Benign Vascular Tumor | Vertebrae & Skull | Corduroy Sign
- Most common benign vascular tumor of bone - vertebral bodies (28%) and skull (20%)
- Pathognomonic MRI: Bright T1 AND bright T2 signal (fat content)
- Radiographs: Corduroy pattern (spine), sunburst/polka-dot (skull)
- 95%+ asymptomatic - observation only, no malignant transformation
- “Bright T1 AND T2 on MRI is pathognomonic - fat within lesion
- “Only symptomatic hemangiomas require treatment
- “Preoperative embolization reduces surgical bleeding
- “Malignant transformation does NOT occur
Hemangioma of Bone
Bright T1 AND T2: Fat content causes this unique signal pattern.
Vertical striations: Thickened trabeculae on lateral spine radiograph.
Benign forever: Unlike other tumors, hemangiomas do NOT transform.
Epidemiology
Demographics
- Most common benign vascular tumor of bone
- Autopsy studies: 10-12% of all spines have hemangiomas
- Clinical significance: Less than 1% become symptomatic
- True prevalence unknown (many never detected)
- Peak Detection: 40-60 years (mean 50 years)
- Can occur at any age after skeletal maturity
- Rare in children (less than 5% of cases)
- Likely congenital but clinically apparent in adulthood
- Female to male ratio: 2:1 overall
- Vertebral hemangiomas: Female to male 3:1
- Skull hemangiomas: No significant gender predilection
- Vertebral Bodies: 28-30% (thoracic greater than lumbar greater than cervical)
- Skull/Calvarium: 20% (frontal and parietal bones)
- Facial Bones: 10% (maxilla, mandible, zygoma)
- Long Bones: 5% (femur, humerus, tibia)
- Other: Ribs, pelvis, scapula (rare)
- Thoracic spine: 55-60% (T4-T9 most common)
- Lumbar spine: 30-35% (L1-L3)
- Cervical spine: 5-10%
- Sacrum: Less than 5%
- Multiple levels: 30-40% of vertebral cases
VERTEBRAHemangioma Characteristics
Hook:VERTEBRA for location and features
Pathophysiology
Pathogenesis
- Hamartomatous: Likely developmental malformation, not true neoplasm
- Congenital: Present from birth, grows slowly over decades
- Estrogen Influence: Female predominance suggests hormonal role
- Pregnancy Association: May enlarge during pregnancy (estrogen effect)
- Capillary Type: Small thin-walled vessels, less aggressive
- Cavernous Type: Large blood-filled spaces, more common, more symptomatic
- Mixed Type: Combination of capillary and cavernous elements
- Expansion: Slow growth causes vertebral body expansion and pain
- Fracture: Pathological fracture from vertebral body weakening
- Compression: Epidural extension causing spinal cord or nerve root compression
- Hemorrhage: Acute bleeding into lesion (very rare)
- Pregnancy: Rapid enlargement during pregnancy
- typical
- Asymptomatic (95%)
- aggressive
- Pain, neurological deficit (5%)
- typical
- Corduroy, well-defined
- aggressive
- Cortical destruction, soft tissue
- typical
- Bright T1 and T2
- aggressive
- Variable signal, soft tissue mass
- typical
- Body only, no posterior elements
- aggressive
- Body + pedicles/posterior elements
- typical
- Minimal, contained
- aggressive
- Marked expansion, epidural extension
- typical
- Observation
- aggressive
- Surgery, radiation, embolization
Clinical Presentation
Asymptomatic Hemangioma (95%)
- Incidental finding on spine imaging (MRI, CT) for unrelated complaints
- No local symptoms or neurological findings
- No intervention required
- Natural history: Stable throughout life
- Confined to vertebral body
- No posterior element involvement
- No soft tissue component
- Bright T1 and T2 signal on MRI
Symptomatic Hemangioma (Less than 1%)
- Localized Back Pain: Mechanical, worse with activity
- Nocturnal Pain: May be present with active expansion
- Radicular Pain: Nerve root compression from epidural extension
- Acute Pain: Pathological fracture (sudden onset)
- Radiculopathy: Dermatomal pain, sensory changes, weakness
- Myelopathy: Spastic gait, hyperreflexia, bowel/bladder dysfunction
- Cauda Equina Syndrome: Rare, lumbar lesions with massive epidural extension
- Acute Paraplegia: Extremely rare, acute hemorrhage or fracture
- Rapid enlargement during pregnancy (estrogen-driven)
- New-onset back pain or neurological symptoms
- Usually regresses postpartum
- May require urgent intervention if cord compression
- Asymptomatic: Palpable skull mass, cosmetic concern
- Dural Involvement: Headache, seizures (rare)
- Erosion: Through inner or outer table
- Bleeding: Profuse hemorrhage if traumatized or during surgery
- Localized pain and swelling
- Pathological fracture (rare)
- Palpable mass in superficial bones
Physical Examination
- Visible deformity (skull lesions)
- Kyphotic deformity (vertebral fracture)
- Normal overlying skin
- Tender to percussion (vertebral)
- Palpable bony prominence (skull)
- Soft tissue mass (aggressive lesions)
- Usually normal (asymptomatic cases)
- Radicular findings (dermatomal sensory loss, weakness)
- Upper motor neuron signs (myelopathy)
- Bowel/bladder dysfunction (cauda equina)
- Vast majority (95-99%) are asymptomatic incidental findings requiring NO treatment
- Symptomatic hemangiomas usually have posterior element involvement or epidural extension
- Bright T1 AND T2 signal on MRI is pathognomonic (no other lesion has this)
- Pregnancy can cause rapid enlargement - counsel female patients of childbearing age
