Workhorse posterior approach for the posterior wall, posterior column and transverse fracture family
- The default posterior approach for posterior wall, posterior column, transverse and posterior-dominant T-type and associated patterns.
- It is NOT a classical internervous plane - gluteus maximus is split along its fibres, and that split denervates the inferior fibres; the safe proximal boundary is the superior gluteal neurovascular bundle exiting above piriformis.
- The sciatic nerve is THE critical structure - identify it early via the fat overlying quadratus femoris and protect it throughout.
- Hip extension and knee extension put the sciatic nerve on tension - keep the knee flexed (and avoid hip extension) to slacken it.
- This approach carries the highest heterotopic ossification risk of the standard acetabular approaches, so prophylaxis is standard practice.
When & Why
Indication. The Kocher-Langenbeck (K-L) approach is the workhorse posterior exposure for the acetabular fracture family that is accessible from behind. Use it for: - Posterior wall fracture causing hip instability or with a displaced or incongruent articular fragment (the primary determinant is instability, not wall size alone).
- Posterior column fracture displaced more than 2mm with articular incongruity.
- Transverse fracture when posterior displacement predominates.
- T-type fracture when the posterior component is primary.
- Transverse plus posterior wall (the classic indication) and posterior column plus posterior wall associated patterns.
- Associated posterior hip dislocation (closed reduction first, then staged ORIF) or a Pipkin femoral head injury requiring posterior access. The decision to operate rests on instability and incongruity, not a fixed wall percentage. Indicators that push toward fixation: - Articular step-off or gap more than 2mm on CT.
- Hip instability confirmed by examination under anaesthesia (EUA) with dynamic stress fluoroscopy - the reference standard. Static wall-percentage thresholds are unreliable: Firoozabadi and Tornetta found that roughly a quarter of EUA-unstable hips had a wall size under 20%, and fractures exiting near the dome behave unstably regardless of wall size.
- Marginal impaction of the posterior rim requiring elevation and grafting.
- Intra-articular fragments requiring removal, or a subluxed or non-concentric femoral head. Contraindications. Absolute: an active posterior wound infection, a Morel-Lavallee degloving lesion (delay until resolved), severe gluteal muscle necrosis, or medical unfitness for prolonged lateral decubitus positioning. Relative: an anterior column or wall as the primary injury (use the ilioinguinal or Stoppa approach instead), morbid obesity (positioning difficulty), previous posterior hip surgery with scarring, a pre-existing complete sciatic palsy (no protective function left to preserve), and both-column fractures (which usually need an anterior approach). Alternatives. Non-operative management with six to eight weeks of protected weight-bearing is reasonable only for a stable, congruent joint with less than 2mm displacement. Percutaneous fixation suits selected posterior column patterns. In the elderly, or with severe comminution and pre-existing arthritis, a total hip arthroplasty (sometimes with prior or concurrent fixation) may be the better reconstructive option. Consent. Quote the evidence-based outcomes: anatomic reduction is achievable in roughly 70 to 85 percent of operatively managed fractures (Matta reported 71 percent in a mixed series; isolated posterior wall reaches 97 percent anatomic in Moed's series), with good-to-excellent clinical results in around 75 to 80 percent when reduction is anatomic. Counsel specifically on the risks below.
- Rate
- Up to about 10%
- Detail
- Lower with meticulous identification and protection (near-negligible in expert series); higher when a dislocation has already injured the nerve
- Rate
- 2-10% (posterior wall)
- Detail
- Driven by the dislocation, not the approach; risk rises with delayed reduction
- Rate
- Up to about 50% without prophylaxis
- Detail
- Highest of the standard acetabular approaches; clinically significant (Brooker III-IV) in a smaller subset
- Rate
- 2-5%
- Detail
- Higher with an open injury or a Morel-Lavallee lesion
- Rate
- Correlates with reduction quality
- Detail
- The strongest predictor of long-term outcome; secondary THA in roughly 6 to 30%
- Rate
- Variable despite prophylaxis
- Detail
- Polytrauma raises the risk
Setup. General anaesthesia with muscle relaxation is mandatory (lateral decubitus precludes spinal alone). Give tranexamic acid 1g IV at induction (repeat at three hours), use a cell saver, and give cefazolin 2g IV within 60 minutes of incision (repeat every four hours or after 1.5L blood loss). Position the patient in lateral decubitus with the affected hip up, the pelvis perpendicular to the table (confirm on AP fluoroscopy before prepping), the hip flexed 30-40 degrees and the knee flexed 90 degrees to slacken the sciatic nerve. Pad the dependent axilla (axillary roll), the lateral malleolus (peroneal nerve) and the dependent knee. Prep from iliac crest to mid-thigh, including the posterior gluteal region and the knee (so flexion can be adjusted), and mark the incision before prep.
