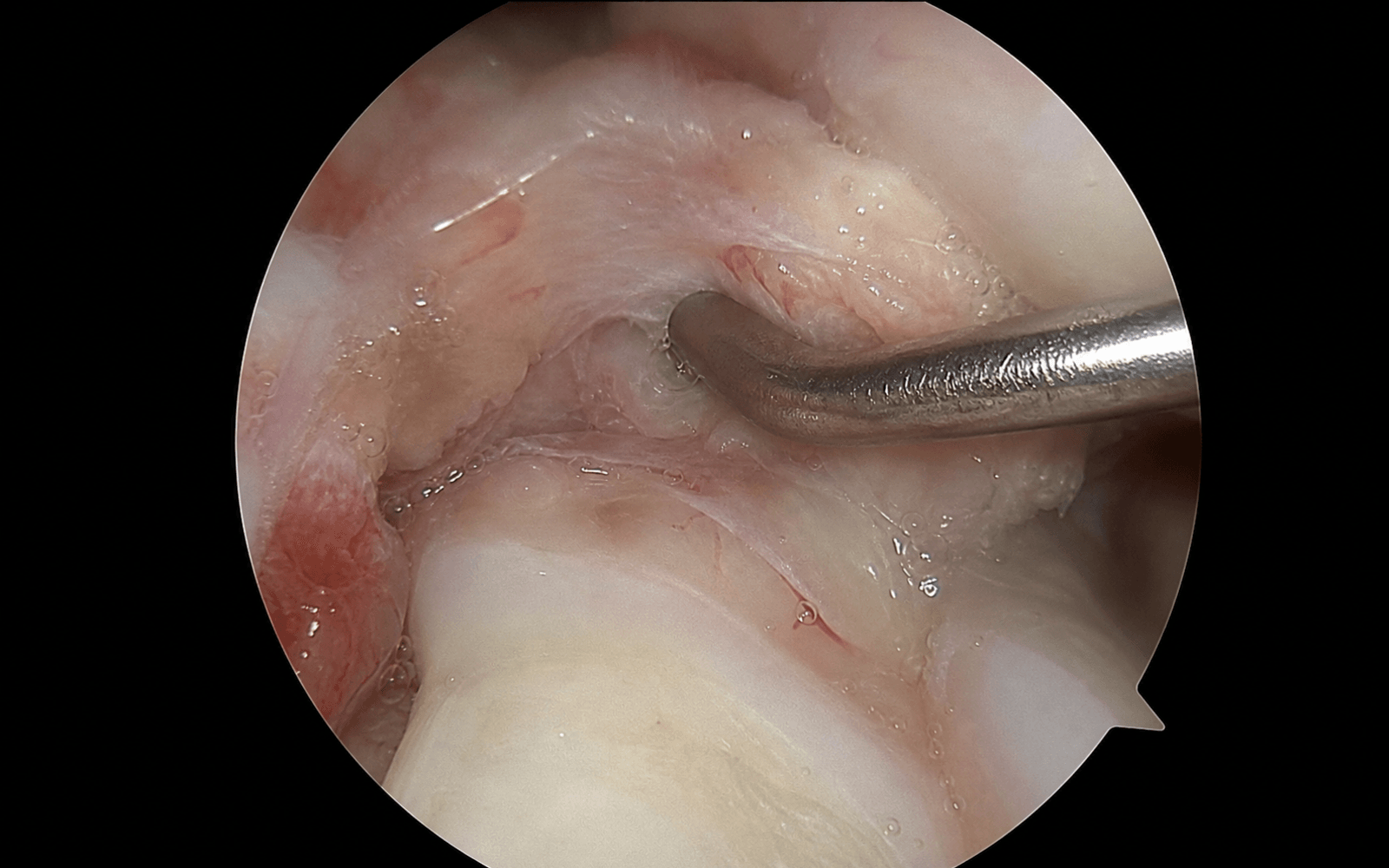
- Follow a fixed sequence so nothing is missed: 1. Distal radius articular surface — radiocarpal cartilage, lunate fossa, sigmoid notch 2. Scaphoid proximal pole — cartilage quality, SL interval from the radiocarpal side 3. Lunate — articular surface; proximal surface of the SL ligament visible 4. TFCC — central disc integrity; probe to assess stability; peripheral margins 5. Radial extrinsic ligaments — radioscaphocapitate (RSC), long and short radiolunate 6. Lunotriquetral interval — probe from the 4-5 portal 7. DRUJ compartment if a TFCC tear is present — probe through the tear to assess DRUJ stability
- Switch the scope to, or establish, the midcarpal radial (MCR) portal (1 cm distal to the 3-4 portal) and use the midcarpal ulnar (MCU) portal (1 cm distal to the 4-5 portal) for the probe.