- Profuse bleeding risk during surgery - always consider preoperative embolization
Investigations
Plain Radiography
- Lateral View: "Corduroy" or "jail-bar" appearance (vertical striations)
- Thickened vertical trabeculae
- Loss of horizontal trabeculae
- Coarse trabecular pattern
- AP View: Vertical striations less apparent
- Vertebral Body: Expansion, increased height (rare)
- Cortex: Usually intact (aggressive lesions may destroy cortex)
- Sunburst: Radiating trabeculae from center (classic)
- Honeycomb: Multiple small lucencies
- Soap-bubble: Expansile lytic lesion with septa
- Well-defined: Sclerotic margins typically
- Lytic lesion with trabeculated appearance
- "Soap-bubble" or "honeycomb" pattern
- Cortical thinning or expansion
Computed Tomography (CT)
- Axial View: "Polka-dot" or "corduroy" sign
- Thickened vertical trabeculae seen as dots
- Low-attenuation marrow between trabeculae
- Sagittal/Coronal: Vertical striations evident
- Cortical Integrity: Assess for destruction
- Epidural Extension: Soft tissue component into spinal canal
- Radiating trabeculations
- Diploe expansion (between inner and outer tables)
- Soft tissue mass if dural involvement
Magnetic Resonance Imaging (MRI)
- T1-Weighted: BRIGHT signal (hyperintense)
- Due to fat content between vascular spaces
- Same intensity as subcutaneous fat
- T2-Weighted: BRIGHT signal (hyperintense)
- Due to slow-flowing blood and edema
- Heterogeneous hyperintensity
- STIR/Fat-Suppression: Signal drops out (confirms fat)
- Extension into posterior elements (pedicles, lamina)
- Epidural soft tissue mass
- Spinal cord compression or displacement
- Vertebral body expansion (greater than 50% canal compromise)
- Heterogeneous signal (less fat, more vascular)
- Usually not needed for diagnosis
- Enhances if performed (vascular lesion)
- Helps delineate epidural extent for surgical planning
MRI Diagnostic Criteria: The combination of BRIGHT T1 and BRIGHT T2 signal is virtually pathognomonic for hemangioma. No other bone lesion shows this pattern:
- Metastases: Dark T1, bright T2
- Myeloma: Dark T1, bright T2
- Hemangioma: BRIGHT T1, BRIGHT T2 (unique)
If you see bright T1 and bright T2 in vertebral body = hemangioma until proven otherwise. Biopsy usually NOT needed.
Angiography
- Preoperative planning for surgery
- Embolization procedure (symptomatic lesions)
- Confirm vascular nature if imaging ambiguous
- Hypervascular lesion with intense blush
- Arterial feeders (vertebral, intercostal, or lumbar arteries)
- Arteriovenous shunting in some cases
- Reduce vascularity before surgery (decrease bleeding)
- Perform 24-48 hours before operation
- Agents: Polyvinyl alcohol (PVA), coils, Onyx
Histopathology
- Atypical radiographic features (cortical destruction, soft tissue)
- Concern for malignancy (angiosarcoma)
- Neurological deficit with unclear diagnosis
- Young patient (hemangiomas rare in children)
- Red-purple spongy tissue
- Blood-filled spaces
- Soft consistency
- Cavernous Type: Large thin-walled vascular channels
- Endothelial-lined spaces
- Separated by fibrous stroma
- Fatty marrow between vessels
- Capillary Type: Small capillary-sized vessels
- Densely packed
- Less fatty stroma
- No Cellular Atypia: Bland endothelial cells
- No Mitoses: Benign proliferation
- CD31: Positive (endothelial marker)
- CD34: Positive (vascular marker)
- ERG: Positive (endothelial transcription factor)
- Ki-67: Low proliferation index (less than 2%)
- Cytokeratin: Negative (excludes carcinoma)
- Angiosarcoma: Cellular atypia, mitoses, infiltrative growth
- Hemangioblastoma: CNS lesion, not bone primary
- Vascular Malformation: Similar but developmental anomaly, not tumor
BRIGHTHemangioma MRI Features
Hook:BRIGHT for MRI diagnosis
Differential Diagnosis
- Age: Usually older (greater than 50 years)
- History: Known primary malignancy
- MRI: Dark T1, bright T2 (opposite of hemangioma)
- Distribution: Multiple lesions common
- Pedicle: Often destroyed (hemangioma spares pedicle usually)
- Age: Greater than 60 years typically
- Labs: Monoclonal protein, hypercalcemia, anemia
- MRI: Dark T1, bright T2, diffuse marrow infiltration
- Radiology: "Punched-out" lytic lesions, osteopenia
- Age: Elderly (greater than 60 years)
- Labs: Elevated alkaline phosphatase
- Radiology: Mixed lytic and sclerotic, "picture frame" vertebra
- Distribution: Polyostotic, pelvis common
- Location: Sacrum most common, can be mobile spine
- MRI: Destructive, soft tissue mass, bright T2
- Age: Adults 40-60 years
- Pathology: Physaliferous cells, brachyury positive
- Age: 20-40 years
- Location: Sacrum greater than mobile spine
- MRI: Dark T1, heterogeneous T2
- Radiology: Lytic, destructive, extends into soft tissue
- Age: Children less than 10 years
- Radiology: "Punched-out" lytic lesion, beveled edges
- Pathology: CD1a+ Langerhans cells
- Behavior: May spontaneously resolve
- Age: Adolescents/young adults
- Radiology: Destructive, soft tissue mass, periosteal reaction
- Pathology: Malignant osteoid production, cellular atypia
- Prognosis: Poor if malignant
- Location: Skull vault, hyperostotic
- Radiology: Sclerotic, "sunburst" can mimic hemangioma
- MRI: Homogeneous enhancement
- Age: Adults 40-60 years
- hemangioma
- BRIGHT (pathognomonic)
- metastasis
- DARK
- myeloma