Hip and knee flexion relaxes the sciatic nerve and meaningfully reduces the risk of traction injury. I position with this in mind and reconfirm it whenever the nerve is being manipulated.
The Operation
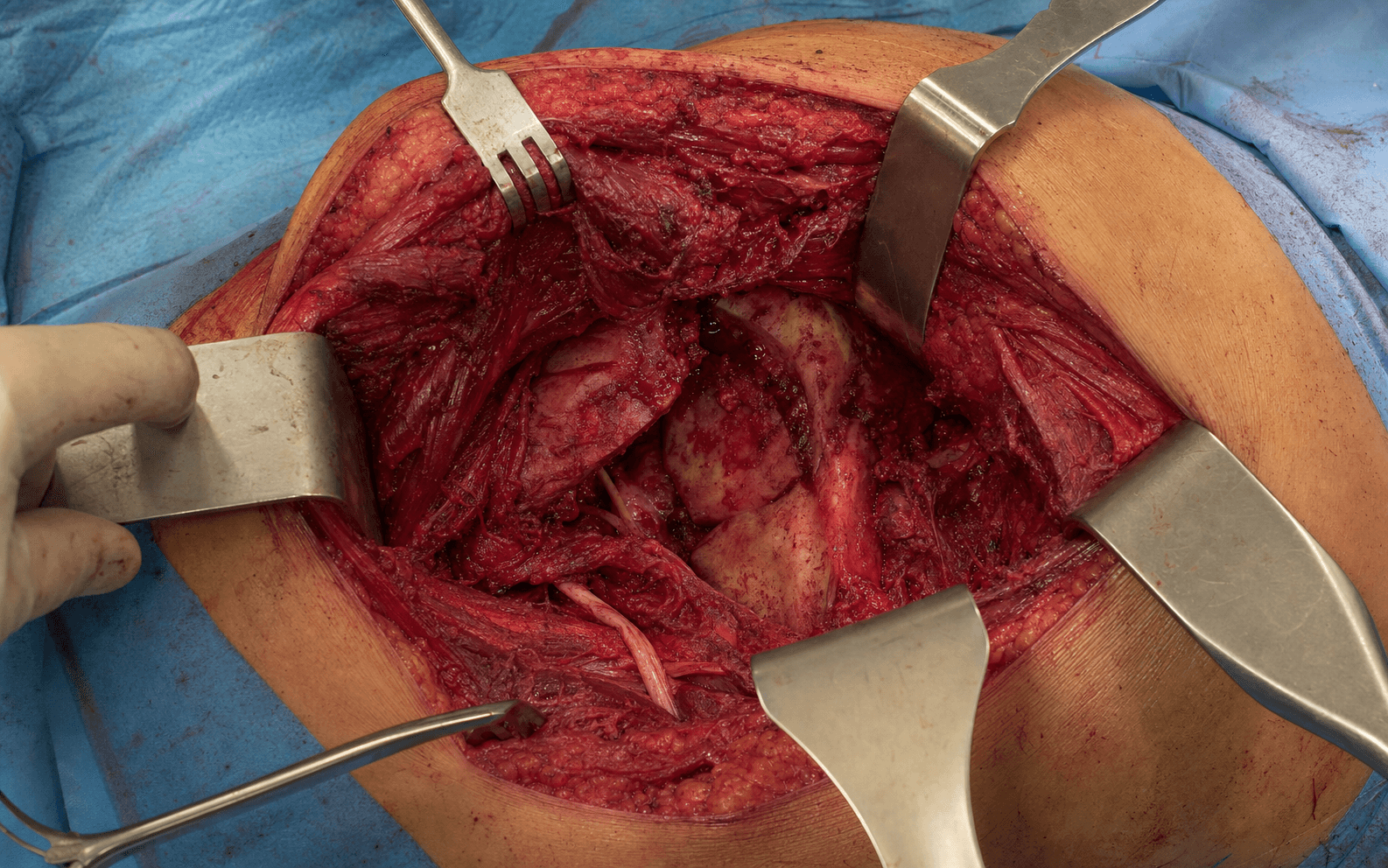
The goal is to expose the posterior column and wall, identify and protect the sciatic nerve throughout, reduce the column first (it is the stable reference), address any marginal impaction, restore the wall and buttress it, and then anatomically repair the short external rotators and capsule to restore the posterior restraints. The exposure is laid out as the first steps below - it is the heart of the operation - and is described in depth on the Kocher-Langenbeck approach to the hip page.
