Most Common Primary Bone Cancer
- Distal Femur: Most common location (50%), then proximal tibia (25%).
- Bimodal Age: Adolescents (primary) and over 60 (secondary - Paget's).
- Sunburst: Spiculated periosteal reaction - pathognomonic radiographic sign.
- Codman Triangle: Elevated periosteum at tumor margin.
- MAP Protocol: Methotrexate (high-dose), Adriamycin, cisPlatin.
- Histologic Response: Over 90% necrosis = good prognosis (75-80% survival).
- “Distal femur most common primary bone cancer location
- “Sunburst + Codman triangle = osteosarcoma until proven otherwise
- “Neoadjuvant chemo BEFORE surgery - treats micrometastases
- “Over 90% necrosis = good response and better prognosis
- “Biopsy tract must be excised with specimen - plan with surgeon

Osteosarcoma treatment REQUIRES CHEMOTHERAPY.
- Surgery alone results in 80% recurrence (micrometastases at presentation).
- Neoadjuvant chemotherapy: Shrinks tumor, treats micrometastases, allows histologic assessment.
- Adjuvant chemotherapy: Completes treatment, improves survival from 20% to 60-70%.
- Exception: Parosteal osteosarcoma (low-grade surface) - wide resection only.
Overview/Epidemiology
Osteosarcoma is the most common primary malignant bone tumor, characterized by direct formation of osteoid or immature bone by malignant mesenchymal cells.
Epidemiology
- 3-4 per million per year
- 400 new cases in USA annually
- Most common in adolescents
- Second peak over 60 years
- Prior radiation therapy
- Paget's disease (1% transform)
- Li-Fraumeni syndrome (p53)
- Hereditary retinoblastoma (Rb1)
- Rothmund-Thomson syndrome
- Distal femur: 50%
- Proximal tibia: 25%
- Proximal humerus: 10%
- Other long bones: 15%
- Metaphyseal predilection
Bimodal Age Distribution
- Age Range
- 10-20 years
- Characteristics
- Rapid skeletal growth
- Association
- Metaphyseal location, conventional type
- Age Range
- Over 60 years
- Characteristics
- Paget's sarcoma
- Association
- Axial skeleton, poor prognosis
Paget's Sarcoma: Secondary osteosarcoma in Paget's disease occurs in 1% of patients. Presents with sudden increase in pain, rapid enlargement, or rising alkaline phosphatase in known Paget's. Very poor prognosis (5-year survival under 10%).
Anatomy/Biomechanics
Anatomic Considerations for Tumor Location
Metaphyseal Predilection:
- Osteosarcoma arises from primitive mesenchymal bone-forming cells
- Metaphyses have highest osteoblastic activity during growth
- Rich blood supply to metaphyses facilitates tumor growth
- Growth plate initially acts as barrier to epiphyseal extension
Compartmental Anatomy
Tumor Extension Patterns:
- Barrier
- Cortical bone
- Clinical Significance
- Skip lesions possible - MRI entire bone
- Barrier
- Soft tissue planes
- Clinical Significance
- Neurovascular involvement risk
- Barrier
- Growth plate
- Clinical Significance
- Less effective barrier than previously thought
- Barrier
- Joint capsule
- Clinical Significance
- Rare but indicates Stage IIB/III
Neurovascular Relationships
- Popliteal artery/vein: Posterior to femur, at risk with posterior extension
- Femoral artery/vein: In Hunter's canal - anterior/medial approach consideration
- Sciatic nerve: Posterolateral - divides to tibial and common peroneal above knee
- Popliteal vessels: Posterior, trifurcate below knee
- Anterior tibial vessels: Pass through interosseous membrane
- Common peroneal nerve: Wraps around fibular neck - high risk
Classification Systems
WHO Histologic Classification:
- Grade
- High
- Location
- Intramedullary
- Chemotherapy
- Yes - MAP protocol
- Grade
- High
- Location
- Intramedullary
- Chemotherapy
- Yes - Same as conventional
- Grade
- High
- Location
- Intramedullary
- Chemotherapy
- Yes - May add Ewing's protocol
- Grade
- Low
- Location
- Surface (posterior femur)
- Chemotherapy
- No - Wide resection only
- Grade
- Intermediate
- Location
- Surface (diaphysis)
- Chemotherapy
- Consider adjuvant
- Grade
- High
- Location
- Surface
- Chemotherapy
- Yes - Full protocol
Key point: Conventional osteosarcoma (75%) requires full chemotherapy protocol.