- DARK
- paget
- Variable (mixed)
- hemangioma
- BRIGHT
- metastasis
- BRIGHT
- myeloma
- BRIGHT
- paget
- Variable
- hemangioma
- Corduroy (vertical striations)
- metastasis
- Lytic destruction
- myeloma
- Punched-out, osteopenia
- paget
- Picture frame, sclerotic
- hemangioma
- Rare (aggressive types only)
- metastasis
- Common (destroyed)
- myeloma
- Occasional
- paget
- Yes (sclerotic)
- hemangioma
- Usually solitary (70%)
- metastasis
- Multiple
- myeloma
- Diffuse
- paget
- Polyostotic
- hemangioma
- 40-60 years
- metastasis
- 50-70 years
- myeloma
- Greater than 60 years
- paget
- Greater than 60 years
Surgical Management of Cord-Compressing Vertebral Hemangiomas (Mayo Clinic)
- Of 59 vertebral hemangiomas, 11 presented with or developed spinal cord compression
- All 11 cord-compression patients recovered fully after decompressive surgery
- Subtotal resection followed by low-dose radiotherapy (1000 cGy or less) led to recurrence in 3 of 6; no recurrence with 2600-4500 cGy or gross total removal
- Authors recommend preoperative angiography and embolization for progressive deficit, then decompression with the approach dictated by extent, and postoperative radiotherapy after subtotal removal
Embolization Safety: Protecting the Spinal Cord Blood Supply
The topic calls preoperative embolization "essential" and lists it in almost every management pathway, and its own Controversies note that "radicular feeders raise spinal-cord-infarction concerns" - but the procedural safety that underlies this is never developed, and it is the single most important thing to know before embolizing a thoracolumbar vertebral hemangioma. (The cord's arterial anatomy itself is covered in the spinal-cord-blood-supply topic; this is the embolization-procedure nuance.)
- The danger is a shared radiculomedullary feeder. The segmental (intercostal/lumbar) arteries that supply a vertebral hemangioma can also give off a radiculomedullary branch to the anterior spinal artery - in the lower thoracic/upper lumbar spine this is the artery of Adamkiewicz (arteria radicularis magna, usually left, T9-L2). Embolic material that passes into that branch causes anterior spinal artery infarction and paraplegia - the catastrophic complication of spinal tumour embolization.
- How the risk is minimised. Embolization is done by superselective microcatheterisation of the tumour's feeding pedicles, with careful pre-embolization angiography (and provocative testing where indicated) to confirm that the vessel about to be embolized does not supply the cord; the particle size is chosen large enough not to pass through arteriovenous shunts into the cord or lungs; and the operator stops if a radiculomedullary/cord feeder is identified. Liquid agents and ethanol (alcohol) are powerful but higher-risk (reflux, cord infarction, skin necrosis, cardiovascular effects), so they are used cautiously.
- Timing and purpose. Particulate transarterial embolization is performed 24-48 hours before surgery (not the same day) so the tumour bed thromboses and intraoperative blood loss falls; it is also used as a stand-alone or vertebroplasty-adjunct treatment for painful non-compressive lesions.
Q: What is the key safety concern when embolizing a vertebral hemangioma? A: The segmental feeders can share a radiculomedullary branch to the anterior spinal artery (the artery of Adamkiewicz, typically left T9-L2) - embolizing it causes anterior spinal artery infarction and paraplegia. Mitigate by superselective catheterisation, pre-embolization angiography ± provocative testing to exclude a cord feeder, appropriate particle size, and abandoning embolization of any vessel supplying the cord. Embolize 24-48 hours pre-op so the tumour thromboses.
Vertebroplasty in a Hypervascular Lesion: the Cement-Leak Hazard
The topic recommends vertebroplasty/kyphoplasty across its pain pathways and lists "cement extravasation" as a complication, but never explains why a hemangioma is uniquely dangerous to cement - a high-yield point that also explains why alcohol/embolization is often done first.
- The lesion is plumbed into the epidural veins. A hemangioma's dilated intraosseous vascular channels communicate directly with the basivertebral vein and the valveless epidural and paravertebral venous plexus (Batson's plexus). Injecting PMMA cement into this high-flow vascular space therefore risks the cement tracking into the epidural space (cord/root compression) or embolizing through the veins to the lungs (pulmonary cement embolism) - a greater risk than in an ordinary osteoporotic fracture.
- Reduce the flow before you inject. This is the rationale for pre-procedural sclerosis/embolization (transarterial particles or intralesional alcohol) before cement in an aggressive or epidural-extending hemangioma - occluding the vascular channels first lowers the leak risk and improves the durability shown in the alcohol-embolization-plus-vertebroplasty series.
- Inject safely. Use higher-viscosity cement injected slowly under continuous ("live") biplane/lateral fluoroscopy, and stop at the first sign of posterior or venous filling; a kyphoplasty balloon cavity can allow a more controlled, lower-pressure fill. The goal is pain relief and stabilisation, not complete filling.
