Article summary
A detailed breakdown of the Single-Row vs. Double-Row debate. Does the biomechanical superiority of double-row repair translate to better clinical outcomes?
Educational content is reviewed for source visibility, editorial coherence, and correction readiness.
No individual clinician credential is claimed unless a named person is shown.
Verify before clinical use; this is not medical advice or a substitute for local guidance.
The debate between Single-Row (SR) and Double-Row (DR) rotator cuff repair is one of the most enduring controversies in shoulder surgery. It frequently pits the biomechanical purist against the clinical pragmatist. On paper and in the controlled environment of a biomechanics lab, the double-row repair—particularly the transosseous-equivalent (TOE) or suture bridge technique—is undeniably superior. It boasts higher ultimate load to failure, covers significantly more footprint area, and effectively suppresses harmful synovial fluid motion.
Yet, when we translate these laboratory triumphs into the clinic, patient-reported outcome measures (PROMs) often fail to show a statistically significant or clinically meaningful difference for the majority of tear sizes. This creates a challenging paradigm for orthopaedic surgery trainees preparing for fellowship exams: how do you justify implant cost and increased surgical time when the clinical superiority is debated?
This article comprehensively dissects the anatomy, biomechanics, health economics, and clinical evidence surrounding rotator cuff repair techniques. Our goal is to equip you with the knowledge not just to pass your orthopaedic exams (FRACS, FRCS, ABOS), but to make sound, evidence-based decisions in your future independent practice.
Examiners love this topic because it tests your ability to weigh biomechanical theory against clinical evidence. Be prepared to discuss the native anatomy of the footprint, the concept of pressurized footprint contact, and exactly which patient populations actually benefit from a double-row construct.
1. Surgical Anatomy: Understanding the Native Footprint
To optimize our repair strategy, we must intimately understand the target anatomy. The rotator cuff insertion on the greater tuberosity is not a mere line; it is a complex, three-dimensional, broad area of fibrocartilaginous attachment. Restoring this anatomy is the theoretical holy grail of rotator cuff surgery.
The Supraspinatus and Infraspinatus Insertion
- Dimensions: The supraspinatus footprint is roughly triangular. It measures approximately 25mm in the anterior-posterior dimension and 15mm in the medial-lateral dimension. The infraspinatus has a much longer insertion (up to 32mm anterior-posterior) and overlaps significantly with the supraspinatus near the bare area.
- The "Cable and Crescent": Described by Burkhart, this anatomical concept is crucial. The thick rotator cable transfers force and stress-shields the thinner, avascular crescent tissue. Repairs often depend on capturing this robust cable tissue.
- Sharpey's Fibers: The ultimate goal of any repair is biological healing—the recreation of a four-zone fibrocartilaginous transition (tendon, uncalcified fibrocartilage, calcified fibrocartilage, bone) via Sharpey's fibers. Healing requires stable contact area and minimized micromotion.
2. The Single-Row Repair (SR): Simplicity and Biology
Technique Overview: In a single-row repair, anchors are placed in a single linear configuration, typically at the lateral aspect of the footprint (near the greater tuberosity crest) or slightly medialized to reduce tension. Sutures are passed through the tendon edge and tied, bringing the tendon down to the bone.
Fixation Configurations
- Simple Stitches: Fast and technically straightforward, but provide only point compression and are prone to cutting through osteoporotic tendon ("cheese-wiring").
- Mattress Stitches: Provide a broader hold on the tendon and slightly better tissue compression against the bone compared to simple stitches.
- Modified Mason-Allen: Biomechanically superior for grasping the tendon in a single-row construct, capturing both medial-lateral and anterior-posterior fibers.
The Pragmatic Advantages (Pros)
- Operative Efficiency: SR is undeniably faster. In a busy public hospital list or an ambulatory surgery center, saving 15-20 minutes per case is significant.
- Health Economics: Uses fewer anchors (typically 1-2 depending on tear size), drastically reducing implant costs.
- Preservation of Vascularity: The rotator cuff relies on a delicate microvascular network. Over-tensioning complex constructs can cause strangulation and ischemia. SR repairs theoretically allow better perfusion to the critical healing zone at the tendon edge.