Clinical Presentation
History
- Pain: Progressive, worse at night
- Initially activity-related
- Becomes constant
- May wake from sleep
- NSAIDs initially helpful
- Develops over weeks-months
- May be warm to touch
- Firm, fixed to bone
- Skin changes rare
- Visible deformity late
- Pathological fracture (10%)
- Weight loss (late)
- Night sweats (rare)
- Respiratory symptoms (mets)
- Duration under 6 months typical
Physical Examination
Systematic Assessment:
-
Inspection:
- Swelling/mass location
- Skin changes (rare, late)
- Muscle wasting (adjacent)
- Limb length (if growth plate involved)
-
Palpation:
- Mass characteristics: Firm, fixed to bone, tender
- Warmth (increased vascularity)
- Range of motion (reduced if near joint)
- Lymph nodes (rarely involved - under 3%)
-
Neurovascular:
- Pulses (rarely compromised)
- Sensation (late involvement)
- Motor function
- Compartment tension
10% of osteosarcomas present with pathological fracture. This does NOT automatically preclude limb salvage but:
- Creates surgical challenge (contamination of fracture hematoma)
- May require modified chemotherapy timing
- Still achieves similar survival with careful planning
Differential Diagnosis
- Key Distinguishing Features
- Diaphyseal, permeative, onion-skin periosteal, smaller cell
- Key Distinguishing Features
- Older patients (40-60), axial, chondroid matrix (arcs/rings)
- Key Distinguishing Features
- Epiphyseal, eccentrically lytic, no matrix
- Key Distinguishing Features
- Systemic symptoms, sequestrum, involucrum
- Key Distinguishing Features
- Transverse, no soft tissue mass, healing callus
- Key Distinguishing Features
- Eccentric, expansile, fluid levels on MRI
Investigations
Imaging Protocol
First-Line Investigation - Essential Characteristics:
-
Location:
- Metaphyseal (most common)
- Eccentric or central
-
Matrix:
- Osteoid production (cloud-like density)
- "Cumulus cloud" appearance
- Dense sclerotic areas
-
Periosteal Reaction:
- Sunburst/Spiculated: Pathognomonic
- Codman Triangle: Elevated periosteum at margins
- Indicates aggressive behavior
-
Margins:
- Permeative/moth-eaten (aggressive)
- Wide zone of transition
- Cortical destruction
-
Soft Tissue:
- Extraosseous mass
- May show calcification
These findings together create the classic "aggressive bone lesion" appearance.


Biopsy Principles
The biopsy is the MOST IMPORTANT step in diagnosis:
- MUST be planned with definitive surgeon
- Wrong approach contaminates compartments
- Biopsy tract excised with specimen
- Violating these principles may necessitate amputation
Biopsy Technique:
- Pros
- Less contamination, outpatient
- Cons
- May miss diagnosis (sampling)
- Indication
- Preferred in most centers
- Pros
- More tissue, higher accuracy
- Cons
- More contamination
- Indication
- If core non-diagnostic
- Pros
- Diagnostic + therapeutic
- Cons
- Contraindicated
- Indication
- Never for suspected osteosarcoma
Biopsy Rules:
- Longitudinal incision along planned resection
- Avoid contaminating neurovascular structures
- Through muscle (not between compartments)
- Meticulous hemostasis
- Mark biopsy site for excision

Non-Operative Management
Chemotherapy Protocol
MAPMAP Chemotherapy
Hook:MAP your treatment - all 3 drugs needed for optimal survival.
- Duration: 8-12 weeks (2-4 cycles)
- Purpose: Shrink tumor, treat micrometastases, assess response
- Response assessment: Tumor shrinkage on imaging (not reliable)
- Duration: 12-29 weeks additional
- Total treatment: Approximately 1 year
- Modifications based on histologic response
Chemotherapy Toxicities
- Major Toxicity
- Mucositis, nephrotoxicity, hepatotoxicity
- Monitoring
- Levels, renal function
- Management
- Leucovorin rescue, hydration
- Major Toxicity
- Cardiotoxicity (dose-dependent)
- Monitoring
- Echo/MUGA
- Management
- Lifetime dose limit 450mg/m²
- Major Toxicity
- Nephrotoxicity, ototoxicity, neuropathy
- Monitoring
- Cr, audiometry
- Management
- Hydration, dose adjustment
Doxorubicin Cardiotoxicity: Cumulative dose-dependent. Lifetime limit typically 450mg/m². Echo/MUGA before each cycle. Irreversible cardiomyopathy if exceeded.