Q: Why is cement extravasation especially dangerous in a vertebral hemangioma, and how do you mitigate it? A: The hemangioma's dilated channels connect to the basivertebral and valveless epidural/paravertebral (Batson) venous plexus, so injected PMMA can track into the epidural space (cord compression) or embolize to the lungs. Mitigate by sclerosing/embolizing the lesion first (alcohol or particles), then injecting high-viscosity cement slowly under continuous live fluoroscopy, stopping at the first hint of venous/posterior filling.
Management
Asymptomatic Hemangiomas
- Indications: Incidental finding, no symptoms, no aggressive features
- Protocol: NO follow-up imaging required
- Counseling: Explain benign nature, no risk of malignant transformation
- Activity: No restrictions
- Prognosis: Stable lifelong, intervention rarely needed
- Benign vascular tumor, not cancer
- Will not cause symptoms in vast majority
- Return if new back pain or neurological symptoms develop
- Safe to ignore for asymptomatic cases
Symptomatic Hemangiomas
- Indications: Symptomatic pain without neurological deficit
- Dose: 20-40 Gy fractionated (10-20 fractions)
- Mechanism: Sclerosis of vascular channels, reduces tumor volume
- Success Rate: 80-90% pain relief
- Onset: Gradual over weeks to months
- Side Effects: Radiation myelopathy (rare), skin changes, vertebral compression fracture
- Contraindications: Neurological deficit (surgery preferred), young age
- Indications: Painful vertebral hemangioma with partial collapse
- Technique: Percutaneous cement injection into vertebral body
- Outcomes: Immediate pain relief in 80-90%
- Complications: Cement extravasation (epidural, vascular), rarely neurological injury
- Advantage: Minimally invasive, quick recovery
- Indications: Reduce tumor vascularity, pain palliation
- Technique: Transarterial embolization of feeding vessels
- Agents: PVA particles, coils, Onyx liquid embolic
- Outcomes: Variable pain relief (50-70%)
- Limitations: Recurrence common (reconstitution of blood supply)
- Best Use: Preoperative adjunct before surgery
- Indications:
- Neurological deficit (myelopathy, radiculopathy)
- Spinal instability or pathological fracture
- Epidural extension with cord compression
- Failed radiation or vertebroplasty
- Rapidly progressive symptoms
- Embolization: Perform 24-48 hours before surgery (reduce bleeding)
- Essential for vascular lesions
- Decreases intraoperative blood loss by 40-60%
- Blood Products: Type and cross 4-6 units PRBC (potential massive bleeding)
- Cell Saver: Available for autotransfusion
- Imaging: Updated MRI for surgical approach planning
- Laminectomy to decompress spinal cord
- Remove epidural component of hemangioma
- Instrumented fusion if instability (usually required)
- Avoid aggressive curettage of vertebral body (bleeding risk)
- Indications: Extensive vertebral body involvement, instability, failed decompression
- Technique:
- Anterior or posterior approach (or combined)
- En bloc or piecemeal vertebrectomy
- Cage reconstruction (titanium mesh, PEEK, allograft strut)
- Posterior instrumented fusion
- Outcomes: Definitive treatment, low recurrence
- Morbidity: Significant, requires anterior approach often
- Long bone hemangiomas
- Thorough curettage, local adjuvants (phenol, cryotherapy)
- Bone grafting (autograft or allograft)
- Prophylactic fixation if structural defect
- Massive Hemorrhage: Most significant risk (up to 2-3 liters blood loss)
- Neurological Injury: Cord or nerve root damage
- Incomplete Resection: Residual tumor if bleeding prevents visualization
- Infection: Standard surgical site infection risk
- Instability: May require fusion if destabilizing procedure
Comprehensive Management of Symptomatic and Aggressive Vertebral Hemangiomas
- Conservative surgical strategies (decompression without aggressive resection) suit most symptomatic hemangiomas causing cord compression without instability or deformity
- Complete intralesional spondylectomy after embolization can be performed safely for aggressive lesions with circumferential vertebral involvement and prevents recurrence
- Transarterial embolization without decompression is effective for painful intraosseous (non-compressive) hemangiomas
- Vertebroplasty improves pain, especially with vertebral body compression fracture and no deficit, but is less durable for long-term pain control