- The midcarpal joint shows the distal surfaces of the SL and LT ligaments directly — Geissler grading of SL instability is performed here, not from the radiocarpal side.
- Insert the probe from the MCU portal into the SL interval and grade the instability (see the Geissler table in Background and Evidence): Grade I haemorrhage or attenuation with no step-off; Grade II a step-off with the probe tip entering but not passing through; Grade III a 1 mm probe passing freely across the joint; Grade IV the 2.7 mm arthroscope itself passing across (gross instability).
- TFCC debridement (Class 1A): insert a motorised shaver (2.0 to 2.9 mm) through the 4-5 portal; trim the central disc tear to stable margins; resect unstable flaps; probe confirms a stable rim at completion; preserve all peripheral TFCC tissue.
- TFCC foveal repair (Class 1B), outside-in: confirm the foveal avulsion from 3-4 viewing and 6R probe palpation (the TFCC is detached and lax); pass a suture needle through the 6U portal, through the peripheral TFCC, and out the ulnar capsule; pass a permanent suture (0-PDS or 2-0 Fiberwire); make a small 1 cm open incision at 6U, protect the dorsal sensory branch of the ulnar nerve, and tie the sutures over the ECU subsheath to re-attach the TFCC to the fovea.
- Ganglion decompression: identify the capsular swelling or stalk origin at the SL interval from the 3-4 portal; use a motorised shaver or radiofrequency probe through the 4-5 portal to excise the capsule at the stalk base — the ganglion contents deflate externally; ensure complete stalk excision to the SL interval; no external incision is required.
- Remove instruments under vision; release traction.
- Skin closure with a single suture or steri-strips per portal; the small stab incisions rarely need deep closure.
- Bulky dressing; splint or cast as dictated by the procedure performed.
Portal reference — radiocarpal. All portals are named by their position relative to the dorsal extensor compartments (numbered 1 radial to 6 ulnar). | Portal | Location | Primary use | Key hazard | |--------|----------|-------------|------------| | 3-4 | Between EPL (3rd) and EDC (4th), ulnar to Lister's tubercle | Primary viewing — radiocarpal | EPL directly beneath (retract before insertion); dorsal sensory radial nerve superficially | | 4-5 | Between EDC (4th) and EDM (5th) | Working — TFCC access, SL probing | EDM tendon and terminal posterior interosseous nerve branch | | 6R | Radial side of ECU (6th) | Outflow — TFCC viewing | Dorsal sensory branch of ulnar nerve | | 6U | Ulnar side of ECU | TFCC repair (outside-in suture passage) | Dorsal sensory branch of ulnar nerve — most at risk here | Portal reference — midcarpal. | Portal | Location | Primary use | Key hazard | |--------|----------|-------------|------------| | MCR (radial) | 1 cm distal to the 3-4 portal, scaphocapitate interval | Viewing the midcarpal joint — SL ligament distal surface | Dorsal sensory radial nerve branches | | MCU (ulnar) | 1 cm distal to the 4-5 portal, capitate-hamate / triquetrum-hamate interval | Working midcarpal — LT ligament, hamate | Dorsal sensory branch of ulnar nerve | Portal surface anatomy — key measurements.
- 3-4 portal: 1 cm distal and 1 cm ulnar to Lister's tubercle
- 6R portal: immediately radial to the palpable ECU tendon
- MCR portal: 1 cm distal to the 3-4 portal, in the scaphocapitate interval


The EPL tendon at Lister's tubercle passes directly beneath the 3-4 portal and is the most at-risk tendon in wrist arthroscopy; EPL rupture is the signature, most feared complication (less than 1 percent). Prevent it at every 3-4 portal: make the skin incision only, then spread bluntly down to the retinaculum; identify and retract the EPL before trocar insertion; use a blunt trocar only; never run a motorised shaver or radiofrequency probe near the portal entry. Loss of thumb IP extension after arthroscopy is an EPL injury until proven otherwise — disclose it promptly (duty of candour), re-explore within 24 to 48 hours, and repair primarily (modified Kessler) or reconstruct with an EIP-to-EPL transfer.