Indications for Chemotherapy
- Neoadjuvant
- Yes
- Adjuvant
- Yes
- Notes
- Standard MAP protocol
- Neoadjuvant
- Yes
- Adjuvant
- Yes
- Notes
- Same as conventional
- Neoadjuvant
- No
- Adjuvant
- No
- Notes
- Wide resection only
- Neoadjuvant
- Consider
- Adjuvant
- Consider
- Notes
- Case-by-case decision
- Neoadjuvant
- Yes
- Adjuvant
- Yes
- Notes
- Full protocol
Management Algorithm

Standard Treatment Pathway:
DIAGNOSIS CONFIRMED
↓
STAGING (MRI, CT Chest, Bone Scan)
↓
┌───────────────────┐
│ NEOADJUVANT CHEMO │ → 8-12 weeks MAP protocol
│ (Pre-operative) │
└─────────┬─────────┘
↓
RESTAGING
↓
┌───────────────────┐
│ WIDE RESECTION │ → Limb salvage (80-90%) or Amputation
│ ± Recon │
└─────────┬─────────┘
↓
HISTOLOGIC ASSESSMENT
(% tumor necrosis)
↓
┌───────────────────┐
│ ADJUVANT CHEMO │ → Continue/modify based on response
│ (Post-operative) │
└───────────────────┘
Key point: Surgery is performed AFTER neoadjuvant chemotherapy to assess histologic response.
Surgical Technique
Surgical Principles
Margin Requirements:
- Wide Margin: Minimum 1-2cm of bone beyond tumor
- Cuff of Normal Tissue: Must include reactive zone
- Biopsy Tract: Excise with specimen
- Skip Lesions: Must be included in resection
Limb Salvage Options
- Most common reconstruction
- Distal femur, proximal tibia, proximal humerus
- Allows early mobilization
- Immediate stability
- Early weight-bearing
- No donor site morbidity
- Mechanical failure (5-10 year revision)
- Infection (5-15%)
- Aseptic loosening
- Limited lifespan in young patients
- For skeletally immature patients
- Non-invasive lengthening available
- Multiple lengthening procedures required
Endoprosthesis remains the gold standard for most limb salvage reconstructions.
Amputation Considerations
- Neurovascular encasement (not reconstructable)
- Massive soft tissue involvement
- Poor response to chemotherapy with progression
- Pathological fracture with contamination
- Patient preference
- Infection precluding salvage
- Expected non-functional limb
- Above-knee for distal femur tumors
- Hip disarticulation for proximal femur
- Forequarter for proximal humerus (rarely needed)
Survival Equal: Multiple studies confirm limb salvage and amputation have equivalent oncologic outcomes when appropriate margins achieved. Limb salvage preferred when feasible due to better function and quality of life.
Complications

Chemotherapy Complications
- Agent
- Doxorubicin
- Incidence
- 5-10%
- Prevention/Management
- Dose limit 450mg/m², serial Echo
- Agent
- Cisplatin, MTX
- Incidence
- 10-20%
- Prevention/Management
- Hydration, dose adjustment
- Agent
- Cisplatin
- Incidence
- 10-30%
- Prevention/Management
- Audiometry, dose modification
- Agent
- MTX
- Incidence
- 40-60%
- Prevention/Management
- Leucovorin rescue, supportive care
- Agent
- All agents
- Incidence
- Universal
- Prevention/Management
- G-CSF, transfusions
- Agent
- All agents
- Incidence
- 2-5%
- Prevention/Management
- Long-term surveillance
Surgical Complications
- Wound infection/dehiscence (10-15%)
- Flap necrosis
- Deep vein thrombosis
- Neurovascular injury
- Periprosthetic fracture
- Aseptic loosening (30% at 10 years)
- Prosthesis failure/breakage
- Infection (5-15% lifetime)
- Leg length discrepancy
- Amputation (10-15% conversion)
- Non-union (15-30%)
- Fracture (15-20%)
- Resorption
- Disease transmission (rare)
- Infection (10-15%)
Local Recurrence
- Inadequate margins
- Poor histologic response
- Skip lesion missed
- Pathological fracture
- Biopsy tract violation
- Re-staging (local + systemic)
- Further resection if possible
- Amputation if no salvage option
- Chemotherapy if not previously given
- Prognosis worse (30-40% survival)
Postoperative Care
Immediate Postoperative Period
- ICU/HDU for 24-48 hours (major surgery)
- DVT prophylaxis (mechanical + chemical)
- Wound assessment (skin flaps, drain output)
- Pain management (multimodal analgesia)
- Limb elevation