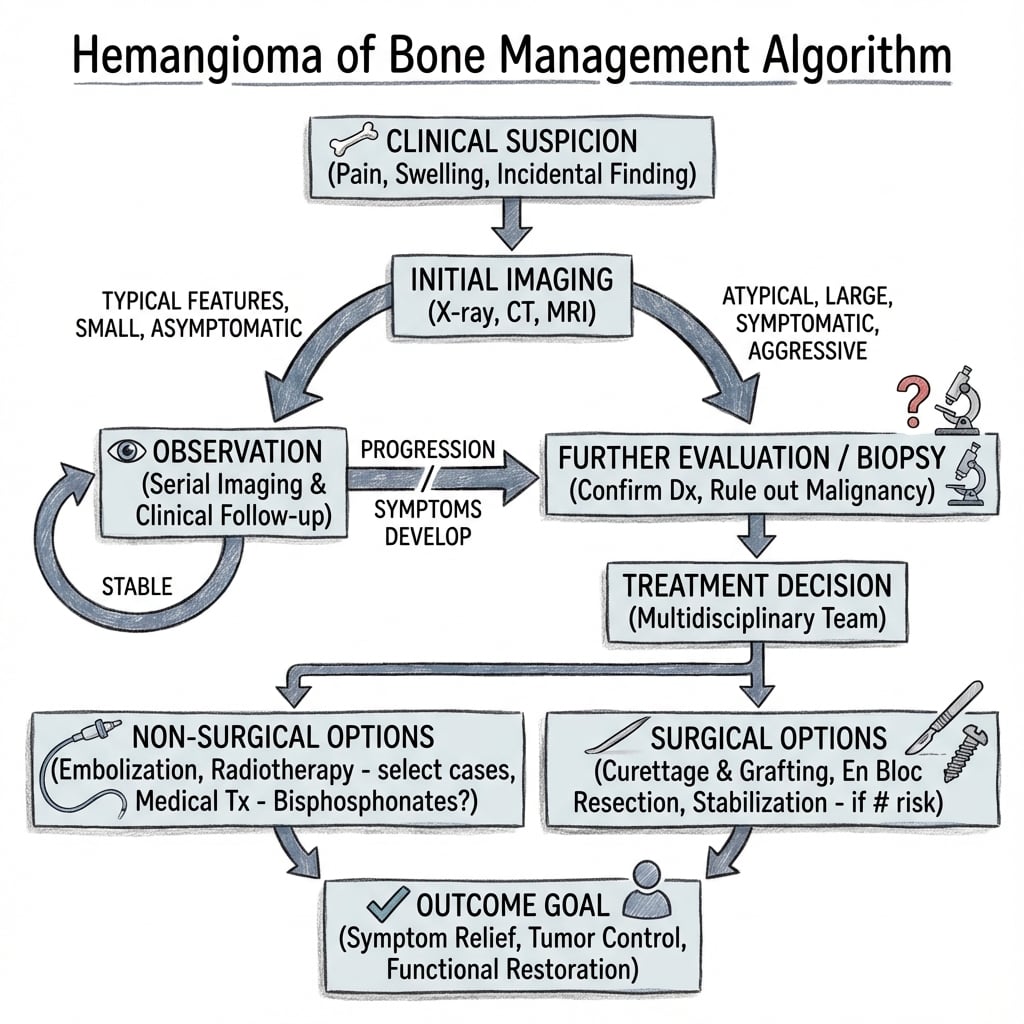
Treatment Algorithm
-
Asymptomatic, Incidental:
- Observation, no follow-up imaging
- Patient education, discharge
-
Symptomatic Pain, NO Neurological Deficit:
- First-line: Radiotherapy (20-40 Gy)
- Alternative: Vertebroplasty/kyphoplasty
- Embolization if above contraindicated
-
Neurological Deficit or Cord Compression:
- Urgent MRI to confirm compression
- Preoperative embolization (24-48 hours prior)
- Surgical decompression + fusion
- Consider adjuvant radiotherapy postoperatively
-
Pathological Fracture:
- Kyphoplasty if stable fracture, no neurology
- Surgical stabilization if unstable or neurological deficit
-
Aggressive Features (Cortical Destruction, Soft Tissue):
- Biopsy to exclude angiosarcoma
- En bloc resection if feasible
- Radiotherapy + embolization if unresectable
- Observation is STANDARD for asymptomatic hemangiomas (95%+)
- Radiotherapy effective for painful hemangiomas WITHOUT neurological deficit
- Surgery reserved for neurological compromise or failed conservative measures
- ALWAYS preoperative embolization before surgery (reduces massive bleeding)
- Vertebroplasty excellent option for painful hemangioma with vertebral collapse
Management Algorithm
Complications & Prognosis
Complications
- Pathological Fracture: Less than 5% (vertebral compression)
- Spinal Cord Compression: Less than 1% (epidural extension)
- Acute Hemorrhage: Extremely rare (acute neurological deficit)
- Pregnancy-Related Enlargement: Rare, usually regresses postpartum
- Radiation myelopathy (less than 1% with modern techniques)
- Vertebral compression fracture (5-10%)
- Skin changes (erythema, pigmentation)
- Lhermitte sign (transient)
- Cement extravasation: Epidural (2-5%), vascular (1-2%)
- Neurological injury: Less than 1%
- Infection: Less than 1%
- Adjacent level fracture: 5-10%
- Massive intraoperative hemorrhage (10-20% even with embolization)
- Neurological worsening (2-5%)
- CSF leak (3-5%)
- Infection (2-5%)
- Recurrence (5% if incomplete resection)
Prognosis
- Excellent: Stable lifelong, no intervention needed
- Risk of becoming symptomatic: Less than 1% over lifetime
- No malignant transformation (benign entity)
- Radiotherapy: 80-90% pain relief, gradual over months
- Vertebroplasty: 80-90% immediate pain relief
- Surgery: 85-95% neurological improvement if preoperative deficit
- Recurrence: 5% after surgical excision
- Most patients remain asymptomatic lifelong
- Symptomatic cases respond well to treatment
- Quality of life: Excellent after successful treatment
- Return to activities: Full return in majority
BENIGNHemangioma Prognosis Features
Hook:BENIGN for prognosis
Guidelines, Registries & Global Practice
Global Epidemiology
- Most common benign vascular tumour of bone; found in 10-12% of spines at autopsy worldwide
- Vertebral body (28-30%) and calvarium (about 20%) are the dominant sites; thoracic spine predominates
- Peak detection 4th-5th decades, female-to-male ratio about 2:1 (up to 3:1 for vertebral lesions)
- Under 1% of all hemangiomas ever become symptomatic, and progression of an incidental lesion is rare (2 of 59 over a mean 7.4 years in the Mayo series)
Side-by-Side Guidance
Bone hemangioma has no single dedicated society guideline; recommendations are derived from tumour-classification bodies and spine-oncology consensus. Where they converge and where emphasis differs:
- who
- Benign vascular neoplasm; imaging usually diagnostic
- acr_esr
- Bright T1 and T2 with fat = no biopsy; MRI/CT problem-solving
- spine_onc
- Reserve biopsy for atypical/aggressive features
- who
- No malignant potential
- acr_esr
- No routine surveillance imaging
- spine_onc
- Observation; reassure
- who
- n/a (classification body)
- acr_esr
- Vertebroplasty or radiotherapy (at least 34 Gy)
- spine_onc
- Radiotherapy or vertebroplasty; embolization adjunct
- who
- n/a
- acr_esr
- Angiography/embolization then intervention
- spine_onc
- Preoperative embolization + decompression +/- spondylectomy
WHO Classification of Tumours (5th ed, 2020) anchors the benign biology. Imaging-society guidance (ACR Appropriateness Criteria, ESR/European radiology consensus) drives the no-biopsy, no-surveillance approach for classic lesions. Spine-oncology consensus (e.g. AO Spine, Acosta/UCSF framework) governs the graded intervention ladder.