The 3-4 portal sits in the internervous soft spot between EPL (posterior interosseous nerve, 3rd compartment) and EDC (also PIN, 4th compartment), just ulnar to Lister's tubercle. It gives the straightest line of sight across the radiocarpal joint to the scapholunate interval and lunate fossa, which is why it is established first and used for viewing throughout.
Geissler grading is performed from the midcarpal portal (MCR viewing, MCU probing), looking at the distal surface of the SL joint — never from the radiocarpal side. If you only use radiocarpal portals you will under-grade dynamic SL instability. Always establish MCR and MCU when SL injury is in question.
Aftercare & Complications
Post-operative protocols by procedure. | Procedure | Immobilisation | Rehabilitation | Return to activity | |-----------|----------------|----------------|--------------------| | Diagnostic arthroscopy | Soft dressing 48 h | Active wrist and finger ROM within 3 to 5 days; sutures out at 10 days | 2 to 4 weeks | | TFCC debridement (1A) | Short-arm splint 2 weeks | ROM from 2 weeks; strengthening from 6 weeks | 6 to 8 weeks | | TFCC foveal repair (1B) | Long-arm cast or above-elbow splint 4 to 6 weeks | Wrist ROM at 6 weeks; strengthening from 3 months | 4 to 6 months | | SL stabilisation (K-wires, Geissler III to IV) | Long-arm thumb spica 8 weeks with K-wires in situ | Remove K-wires at 8 weeks under fluoroscopy; graduated ROM; strengthening from 12 weeks | 4 to 6 months | | Arthroscopic ganglion | Soft dressing, no splint | ROM from day 2 to 3 | 2 to 3 weeks | Outcomes by procedure. | Procedure | Good to excellent | Return to activity | Recurrence or reoperation | |-----------|-------------------|-------------------|--------------------------| | TFCC 1A debridement | 80 to 90 percent | 6 to 8 weeks | 5 to 10 percent | | TFCC 1B foveal repair | 75 to 85 percent | 4 to 6 months | 10 to 15 percent | | SL K-wire stabilisation | 60 to 70 percent (Grade III) | 4 to 6 months | 20 to 30 percent (residual instability) | | Arthroscopic ganglion | 80 percent symptom relief | 2 to 3 weeks | 20 to 30 percent recurrence | | Loose body removal | 85 to 95 percent | 4 to 6 weeks | Rare | Complications.
- Mechanism
- EPL passes directly beneath the 3-4 portal — trocar or shaver injury; delayed rupture from thermal injury (radiofrequency probe)
- Prevention
- Blunt trocar only at the 3-4 portal; identify and retract EPL before insertion; avoid radiofrequency near EPL; blunt spread technique at portal entry
- Management
- Duty of candour and document; re-explore within 24 to 48 h; primary repair (modified Kessler) if recognised; EIP-to-EPL transfer if repair not feasible; splint thumb IP in extension 6 weeks
- Mechanism
- Superficial radial nerve branches cross the 3-4 and MCR portal sites in subcutaneous tissue; stab incision or thermal injury
- Prevention
- Skin incision only, then blunt spread to retinaculum; no cautery near portals; plan portal sites on landmark anatomy
- Management
- Neuropraxia resolves 6 to 12 weeks; neuroma — desensitisation, gabapentin; persistent symptomatic neuroma — excision and nerve burial
- Mechanism
- At risk during 6U and MCU portal creation; the dorsal sensory branch of the ulnar nerve crosses the ulnar wrist
- Prevention
- Blunt portal technique at 6U and MCU; skin incision only then blunt spread; palpate ulnar styloid to orient; consider 6R over 6U for outflow
- Management
- Same as radial nerve injury; the 6U portal has the highest ulnar nerve risk — protect the nerve during suture retrieval
- Mechanism