- Physiotherapy: ROM exercises
- Weight-bearing: Depends on reconstruction
- Endoprosthesis: Touch weight-bearing → progressive
- Allograft: Protected weight-bearing 6-12 weeks
- Wound care: Watch for infection/dehiscence
- Chemotherapy: Resumes when wound healed (usually week 3-4)
Rehabilitation Protocol
- Timeline
- 0-6 weeks
- Goals
- Wound healing, ROM
- Activities
- Bed exercises, transfer training
- Timeline
- 6-12 weeks
- Goals
- Strength, progressive WB
- Activities
- Gait training, strengthening
- Timeline
- 3-6 months
- Goals
- Full function
- Activities
- Sport-specific training
- Timeline
- Ongoing
- Goals
- Monitor function
- Activities
- Activity modification as needed
Follow-up Surveillance
- Every 3 months: Clinical exam, chest X-ray
- Every 6 months: CT chest, local imaging
- Every 6 months: Clinical exam, chest X-ray
- Annual: CT chest
- Annual clinical and radiographic review
- Late recurrence possible (rare after 10 years)
- Monitor for late effects of chemotherapy
Outcomes/Prognosis
Survival Rates
- 5-Year Survival
- 60-70%
- Notes
- Majority of presentations
- 5-Year Survival
- 20-30%
- Notes
- 15-20% have lung mets at presentation
- 5-Year Survival
- 75-80%
- Notes
- Strongest prognostic factor
- 5-Year Survival
- 50-55%
- Notes
- Still benefits from adjuvant chemo
- 5-Year Survival
- 30-40%
- Notes
- Depends on resectability
Prognostic Factors
- Favorable
- Over 90% necrosis
- Unfavorable
- Under 90% necrosis
- Favorable
- Localized disease
- Unfavorable
- Metastatic at diagnosis
- Favorable
- Extremity
- Unfavorable
- Axial skeleton, pelvis
- Favorable
- Under 8cm
- Unfavorable
- Over 8cm, skip lesions
- Favorable
- Normal
- Unfavorable
- Elevated
- Favorable
- Wide/negative
- Unfavorable
- Marginal/positive
SMARTOsteosarcoma Prognosis
Hook:SMART prognosis assessment.
Functional Outcomes
- MSTS functional score: 70-85%
- Most return to normal daily activities
- Competitive sports: Limited/modified
- Prosthesis revision: Expected at 10-15 years
- Prosthetic fitting: 2-3 months post-op
- Above-knee: 60-70% MSTS score
- Quality of life: Similar to limb salvage
- Energy expenditure: Higher for ambulation
Germline Predisposition Syndromes: the Genetics Behind Osteosarcoma
The risk-factors card lists Li-Fraumeni, hereditary retinoblastoma and Rothmund-Thomson and notes a 2-5% secondary-malignancy rate, but the topic never develops the genetics - yet the germline predisposition syndromes are high-yield and change how you counsel a young patient and their family. (Paget-associated secondary osteosarcoma is developed in the paget-sarcoma topic; this is the inherited/germline dimension.)
- Li-Fraumeni syndrome (germline TP53). A loss-of-function germline mutation in the TP53 tumour-suppressor gives a very high lifetime cancer risk, with osteosarcoma one of the classic component tumours (alongside soft-tissue sarcoma, breast cancer, brain tumours, adrenocortical carcinoma and leukaemia). An osteosarcoma in a very young child, multifocal disease, or a strong family cancer history should prompt consideration of Li-Fraumeni, referral for genetic counselling and germline testing, and awareness of the lifelong multi-cancer surveillance these families need.
- Hereditary retinoblastoma (germline RB1). Survivors of bilateral (germline) retinoblastoma carry a markedly increased risk of second cancers, and osteosarcoma is the single most common second malignancy - both spontaneously and, importantly, within a prior radiotherapy field because the retinoblastoma-treatment RB1-deficient tissue is radiosensitive. A history of childhood retinoblastoma in an osteosarcoma patient is a major red flag.
- RecQ-helicase (DNA-repair) syndromes. Rothmund-Thomson syndrome (RECQL4), and to a lesser extent Bloom and Werner syndromes, are autosomal-recessive DNA-repair disorders with an increased osteosarcoma risk - typically presenting younger and sometimes multifocally.