Registry and Resource Considerations
- No arthroplasty-style registry tracks hemangioma; evidence rests on institutional series (Mayo, UCSF, Pitie-Salpetriere) and the German multicenter radiotherapy cohort
- High-resource settings: Interventional radiology enables preoperative or stand-alone transarterial/alcohol embolization and vertebroplasty, shifting many aggressive epidural cases away from open surgery
- Limited-resource settings: Where embolization and cell-salvage are unavailable, open surgery for vascular lesions carries higher haemorrhage risk; radiotherapy (widely available, dose at least 34 Gy) becomes a key first-line option for painful lesions, and conservative observation is emphasised for incidental findings
- MDT coordination between spine surgeon and interventional radiologist is the practice standard wherever embolization is offered
Controversies & Areas of Uncertainty
- Surveillance of "atypical" but asymptomatic lesions: Low-T1 (fat-poor) lesions can look worrying yet behave indolently. There is no consensus on whether to image-monitor a fat-poor lesion without Laredo aggressive features; most authors observe, but interval MRI is sometimes used.
- Vertebroplasty alone for aggressive epidural lesions: Cementoplasty (with or without alcohol embolization) controls pain and sensory symptoms durably, but is unreliable for motor deficit. The threshold for choosing percutaneous treatment over open decompression in patients with mild myelopathy is debated.
- Embolization technique and timing: Particulate transarterial embolization 24-48 hours preoperatively is standard, but direct intralesional alcohol/Onyx and the optimal interval are not standardised, and radicular feeders raise spinal-cord-infarction concerns.
- Adjuvant radiotherapy after subtotal resection: Historical data show recurrence with under-dosed radiotherapy; the role of routine postoperative radiotherapy after modern gross-total or near-total resection is unsettled, and long-term radiation risk must be weighed in young patients.
- Pregnancy-associated enlargement: The reported rapid growth and regression of vertebral hemangiomas in pregnancy is based on case reports; the true magnitude of estrogen sensitivity and how aggressively to intervene during pregnancy remain uncertain.
- Biopsy safety: Bright-T1/T2 classic lesions need no biopsy, but when imaging is atypical the bleeding risk of percutaneous biopsy of a vascular lesion versus the need to exclude angiosarcoma is a genuine trade-off.
MCQ Practice Points
Q: What is the classic radiographic appearance of vertebral hemangioma on plain films and CT?
A: Corduroy/jail-bar sign on lateral radiograph: Vertical striations from thickened trabeculae. Polka-dot sign on axial CT: Thickened trabeculae in cross-section appearing as dots. Fat and blood within lesion. Most are incidental findings in thoracic greater than lumbar spine. Typically involves vertebral body.
Q: What MRI characteristics distinguish aggressive from non-aggressive vertebral hemangiomas?
A: Non-aggressive: T1 and T2 hyperintense (high fat content), partial vertebral body involvement, no expansion. Aggressive: T1 hypointense (less fat, more vascular), entire vertebral body involved, posterior element extension, epidural soft tissue mass, cortical expansion. Low T1 signal correlates with aggressive behavior.
Q: Why should bone scan not be used to screen for multiple myeloma but can detect vertebral hemangiomas?
A: Myeloma suppresses osteoblast activity - purely lytic lesions show no bone scan uptake. Hemangiomas have reactive bone formation around dilated vessels - show variable uptake. However, vertebral hemangiomas are usually diagnosed on MRI during spinal imaging. Myeloma screening uses skeletal survey or whole-body MRI.
Q: What are the treatment options for symptomatic or aggressive vertebral hemangioma?
A: Asymptomatic: Observation only. Painful without compression: Vertebroplasty (cement stabilization and pain relief). Cord compression: Embolization + surgical decompression + stabilization. Pre-operative embolization reduces intraoperative bleeding. Radiation for residual/recurrent disease. Avoid biopsy - risk of hemorrhage.
Q: What is the typical location and age distribution of bone hemangiomas?