Operative sequence - exposure first, then fixation
- Lateral decubitus, affected hip up; pelvis perpendicular to the table (confirm on AP fluoroscopy).
- Hip flexed 30-40 degrees and knee flexed 90 degrees to slacken the sciatic nerve.
- Palpate the landmarks: posterior superior iliac spine (PSIS) (proximal start of the incision), the greater trochanter (the incision curves over its apex), the ischial tuberosity (distal limit of column exposure) and the greater sciatic notch (where the sciatic nerve exits - the danger zone).
- Prep from iliac crest to mid-thigh, including the knee; mark the incision before prep.
- A 15-20cm curvilinear, hockey-stick incision.
- Begin about 10cm distal to the PSIS, curve over the posterior aspect of the greater trochanter, and continue along the lateral femoral shaft for 8-10cm distal to the trochanter.
- The layers in turn are skin and subcutaneous tissue, the fascia lata (thick over the trochanter), and gluteus maximus (split in line with its fibres).
- Incise skin and subcutaneous fat, then the fascia lata over the greater trochanter in line with the skin.
- Identify the gluteus maximus fibres running obliquely (superomedial to inferolateral).
- Split gluteus maximus in line with its fibres using blunt finger dissection, and control bleeding from the superior and inferior gluteal vessels at the proximal extent of the split.
- Do NOT extend the split more than 4-5cm proximal to the trochanter (superior gluteal nerve - see safety note below).
- Identify the fat pad overlying quadratus femoris; the sciatic nerve lies in this fat on the posterior surface of the short external rotators and quadratus femoris.
- The nerve exits the pelvis through the greater sciatic notch, passing below piriformis in roughly 85-90 percent of people (variants pierce or pass above piriformis), then descends midway between the ischial tuberosity (medially) and the greater trochanter (laterally).
- Gently identify the cord-like nerve, trace it from the notch distally, and confirm it feels mobile and soft (not tethered).
- Protect it by keeping the tagged, reflected short rotators interposed between the nerve and your instruments, using only blunt retractors, keeping the knee flexed, and releasing retractors intermittently.
- Identify piriformis at the superior border of the greater trochanter; place a tagging suture (2-0 Ethibond) before release, then release it 1-2cm from its insertion with diathermy.
- Repeat for gemellus superior, obturator internus and gemellus inferior, tagging each.
- Preserve quadratus femoris and obturator externus whenever possible - they protect the deep branch of the medial femoral circumflex artery (see safety note).
- Reflect the tagged rotators posteriorly so they sit between the nerve and your retractors.
- Perform a posterior capsulotomy parallel to the acetabular rim and place stay sutures for later repair.
- Gently flex the hip and apply traction to visualise the joint.
- Remove all loose bodies - chondral fragments, bone and haematoma.
- Assess the articular surface systematically and actively look for marginal impaction (palpate the posterior rim for a depressed segment), cartilage damage, and any femoral head (Pipkin) injury.
- Place three blunt Hohmann retractors for exposure: one in the greater sciatic notch (protect the sciatic nerve), one on the ischium inferiorly, and one on the ilium or posterior column superiorly.
- Use a periosteal elevator to clear the fracture surfaces of haematoma and fibrous tissue.
- Identify all fragments and map out the fracture pattern before any reduction.
- Place a Schanz pin or ball-spike pusher in the ischial fragment and manipulate it to reduce the column to the intact ilium.
- Apply pointed (Weber) or Farabeuf reduction forceps; confirm reduction on the obturator oblique view (the best view for the posterior column) and aim for less than 1mm step.
- Hold the reduction with 2.0mm K-wires.
- If marginal impaction is present, elevate the impacted osteochondral fragment from within the joint using a Freer elevator or curette, restoring the spherical contour.
- Fill the metaphyseal void beneath the elevated fragment with cancellous autograft (femoral head if damaged by the dislocation, otherwise greater trochanter or iliac crest) to prevent re-collapse.
- Only then reduce the posterior wall fragments to the column with pointed forceps and hold with K-wires, assessing reduction on the iliac oblique view (the best view for the posterior wall).