- Why it matters clinically. Recognising a predisposition syndrome triggers germline testing and genetic counselling, changes surveillance (the patient and relatives are at risk of further cancers), and informs treatment caution - particularly minimising radiotherapy exposure in RB1 and DNA-repair-defective patients, who are prone to radiation-induced second tumours.
Q: Which inherited syndromes predispose to osteosarcoma? A: Li-Fraumeni (germline TP53) - osteosarcoma is a classic component tumour; hereditary (bilateral) retinoblastoma (germline RB1) - osteosarcoma is the commonest second malignancy, especially in a prior radiotherapy field; and the RecQ-helicase DNA-repair syndromes - Rothmund-Thomson (RECQL4), Bloom, Werner. A very young, multifocal, or strong-family-history osteosarcoma warrants germline testing and genetic counselling, and radiotherapy should be minimised in RB1/DNA-repair patients.
Radiation-Induced Osteosarcoma and the Cahan Criteria
The topic lists prior radiation therapy as a risk factor and a 2-5% secondary-malignancy rate, and notes a secondary peak in older adults, but never develops radiation-induced sarcoma - a discrete, examinable entity with its own diagnostic criteria.
- What it is. A secondary sarcoma arising in a previously irradiated field, usually years to decades after radiotherapy for a different (often childhood) cancer. Osteosarcoma is the most common radiation-induced bone sarcoma, and the risk is dose-dependent and higher in genetically susceptible patients (notably germline RB1 retinoblastoma survivors and DNA-repair syndromes).
- The Cahan criteria (how it is defined). A post-radiation sarcoma is classically diagnosed when: (1) the tumour arises within the prior radiation field; (2) there is a latency period (typically several years - often five or more); (3) the sarcoma is histologically proven and distinct from the original irradiated lesion; and (4) the irradiated tissue was normal, or a different tumour type, before radiotherapy.
- Why it matters. Radiation-induced osteosarcoma tends to occur at older ages and in axial or previously-irradiated sites, is often higher-stage at presentation, and carries a worse prognosis than conventional extremity osteosarcoma. The surgical principles are unchanged (wide resection, chemotherapy for high-grade disease), but re-irradiated, scarred, hypovascular tissue makes resection and reconstruction harder - and it reinforces the case for minimising and carefully planning radiotherapy in children, especially those with a genetic predisposition.
Q: How is radiation-induced osteosarcoma recognised? A: By the Cahan criteria - a histologically-proven sarcoma, distinct from the original lesion, arising within a prior radiation field after a latency period (often five or more years), in tissue that was normal or a different tumour before radiotherapy. Osteosarcoma is the commonest radiation-induced bone sarcoma, is more frequent in RB1 survivors and DNA-repair syndromes, presents at older ages/axial sites, and has a worse prognosis than conventional osteosarcoma.
Guidelines, Registries & Global Practice
Global Epidemiology
- Incidence approximately 3-4 per million per year worldwide, the most common primary bone sarcoma of childhood and adolescence
- Bimodal distribution: a dominant adolescent peak (skeletal growth spurt) and a smaller secondary peak over 60 (often Paget-associated or radiation-induced), the latter carrying a markedly worse prognosis
- Outcomes plateaued internationally since the 1980s: 60-70% 5-year survival for localised disease, 20-30% for metastatic disease at presentation, with no major survival gain from chemotherapy intensification (EURAMOS-1)
Major Guidelines Side by Side
- Core recommendations
- MAP backbone; wide resection with limb salvage where margins achievable; metastasectomy for resectable lung disease
- Core recommendations
- Treat in reference sarcoma centres; neoadjuvant MAP, surgery, response-adapted continuation; no benefit from adding ifosfamide/etoposide for poor responders
- Core recommendations
- Mandatory referral to a recognised bone-sarcoma centre before biopsy; biopsy by (or directed by) the operating surgeon
- Core recommendations
- Plan biopsy along the definitive incision; excise the biopsy tract en bloc with the specimen
Registry and Network Evidence
- Cooperative groups (COSS, COG, EOI, SSG) feeding the EURAMOS collaboration provide the strongest randomised evidence base
- Bone-tumour endoprosthesis outcome data are pooled through specialist-centre series (eg Birmingham/Royal Orthopaedic Hospital) rather than national joint registries, which exclude tumour implants
- International tumour banking and biobanking underpin ongoing molecular and trial work
High- vs Limited-Resource Practice Variation
- High-resource settings: centralised multidisciplinary sarcoma units, neoadjuvant MAP, limb salvage in 80-90%, growing/expandable endoprostheses for skeletally immature children
- Limited-resource settings: later presentation with larger tumours and higher rates of pathological fracture, limited access to high-dose methotrexate monitoring, higher reliance on amputation and on biologic reconstruction (allograft, recycled autograft) where implants are unaffordable
Universal principle: Osteosarcoma must be managed by a specialist multidisciplinary sarcoma team, and biopsy must be planned with the definitive surgeon. Referral BEFORE biopsy is the single most important system-level safeguard worldwide.