A: Most common in spine (thoracic greater than lumbar), followed by skull. Long bone and appendicular involvement rare. Peak incidence 4th-5th decades. Female predominance. Incidence increases with age - found in 10-12% of autopsy spines. Most remain asymptomatic throughout life; only 1% become symptomatic.
At a Glance
Hemangioma of bone is a benign vascular tumor most common in vertebral bodies (28%) and skull (20%), typically incidental in adults 40-60 years with 2:1 female predominance. Pathognomonic MRI shows bright T1 AND bright T2 signal (fat content). Radiographs show corduroy pattern in spine, sunburst in skull. 95%+ are asymptomatic requiring observation only. Symptomatic lesions may require radiotherapy, vertebroplasty, or surgery with preoperative embolization. Malignant transformation does NOT occur.
CORDUROYHemangioma Features - CORDUROY
Hook:The classic radiographic sign is your memory hook
SEVEREHemangioma Treatment - SEVERE
Hook:Only SEVERE cases need intervention
FATMRI Features - FAT
Hook:Fat content explains the MRI
Exam Essentials:
- Benign vascular tumor, most common in vertebral bodies (28%) and skull (20%)
- Usually incidental finding in adults (40-60 years), female predominance 2:1
- Radiology: "Corduroy" (vertical striations) in spine, "sunburst" or "polka-dot" in skull
- MRI: Bright on T1 and T2 (fat content), definitive diagnostic feature
- 95% asymptomatic, symptomatic if aggressive (rapid growth, cortical destruction)
- Management: Observation for asymptomatic, surgery/embolization/radiation for symptomatic
- Pathological fracture in less than 5%, neurological compression rare
- Malignant transformation does NOT occur (benign entity)
Visual One-Pager
- 50-year-old woman with incidental vertebral lesion on lumbar spine MRI
- Asymptomatic, discovered during evaluation for mechanical back pain
- MRI shows bright T1 and T2 signal in L3 vertebral body
- "Corduroy" appearance on lateral radiograph
- Plain X-ray: Vertical striations (corduroy) in vertebrae, sunburst (skull)
- MRI: High T1 and T2 signal (pathognomonic), no enhancement pattern needed
- CT: Thickened vertical or radiating trabeculae, "polka-dot" axial view
- Biopsy: Only if atypical features (soft tissue mass, cortical destruction)
- Asymptomatic (95%): Observation, no follow-up imaging needed
- Symptomatic Pain: Radiotherapy (20-40 Gy), vertebroplasty/kyphoplasty
- Neurological Deficit: Decompression + stabilization, preoperative embolization
- Pathological Fracture: Surgical fixation + curettage, bone grafting
- Aggressive Features: Biopsy to exclude angiosarcoma, consider en bloc resection
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old woman undergoes MRI for chronic mechanical low back pain. L3 vertebral body shows a 2 cm lesion with bright signal on both T1 and T2 sequences, no epidural extension, no posterior element involvement. She has no radicular symptoms or neurological deficit.”
“A 48-year-old man presents with 3-month progressive bilateral lower extremity weakness, gait imbalance, and hyperreflexia. MRI shows T6 vertebral hemangioma with epidural extension causing 60% spinal canal stenosis and cord compression. No pathological fracture. He has 4/5 strength in lower extremities and upgoing plantars.”
“A 38-year-old woman has 6 months of severe localised thoracic pain. MRI shows a T8 hemangioma with low T1 signal, involvement of the whole vertebral body and pedicle, and a small epidural soft-tissue component causing mild canal narrowing. She has sensory paraesthesia in a band-like distribution but normal power, reflexes, and bladder function. She is keen to avoid major open surgery.”
Must-Know Facts
- DEFINITION: Benign vascular tumor, most common in vertebrae (28%) and skull (20%)
- AGE: Adults 40-60 years, female to male 2:1, rare in children
- INCIDENCE: 10-12% of spines at autopsy, less than 1% symptomatic
- PATHOGNOMONIC MRI: BRIGHT T1 and BRIGHT T2 (fat + blood, no other lesion does this)
- X-RAY: Corduroy (vertical striations) in spine, sunburst/honeycomb in skull
- MANAGEMENT: Observation for 95%+ (asymptomatic), surgery only if neurological deficit
- PROGNOSIS: Benign, never malignant transformation, excellent outcomes
Imaging Key Points
- MRI T1 BRIGHT + T2 BRIGHT = hemangioma (pathognomonic, no biopsy needed)
- PLAIN X-RAY SPINE: Corduroy (vertical striations lateral view), polka-dot (CT axial)
- PLAIN X-RAY SKULL: Sunburst (radiating trabeculae), honeycomb, soap-bubble
- AGGRESSIVE FEATURES: Posterior element involvement, epidural extension, soft tissue mass, cortical destruction
- CT: Thickened vertical trabeculae (polka-dot axial), assess cortical integrity
- ANGIOGRAPHY: Preoperative embolization (24-48h before surgery), reduce bleeding 40-60%
Management Algorithm
- ASYMPTOMATIC (95%): Observation ONLY, NO follow-up imaging, reassure benign
- SYMPTOMATIC PAIN, NO NEUROLOGY: Radiotherapy (20-40 Gy) first-line OR vertebroplasty/kyphoplasty
- NEUROLOGICAL DEFICIT: URGENT surgery - preop embolization (essential), decompression + fusion
- PATHOLOGICAL FRACTURE: Kyphoplasty if stable, surgery if unstable or neurological compromise
- AGGRESSIVE/ATYPICAL: Biopsy (exclude angiosarcoma), consider en bloc resection