- Post-arthroscopy adhesions, capsular scarring, inadequate rehabilitation
- Prevention
- Early active ROM within 3 to 5 days; avoid immobilisation beyond 10 to 14 days; formal hand therapy if ROM not improving by 3 weeks
- Management
- Hand therapy (active and passive ROM); NSAIDs; if persistent at 3 months reassess for missed pathology (retained loose body, recurrent TFCC tear)
- Mechanism
- Portal-site superficial infection or deep septic arthritis
- Prevention
- Single-dose pre-operative antibiotic (cephazolin); sterile technique; avoid irrigation pump overload; tourniquet on to limit fluid extravasation
- Management
- Superficial — oral antibiotics; septic arthritis — arthroscopic washout plus IV antibiotics plus culture-directed therapy
- Mechanism
- High-pressure irrigation pump forces fluid into forearm soft tissues; risk rises with procedure duration and pump pressure
- Prevention
- Use gravity irrigation or a low-pressure pump (less than 40 mmHg); keep the procedure under 90 minutes; monitor forearm compartments; tourniquet limits proximal migration
- Management
- Minor — resolves with elevation over 24 to 48 h; severe swelling — check compartment pressures (compartment syndrome from extravasation is rare but documented)
EPL rupture after wrist arthroscopy — in detail. This deserves special attention as the classic exam question. The EPL at Lister's tubercle passes directly beneath the 3-4 portal. Mechanisms of injury: (1) direct laceration from the trocar at portal establishment; (2) thermal injury from a radiofrequency probe near the portal; (3) shaver injury if the instrument strays from the intra-articular position; (4) delayed rupture from compromised vascularity — rare. Recognition. Loss of IP joint extension of the thumb, usually presenting at the post-operative assessment (day 1 to 14) rather than immediately, unless transection was recognised intra-operatively. Management.
- If transection is recognised intra-operatively: direct repair (4-0 braided suture, modified Kessler core plus epitendinous).
- If delayed: EIP-to-EPL tendon transfer (extensor indicis proprius re-routed to the EPL distal stump — EIP is expendable as EDC to the index remains for extension).
- Immobilise the thumb IP joint in extension for 6 weeks after repair or transfer, with dynamic extension splinting from 4 weeks to allow tendon gliding.
Viva & Exam Focus
PALMERPALMER — TFCC Classification (Class 1 Traumatic)
PORTALPORTAL — Wrist Arthroscopy Setup Sequence
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old recreational tennis player sustained a forced ulnar deviation injury to the right wrist 6 months ago. She has persistent ulnar-sided wrist pain, a positive ulnar fovea sign, and pain with DRUJ stress testing. MRI arthrogram shows a TFCC peripheral avulsion at the fovea. She has failed 3 months of splinting. Describe your arthroscopic management.”
“You are performing wrist arthroscopy for suspected SL instability in a 32-year-old who fell on an outstretched hand 8 weeks ago. Radiocarpal inspection through the 3-4 portal shows a widened SL interval. You then insert the arthroscope into the midcarpal radial portal and can pass the 2.7 mm arthroscope itself through the SL interval from the distal side. What is the Geissler grade and what are your management options?”
“You are performing routine diagnostic wrist arthroscopy through the 3-4 portal with a motorised shaver. At the end of the procedure you release and deflate the tourniquet. Post-operatively the patient cannot extend the IP joint of their thumb. What has happened and how do you manage this?”