Summary Points
High-Yield Take-Home Messages
- Osteosarcoma = Most common primary bone cancer in adolescents, defined by osteoid production
- Distal femur most common site (50%), "around the knee" in growing skeleton
- Sunburst + Codman triangle on X-ray = osteosarcoma until proven otherwise
- Biopsy MUST be planned with definitive surgeon - wrong approach contaminates compartments
- MRI entire bone - skip lesions occur in 1-5%, change surgical planning
- Neoadjuvant chemotherapy essential - MAP protocol (Methotrexate, Adriamycin, Platinum)
- Histologic response is strongest prognostic factor - over 90% necrosis = good response
- Limb salvage in 80-90% - equivalent survival to amputation
- Parosteal = exception - low-grade surface tumor, wide resection alone, no chemo
- Metastatic disease still aim for cure - complete resection of ALL disease improves survival
Controversies & Areas of Uncertainty
- Current position
- Standard postoperative MAP remains standard of care
- Why it remains unsettled
- EURAMOS-1 showed adding ifosfamide/etoposide (MAPIE) gave no survival benefit and more toxicity; no regimen has reliably rescued poor responders
- Current position
- Added to chemotherapy in some guidelines (eg EMA approval); not universally adopted (eg not FDA-approved)
- Why it remains unsettled
- INT-0133 reported a survival signal of borderline statistical interpretation; benefit and cost-effectiveness still debated
- Current position
- Negative margin with a cuff of normal tissue; exact millimetre threshold not fixed
- Why it remains unsettled
- Necrotic, chemotherapy-treated tumour blurs the reactive zone; response quality may matter more than absolute distance
- Current position
- No longer an absolute contraindication if good chemotherapy response and clear margins
- Why it remains unsettled
- Older data suggested higher local recurrence; modern series show comparable outcomes with careful selection
- Current position
- CT chest plus bone scan remain core; PET-CT increasingly used
- Why it remains unsettled
- PET-CT response (SUV change) is prognostic but has not replaced histologic necrosis as the reference standard
- Current position
- Regular chest imaging and local review for at least 5 years
- Why it remains unsettled
- Optimal frequency, modality (CXR vs CT) and radiation/cost trade-offs are not standardised internationally
Mnemonic Cards
DPHFOsteosarcoma Sites - DPHF
Hook:DPHF - 'Down Past the Hip to Flat' - Remember location distribution by frequency.
SCAMRadiographic Signs - SCAM
Hook:SCAM the X-ray - Classic aggressive bone tumor appearance on radiographs.
MAPMAP Chemotherapy
Hook:MAP your treatment - All 3 drugs needed for optimal survival in osteosarcoma.