- Revision Bone Stock: If an SR repair fails, the medial footprint is largely virgin bone. This preserves invaluable real estate for a revision double-row repair or patch augmentation.
The Biomechanical Drawbacks (Cons)
- The "Windshield Wiper" Effect: Because the tendon is secured along a single axis, it can toggle or rotate around this line of fixation during active or passive shoulder motion.
- Synovial Fluid Leakage: SR repairs often fail to create a watertight seal at the medial articular margin. Synovial fluid contains lysozymes and prevents the formation of a stable fibrin clot, inhibiting the bone-tendon healing process.
- Limited Footprint Restoration: SR re-creates only a fraction (often less than 50%) of the native medial-lateral footprint width.
3. Double-Row (DR) and Transosseous-Equivalent (TOE) Repairs
The evolution from single to double row was driven by the desire to recreate the broad native footprint and maximize biomechanical strength.
Technique Overview (Suture Bridge / TOE):
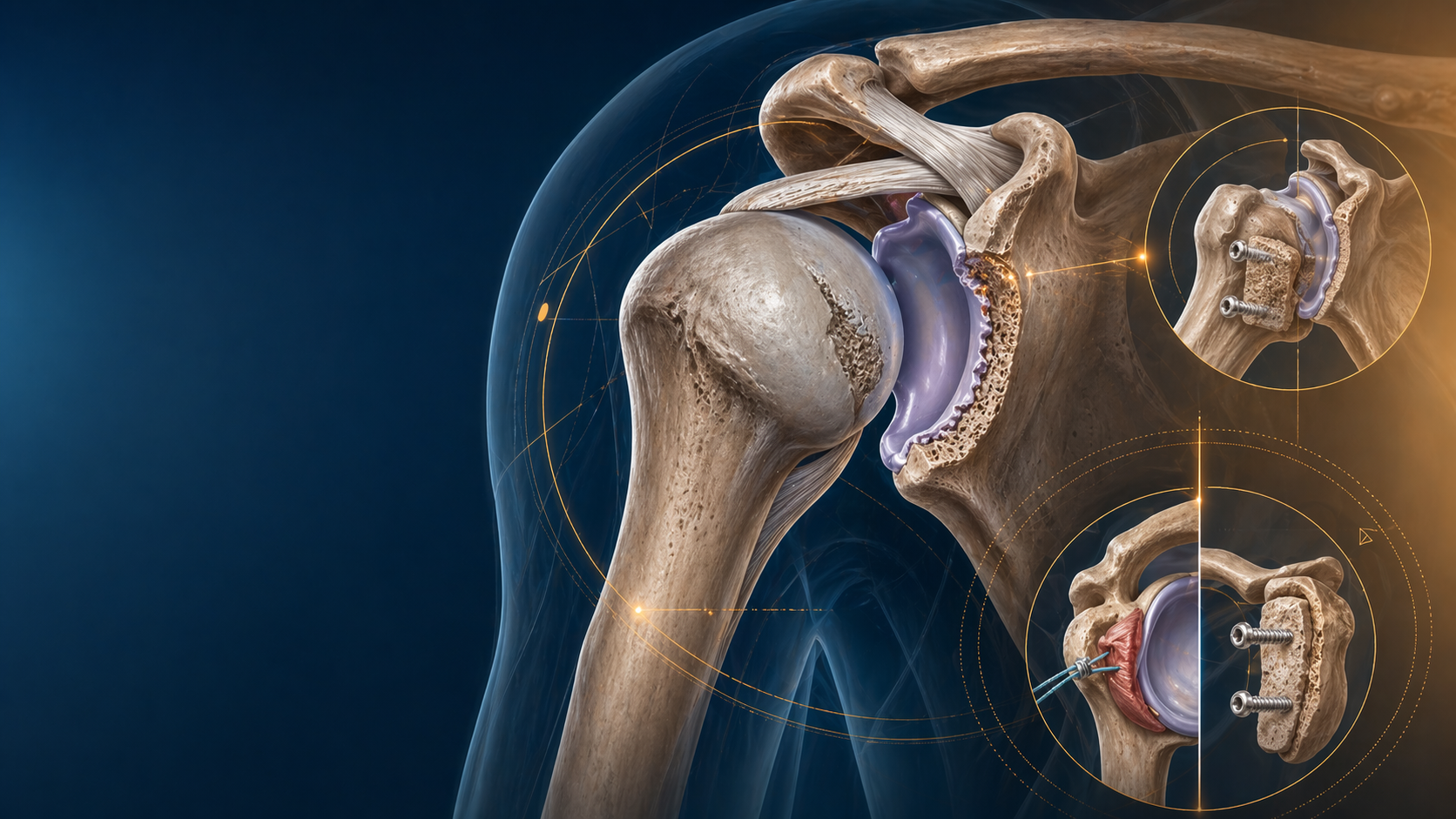
- Medial Row: Anchors (usually double-loaded) are placed precisely at the articular margin of the humeral head. Sutures are passed through the tendon, often via a mattress configuration.