- PREGNANCY-RELATED: May enlarge during pregnancy, usually regresses postpartum, surgery if urgent
Surgical Principles
- PREOP EMBOLIZATION: Mandatory 24-48 hours before surgery (reduce bleeding 40-60%)
- BLOOD PRODUCTS: Type and cross 4-6 units PRBC, cell saver, massive transfusion protocol ready
- APPROACH: Posterior decompression + instrumented fusion standard for epidural component
- TECHNIQUE: Remove epidural tumor, avoid aggressive vertebral body curettage (massive bleeding)
- VERTEBRECTOMY: Consider if extensive body involvement, anterior or posterior approach, cage reconstruction
- ACCEPT SUBTOTAL: If bleeding prohibitive, subtotal resection + adjuvant radiotherapy (20-30 Gy)
- OUTCOMES: 85-95% neurological improvement, 5% recurrence (incomplete resection)
Viva Traps to Avoid
- DON'T: Biopsy classic bright T1/T2 lesion - imaging is diagnostic, biopsy unnecessary
- DON'T: Treat asymptomatic hemangiomas - observation is standard, no follow-up needed
- DON'T: Operate without preoperative embolization - massive bleeding will occur
- DON'T: Confuse with metastasis - mets are DARK T1, hemangioma is BRIGHT T1
- DON'T: Promise complete excision - accept subtotal if bleeding severe, use adjuvant XRT
- DO: Embolize 24-48 hours before surgery (not same day, need time for thrombosis)
- DO: Have 4-6 units PRBC available (high transfusion rate even with embolization)
- DO: Explain benign nature to patient - no cancer risk, no follow-up for asymptomatic
Quick Differentials
- METASTASIS: Dark T1 bright T2 (opposite), multiple lesions, pedicle destruction, known primary
- MYELOMA: Dark T1 bright T2, punched-out lytic, age greater than 60, monoclonal protein, anemia
- PAGET DISEASE: Mixed lytic/sclerotic, picture frame vertebra, elevated ALP, age greater than 60
- HEMANGIOMA: BRIGHT T1 BRIGHT T2 (unique), corduroy X-ray, asymptomatic, benign
- KEY: MRI signal differentiates - only hemangioma is bright T1
Evidence Base
Vertebral Hemangiomas: Radiologic Criteria for Aggressiveness (Laredo Criteria)
- 57 solitary vertebral hemangiomas reviewed to separate quiescent from cord-compressing lesions
- Six features predicted aggressive (compressive) behaviour: T3-T9 location, whole vertebral body involvement, neural-arch extension, expanded cortex with indistinct margins, irregular honeycomb pattern, soft-tissue mass
- Three or more of these signs in a painful patient flag a potentially symptomatic lesion warranting angiography +/- embolization
Natural History and Management of Vertebral Hemangiomas (Mayo Clinic)
- 59 cases over a decade; lesions incidental in 35, painful in 13, with neurological deficit in 11
- Progression from asymptomatic/painful to neurological symptoms in only 2 cases over mean 7.4-year follow-up - routine surveillance of asymptomatic lesions is unnecessary
- All 11 patients with cord compression had full neurological recovery after decompressive surgery
- Recurrence after subtotal resection occurred only when adjuvant radiotherapy was 1000 cGy or less; no recurrence with 2600-4500 cGy
- Recommends preoperative angiography and embolization for progressive deficit, decompression, and postoperative radiotherapy after subtotal removal
Radiotherapy for Symptomatic Vertebral Hemangiomas: Multicenter Study
- Largest series to date: 84 patients with 96 symptomatic lesions across 7 institutions; pain was the indication in 97.6%
- Overall response 90.5% (complete remission 61.9%, partial 28.6%) at median 68-month follow-up
- Total dose of 34 Gy or more gave significantly better symptom relief and control than under 34 Gy
- Radiological reossification seen in 26.2% but did not correlate with pain relief
Percutaneous Alcohol Embolization plus Vertebroplasty for Aggressive Hemangiomas with Epidural Extension
- 26 patients with 27 aggressive hemangiomas with epidural extension treated by alcohol embolization then vertebroplasty, no surgery
- Mean pain VAS fell from 7.2 to 3.1 (p less than 0.001) at mean 88-month follow-up; 38.5% became asymptomatic
- 88% of patients with sensory disturbance had complete regression; 2 of 3 with motor deficit did not improve
- No major complications - a minimally invasive alternative to open surgery for selected epidural cases
Musculoskeletal Angiomatous Lesions: Radiologic-Pathologic Correlation (AFIP)
- Hemangioma is the most common angiomatous lesion of bone, favouring spine and calvaria
- Characteristic appearance: coarsened trabeculae adjacent to vascular channels, or multifocal lytic honeycomb pattern
- MRI shows fat overgrowth and serpentine vascular channels; phleboliths may be seen in soft-tissue lesions
- More aggressive vascular tumours (hemangioendothelioma, hemangiopericytoma, angiosarcoma) have nonspecific imaging and require biopsy
WHO Classification of Soft Tissue and Bone Tumours, 5th edition
- Haemangioma of bone classified as a benign vascular neoplasm with no metastatic potential and no recognised malignant transformation
- Recently characterised by recurrent activating somatic mutations in the GNAQ/GNA11/GNA14 pathway in a subset of lesions
- Distinguished from epithelioid haemangioma (locally aggressive, intermediate) and angiosarcoma (malignant) on histology