Portal anatomy summary
- 3-4 portal: PRIMARY viewing — between EPL (3rd) and EDC (4th), ulnar to Lister's tubercle; EPL directly beneath
- 4-5 portal: PRIMARY working — between EDC (4th) and EDM (5th); access to TFCC and SL probing
- 6R portal: radial side of ECU; outflow plus TFCC viewing; dorsal ulnar nerve risk
- 6U portal: ulnar side of ECU; TFCC outside-in repair suture passage; HIGHEST ulnar nerve risk
- MCR (radial midcarpal): 1 cm distal to the 3-4 portal; viewing SL and the midcarpal joint
- MCU (ulnar midcarpal): 1 cm distal to the 4-5 portal; LT ligament and hamate assessment
Palmer TFCC classification — must know
- Class 1A: central perforation (horizontal tear) — AVASCULAR — DEBRIDEMENT ONLY
- Class 1B: ulnar foveal avulsion — VASCULAR (peripheral) — REPAIRABLE (outside-in or inside-out)
- Class 1C: distal carpal avulsion (ulnocarpal ligaments)
- Class 1D: radial avulsion from the sigmoid notch — DRUJ instability risk
- Class 2A to 2E: degenerative (ulnar impaction) — progressive TFCC wear, LT tear, chondromalacia
- Key exam distinction: 1A = debridement, 1B = repair; location determines biological capacity
Geissler SL grading — assessed from the midcarpal portal
- Grade I: haemorrhage or attenuation, no step-off — conservative management
- Grade II: step-off, probe tip enters the SL interval but does not pass through — consider splinting or K-wires
- Grade III: 1 mm probe passes freely across the SL joint — surgical stabilisation (K-wires or open repair)
- Grade IV: 2.7 mm arthroscope passes across the SL interval — GROSSLY UNSTABLE — open SL repair or K-wire stabilisation mandatory
- Midcarpal portals (MCR and MCU) are ESSENTIAL for Geissler grading — radiocarpal portals alone are insufficient
Setup and traction
- Traction: 5 to 10 lb (2 to 4 kg) through finger traps on index and middle fingers
- Scope: 1.9 mm or 2.4 mm for the radiocarpal joint; 2.7 mm acceptable in the midcarpal joint
- Distend the radiocarpal joint with 5 to 8 mL saline before 3-4 portal insertion — confirms position and creates space
- Arm suspended vertically (tower) or horizontal (arm board) — both acceptable
- Tourniquet to 250 mmHg limits fluid extravasation into forearm soft tissues — keep it on throughout
TFCC repair technique — outside-in (1B foveal)
- Establish 3-4 viewing, 4-5 working, 6U for repair needle passage
- Confirm foveal avulsion with a probe at the 6U portal — TFCC detached and lax
- Pass a curved suture needle through the 6U portal, pierce the peripheral TFCC, exit the ulnar capsule
- Pass 0-PDS or 2-0 Fiberwire through the TFCC — two sutures minimum
- Small 1 cm open incision at 6U — identify and protect the dorsal sensory ulnar nerve
- Tie sutures over the ECU subsheath — re-attaches the TFCC to the foveal region
- Post-op: LONG-ARM cast 4 to 6 weeks (protects from forearm rotation stress)
Complications — key facts
- EPL rupture: MOST FEARED — EPL beneath the 3-4 portal; prevent with a blunt trocar only and retract the EPL before insertion
- Management of EPL rupture: duty of candour, re-explore within 24 to 48 h, primary repair versus EIP-to-EPL transfer
- Dorsal sensory radial nerve: at the 3-4 and MCR portals; blunt technique; 5 to 8 percent minor injury
- Dorsal sensory ulnar nerve: at the 6U portal (highest risk); blunt technique; protect during suture retrieval
- Fluid extravasation: use gravity irrigation or a low-pressure pump; monitor forearm swelling
- Arthroscopic ganglion recurrence: 20 to 30 percent versus open 5 to 10 percent — counsel patients pre-operatively
Post-op protocols
- TFCC debridement (1A): 2-week splint, ROM from 2 weeks, full activity 6 to 8 weeks
- TFCC foveal repair (1B): LONG-ARM cast 4 to 6 weeks, ROM from 6 weeks, full activity 4 to 6 months
- SL K-wire stabilisation: long-arm thumb spica 8 weeks with K-wires in situ
- Arthroscopic ganglion: soft dressing only, ROM day 2 to 3, return to activity 2 to 3 weeks
- Diagnostic arthroscopy: ROM within 3 to 5 days, full activity 2 to 4 weeks
Background & Evidence
The TFCC and its blood supply. The triangular fibrocartilage complex is the primary stabiliser of the distal radioulnar joint (DRUJ) and the ulnar carpus. It comprises the articular disc (the central fibrocartilage between the ulna and the proximal carpal row — an avascular central zone), the dorsal and volar radioulnar ligaments (peripheral bands with a good blood supply — repairable), the ulnocarpal ligaments (ulnolunate and ulnotriquetral, the distal stabilisers), and the ECU subsheath and meniscus homologue at the ulnar margin. The critical biological point: the central TFCC (articular disc) has no direct vascular supply, so repair will not heal — debridement only. The peripheral 15 to 20 percent of the TFCC, especially the foveal attachment, receives blood from ulnar artery branches — repair in this zone is biologically sound. This single fact underpins the entire Palmer 1A-versus-1B decision. Scapholunate ligament anatomy for Geissler grading. The SL ligament has three portions: the dorsal SL (the thickest at about 3 mm and the strongest — the primary restraint to scaphoid flexion), the proximal (membranous) portion (a thin fibrocartilaginous central zone), and the volar SL (an oblique ligament, a secondary stabiliser). Geissler grading is assessed from the midcarpal portal, viewing the dorsal SL interval from the distal side.