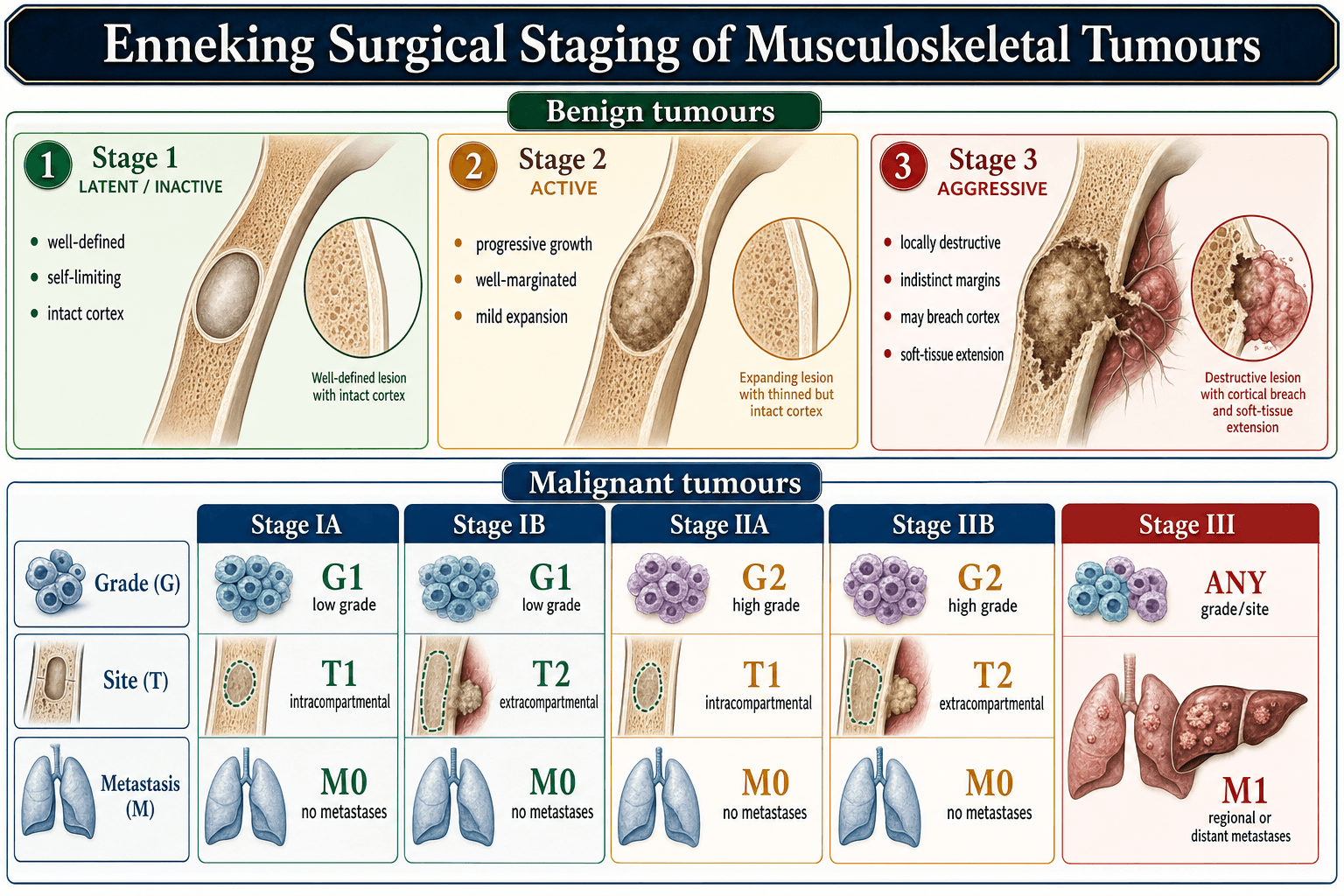
GTMEnneking Staging - GTM
Hook:GTM staging - Grade, Tumor site, Mets determine prognosis and margin requirements.
MCQ Practice Points
Q: What is the most common site for osteosarcoma? A: Distal femur (50%), followed by proximal tibia (25%), proximal humerus (10%). Remember: "Around the knee" in adolescents.
Q: What are the pathognomonic radiographic features of osteosarcoma? A: Sunburst periosteal reaction and Codman triangle. Also look for: permeative destruction, osteoid matrix (cloud-like), soft tissue mass.
Q: What is the standard chemotherapy regimen for osteosarcoma? A: MAP - high-dose Methotrexate (with leucovorin rescue), Adriamycin (doxorubicin), cisPlatin.
Q: What defines a good histologic response in osteosarcoma? A: Over 90% tumor necrosis in resected specimen. This is the strongest prognostic factor (5-year survival 75-80% vs 50-55% for poor response).
Q: Which osteosarcoma subtype does NOT require chemotherapy? A: Parosteal osteosarcoma - low-grade surface tumor treated with wide resection alone. 90-95% 5-year survival. Watch for dedifferentiation.