- Lateral Row: Anchors (typically knotless) are placed roughly 1-2 cm lateral to the medial row, on the lateral cortex of the greater tuberosity.
- The Suture Bridge: Instead of simply tying the medial knots, the suture limbs are crisscrossed over the bursal surface of the tendon and locked into the lateral knotless anchors. This compresses the tendon flat against the footprint, akin to a seatbelt or a tied-down tarpaulin.
Biomechanical Triumphs (Pros)
- Maximal Footprint Restoration: The TOE technique covers nearly 100% of the native footprint area, maximizing the surface available for cellular integration.
- Pressurized Contact Area: It generates high, uniform compressive force between the tendon and the decorticated bone.
- The Water-Tight Seal: By compressing the medial edge precisely at the articular margin, it effectively blocks synovial fluid intrusion into the healing zone.
- Superior Load-to-Failure: DR constructs demonstrate significantly higher ultimate strength, stiffness, and yield load in cadaveric models compared to SR.
The Clinical and Technical Costs (Cons)
- Financial Burden: Utilizing 4 anchors instead of 2 effectively doubles the implant cost of the procedure.
- Technical Complexity: It requires more advanced arthroscopic skills, excellent suture management, and increased operative time.
- Type 2 Failures (Medial Cuff Failure): The "seatbelt" effect can be a double-edged sword. Excessive tension across the suture bridge can create a stress riser at the medial row or strangulate the blood supply. When TOE repairs fail, they often tear medial to the medial row anchors—leaving a pristine footprint but a catastrophically short, retracted tendon that is incredibly difficult to revise.
| Feature | Single-Row (SR) | Double-Row (TOE/Suture Bridge) |
|---|---|---|
| Footprint Coverage | Low (~40-50%) | High (~80-100%) |
| Synovial Seal | Poor | Excellent |
| Operative Time | Shorter | Longer |
| Implant Cost | Lower ($) | Higher ($$) |
| Failure Pattern | Pull-off from bone (Type 1) | Medial tear / Tissue failure (Type 2) |
| Tissue Strangulation Risk | Low | Moderate to High |
4. The Clinical Disconnect: Why Doesn't Double-Row Always Win?
If DR is a biomechanical masterpiece, why don't all Level I randomized controlled trials (RCTs) show it is clinically superior? This is the core of the "Biomechanics vs. Biology" paradox in orthopaedic surgery training.
The Evidence Summary for Fellowship Exams
When preparing for your fellowship exam preparation, you must nuance your answers based on tear size.
- Small and Medium Tears (<3cm): Level I evidence, including numerous systematic reviews and meta-analyses, consistently shows NO clinically significant difference in functional outcomes (ASES, Constant, UCLA scores), pain levels, or range of motion between SR and DR. For these tears, the biology is usually good, the tension is low, and a well-executed single row is "strong enough" to hold the tendon until biology takes over.
- Large and Massive Tears (>3cm): This is the critical inflection point where DR proves its worth. For large tears, studies consistently demonstrate significantly lower structural re-tear rates with double-row repair. The increased mechanical stability is required to overcome the higher resting tension of a chronically retracted, large tendon tear.
Landmark Literature to Quote
- The OASIS Trial: While early reports showed similar functional scores, long-term follow-ups of large cohorts suggest the re-tear rate for DR is roughly half that of SR for larger tears (e.g., ~20-25% for DR vs ~40-50% for SR).