- Lesion
- Central perforation (horizontal tear of the articular disc)
- Vascularity and management
- Avascular — debridement to a stable rim only
- Lesion
- Ulnar (foveal) avulsion of the peripheral attachment
- Vascularity and management
- Vascular — repairable (outside-in or inside-out arthroscopic)
- Lesion
- Distal avulsion from the carpal attachments (ulnocarpal ligaments)
- Vascularity and management
- Ulnar-sided pain and instability; repairable if tissue allows
- Lesion
- Radial avulsion from the sigmoid notch
- Vascularity and management
- DRUJ instability risk; may require open repair
- Lesion
- Earliest degenerative wear without perforation
- Vascularity and management
- Ulnar positive variance and ulnar impaction; treat the impaction
- Lesion
- Full perforation plus lunate or ulnar head chondromalacia plus LT disruption
- Vascularity and management
- Advanced ulnar impaction; debridement with or without ulnar shortening osteotomy
- Arthroscopic finding (midcarpal view)
- Attenuation or haemorrhage of the SL ligament; no step-off
- Typical management
- Conservative — splinting
- Arthroscopic finding (midcarpal view)
- Step-off between scaphoid and lunate; probe tip enters the gap but does not pass through
- Typical management
- Consider splinting or arthroscopic K-wire stabilisation
- Arthroscopic finding (midcarpal view)
- 1 mm probe passes freely across the SL joint
- Typical management
- Surgical stabilisation — K-wires or open SL repair
- Arthroscopic finding (midcarpal view)
- 2.7 mm arthroscope passes across the SL interval (gross instability)
- Typical management
- Open SL repair (Brunelli or three-ligament tenodesis) or K-wire stabilisation
Key evidence. Palmer (1989) established the TFCC classification into traumatic (Class 1) and degenerative (Class 2) that still guides management worldwide. Geissler and colleagues (1996) described the arthroscopic grading system for SL and LT injuries from the midcarpal side — the standard for SL instability. Osterman (1990) provided the first systematic outcomes data for arthroscopic TFCC debridement, establishing the technique as standard for Class 1A central perforations. Roth, Poehling and Whipple (1988) gave the comprehensive early description of wrist arthroscopy including portal anatomy and the systematic inspection sequence. Verhellen and Bain (2000) reported arthroscopic versus open ganglion excision — 27 percent arthroscopic recurrence versus 7 percent open — the basis for pre-operative counselling about recurrence.
References
Triangular fibrocartilage complex lesions: a classification
Landmark classification of TFCC lesions into traumatic (Class 1) and degenerative (Class 2) — the classification system used worldwide and tested in all major exams.
Intracarpal soft-tissue lesions associated with an intra-articular fracture of the distal radius
The Geissler arthroscopic grading system for scapholunate and lunotriquetral ligament injuries — the standard grading system for SL instability.
Arthroscopic debridement of triangular fibrocartilage complex tears
First systematic outcomes data for arthroscopic TFCC debridement — established the technique as the standard of care for Class 1A central perforations.
Arthroscopic surgery of the wrist
Comprehensive early description of wrist arthroscopy technique including portal anatomy and the systematic inspection sequence.
Arthroscopic ganglion excision of the wrist: a different approach
Arthroscopic versus open ganglion excision outcomes — 27 percent arthroscopic recurrence versus 7 percent open — the basis for pre-operative counselling about recurrence rates.