Common MCQ Scenarios
- Key Answer Point
- Osteosarcoma - biopsy with surgeon
- Key Answer Point
- Parosteal osteosarcoma - no chemo
- Key Answer Point
- Continue standard adjuvant chemo
- Key Answer Point
- Include in resection, not contraindication to limb salvage
- Key Answer Point
- Still attempt limb salvage with modified approach
- Key Answer Point
- Poor prognostic factor
- Key Answer Point
- Suspect secondary osteosarcoma
Self-Assessment Quiz
At a Glance Table
- Details
- Primary malignant bone tumor producing osteoid by malignant cells
- Details
- 3-4 per million per year (most common primary bone cancer in adolescents)
- Details
- Bimodal: 10-20 years (primary), over 60 (secondary - Paget's)
- Details
- Male to Female = 1.5:1
- Details
- Distal femur (50%), proximal tibia (25%), proximal humerus (10%)
- Details
- Pain + Mass + Restricted ROM
- Details
- Sunburst periosteal reaction + Codman triangle
- Details
- Neoadjuvant chemo → Wide resection → Adjuvant chemo
- Details
- 60-70% localized, 20-30% metastatic at presentation
- Details
- Histologic necrosis (over 90% = good response)
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-year-old boy presents with 3 months of worsening right knee pain. X-ray shows an aggressive metaphyseal lesion in the distal femur with a sunburst periosteal reaction and Codman triangle. How do you manage this patient?”
“A 35-year-old woman has a slowly enlarging mass on the posterior aspect of her distal femur for 2 years. X-ray shows a densely ossified surface lesion attached to the posterior cortex. Biopsy confirms low-grade parosteal osteosarcoma. How does management differ from conventional osteosarcoma?”
“A 16-year-old presents with a distal femur osteosarcoma. Staging CT chest reveals 3 pulmonary nodules consistent with metastatic disease. How does this change your management approach?”
CLINICAL FEATURES
- Distal femur most common (50%)
- Bimodal: adolescents + over 60 (Paget's)
- Sunburst + Codman triangle on X-ray
- Pain worse at night, progressive swelling
STAGING WORKUP
- MRI entire bone (skip lesions)
- CT chest (lung mets - 80% of distant disease)
- Bone scan (systemic staging)
- Biopsy planned with definitive surgeon
TREATMENT PROTOCOL
- Neoadjuvant: MAP chemo 8-12 weeks
- Wide resection (limb salvage 80-90%)
- Assess histologic necrosis (over 90% = good)
- Adjuvant chemotherapy to complete
SUBTYPES
- Conventional (75%): High-grade, needs chemo
- Telangiectatic: Lytic, same treatment
- Parosteal: Low-grade, NO chemo needed
- Periosteal: Intermediate, consider chemo
PROGNOSIS
- Localized: 60-70% 5-year survival
- Metastatic: 20-30% survival
- Over 90% necrosis: 75-80% survival
- Under 90% necrosis: 50-55% survival
EXAM TRAPS
- Biopsy through wrong approach
- Surgery without chemotherapy
- Missing skip lesions (MRI entire bone)
- Giving chemo for parosteal type
Evidence Base
- 57 extremity osteosarcomas treated with preoperative high-dose methotrexate, doxorubicin and BCD
- Histologic response (over 90% necrosis) used to tailor postoperative chemotherapy
- Poor responders salvaged by switching regimen: 32 of 35 (91%) remained disease-free short-term
- Established neoadjuvant chemotherapy and histologic response as the modern treatment paradigm
- Largest osteosarcoma trial: 2260 registered, 618 poor responders randomised (MAP vs MAPIE)
- Adding ifosfamide and etoposide (MAPIE) did NOT improve event-free survival (HR 0.98)
- MAPIE increased grade 3-4 toxicity (febrile neutropenia, non-haematological events)
- Defines standard postoperative MAP as standard of care even for poor responders
- Multi-institutional retrospective study of 227 distal femur osteosarcomas
- No difference in survival between limb-sparing surgery, above-knee amputation, or hip disarticulation (p=0.8)
- Local recurrence and metastasis rates comparable across groups
- Overall 5-year survival 55%; disease-free survival 42%
- 560 extremity high-grade osteosarcomas treated with neoadjuvant chemotherapy at Rizzoli
- On multivariate analysis only two factors independently predicted event-free survival
- Pre-treatment serum alkaline phosphatase (p=0.002) and chemotherapy-induced necrosis (p=0.0001)
- 5-year event-free survival 60%, overall survival 68%
- Musculoskeletal Tumor Society survey of 597 sarcoma biopsies across 21 institutions
- Diagnostic error rate 17.8%; biopsy problems altered management in 19.3% of patients
- Errors and complications two to twelve times higher when biopsy done at referring (non-treatment) centre
- 18 patients underwent unnecessary amputation due to biopsy-related problems
- 34 patients (15 osteosarcoma) after whole-bone resection and endoprosthetic reconstruction
- Cumulative 10-year implant survival 90% (Kaplan-Meier)
- Periprosthetic infection was the most common surgical complication
- Mean MSTS functional score 83% in disease survivors