- Carbonel et al. (Level I RCT): Demonstrated that while clinical scores were similar at 2 years, the MRI-confirmed healing rate was significantly higher in the double-row group for tears larger than 3cm.
5. Value-Based Care: The Cost-Utility Analysis
In modern orthopaedic practice, we cannot ignore health economics. We operate in an era of value-based care.
- A standard DR or TOE repair adds approximately 1,500 USD in implant costs per case compared to an SR repair.
- To justify this expense, the intervention must either prevent costly downstream events (like revision surgery) or provide a massive leap in patient quality of life.
- Low Value: For a 1.5cm crescent tear in a 65-year-old, spending the extra money on a DR provides no measurable functional benefit and does not significantly change the already low re-tear rate.
- High Value: For a 4cm U-shaped tear in a 50-year-old manual laborer, spending the extra $1,000 to halve the risk of a catastrophic re-tear—which would require a massively expensive revision surgery, superior capsular reconstruction, or reverse total shoulder arthroplasty—is highly cost-effective.
6. The Surgeon's Playbook: Decision-Making Algorithm
So, how do you synthesize this for your surgical practice and your oral exams? You must develop a tailored algorithm.
Indications for Single-Row Repair
- Tear Size: Small (<1cm) or Medium (1-3cm) crescent-shaped tears.
- Tear Type: Partial articular-sided tendon avulsion (PASTA) lesions that are taken down and completed to full thickness.
- Patient Profile: Elderly or low-demand patients where the primary surgical goal is pain relief, not absolute restoration of lifting strength.
- Tissue Quality: Degenerated, friable tendon that will "cheese-wire" if subjected to the high tension of a suture bridge.
- Bone Stock: Severe osteopenia or large cystic changes in the greater tuberosity where lateral row knotless anchors are at high risk of pulling out.
Indications for Double-Row (Suture Bridge / TOE)
- Tear Size: Large (>3cm) or Massive tears that can be adequately mobilized.
- Patient Profile: Young, active patients, manual laborers, and overhead athletes who require maximal postoperative strength and torque.
- Tear Geometry: L-shaped or U-shaped tears that require complex margin convergence followed by secure footprint fixation.
- Tissue Quality: Robust, thick tendon capable of withstanding the compressive forces of the suture bridge without ischemic necrosis.
- Revision Surgery: Assuming adequate bone stock remains, revising a failed SR with a biomechanically superior DR is standard practice.
7. Future Horizons: Beyond the Double Row
The orthopaedic community is recognizing that we may have hit the ceiling of purely mechanical solutions. Adding a 5th, 6th, or 7th anchor (so-called "triple row" constructs) rarely adds meaningful biomechanical strength. In fact, it often subtracts value by turning the greater tuberosity into "Swiss cheese," increasing the risk of postoperative fracture and severe tendon strangulation.
The future of rotator cuff repair lies in Bio-inductive and Biological Augmentation. Instead of adding more plastic and suture, surgeons are increasingly combining a solid mechanical repair (SR or DR) with biological overlays. This includes:
- Bovine or Porcine Dermal Patches: To thicken the native tissue and share the load.
- Recombinant Human Platelet-Derived Growth Factor (rhPDGF): To stimulate cellular proliferation.
- Subacromial Balloon Spacers: To depress the humeral head and protect the repair during the vulnerable early healing phase.
Conclusion
The "Single vs. Double Row" debate is not a binary, zero-sum game. It is a spectrum of indications that requires thoughtful surgical judgment.
- Single-Row is not an "inferior" legacy technique; it is a highly appropriate, cost-effective, biologically friendly, and highly successful operation for the vast majority of routine, degenerative rotator cuff tears.
- Double-Row is your "heavy-duty" biomechanical tool. It provides the essential mechanical stability and footprint restoration required for large tears, high-demand tissues, and young patients.
The hallmark of a master surgeon—and the exact trait examiners look for in orthopaedic surgery training—is not the ability to forcefully deploy a "one-size-fits-all" construct. It is the wisdom to match the biomechanical solution precisely to the patient's biological problem.
Related topics
Share this article
Useful for a journal club, study list, or teaching session.