- Contour a 3.5mm pelvic reconstruction plate (8-14 hole) to the posterior column, running from the ischium to the ilium.
- Use a minimum of three bicortical screws on each side of the fracture.
- Check screw lengths carefully to avoid joint penetration.
- Apply a 3.5mm plate perpendicular to the column plate (L or T configuration) so it buttresses the wall and prevents the fragments displacing into the joint.
- For small or comminuted fragments, use spring plates; alternatively use 3.5-4.0mm lag screws where geometry allows.
- Check all screw positions on the iliac oblique view (which shows the posterior wall and joint).
- Remove all retractors, reduce the hip and test stability with an axial load in flexion; range the hip through flexion and internal rotation checking for smooth, congruent motion.
- Confirm the final result on AP pelvis, inlet (25 degrees caudal), outlet (45 degrees cranial), obturator oblique (posterior column and anterior wall) and iliac oblique (anterior column and posterior wall - the key view for joint penetration).
- Confirm anatomic reduction (less than 2mm step), no intra-articular hardware, and no loose bodies.
- Repair the posterior capsule with 0-Vicryl.
- Repair the short external rotators using the tagged sutures, reattaching them to the posterior capsule or trochanteric insertion at appropriate tension (not over-tight, which limits motion).
- Close the gluteus maximus fascia with 1-0 Vicryl, place a deep drain (19Fr Blake) under gluteus maximus, close the fascia lata with 0-Vicryl, and close the skin (staples or 3-0 Monocryl subcuticular).
The superior gluteal neurovascular bundle exits the pelvis above piriformis, about 3-4cm from the acetabular rim, and supplies gluteus medius and minimus. Do NOT extend the split of gluteus maximus more than 4-5cm proximal to the greater trochanter, and never place retractors blindly into the greater sciatic notch.
The deep branch of the medial femoral circumflex artery (MFCA) is the dominant blood supply to the femoral head. It runs along the inferior border of obturator externus, passes deep (posterior) to the obturator externus tendon, then ascends to enter the capsule near the posterosuperior retinaculum. Obturator externus is the key protector. Preserve obturator externus and quadratus femoris; do not detach obturator externus, as dividing it close to the trochanter risks the MFCA and femoral head AVN.
Keep the knee flexed and avoid hip extension to slacken the nerve. Use only blunt retractors near the nerve, keep the tagged reflected rotators interposed between instruments and the nerve, release retractors intermittently rather than holding sustained traction, never extend the hip with retractors in place, and recheck the nerve position before placing any screws.
- Ischial screws: keep them short (about 20mm or less) - the pudendal vessels and rectum lie medially.
- Screws aimed toward the joint: confirm position on the iliac oblique view (which shows the posterior wall and joint).
- Beware anteriorly-directed long screws or drills perforating the quadrilateral surface (femoral neurovascular bundle across the front of the joint).
- If in doubt, use the shorter screw - safety over purchase.
Release the rotators close to their insertion and tag them with suture. This lets you anatomically repair the rotators and posterior capsule at closure, restoring the posterior soft-tissue restraints and reducing the risk of recurrent posterior instability. I regard it as a routine, non-optional part of closure.
The wall plate is a buttress - it prevents the wall from displacing into the joint. Position it perpendicular to the column plate, and use spring plates for comminuted fragments. The obturator oblique view shows the posterior column in profile (my go-to for column reduction); the iliac oblique view shows the posterior wall and is the key view for joint penetration.
Aftercare & Complications
Rehabilitation and weight-bearing | Phase | Timing | Weight-bearing / immobilisation | Focus | |-------|--------|--------------------------------|-------| | Immediate | Day 0-2 | Bed rest, ICU/HDU if polytrauma | Sciatic nerve checks every 2 hours for 24 hours; compare with the pre-operative baseline; monitor the drain | | Early | Week 1-6 | Toe-touch weight-bearing only | Walker or crutches; posterior hip precautions (no combined flexion, adduction and internal rotation); physiotherapy for ROM and strengthening | | Progression | Week 6-12 | Partial then full weight-bearing as radiographs allow | At 6 weeks continue toe-touch if still healing; 8-10 weeks progress to partial; 12 weeks full weight-bearing if healing | | Return to function | 3-12 months | Activity-graded | Sedentary work around 3-6 months; manual work 6-12 months; impact activities 9-12 months if fully healed | Most patients are followed at 6 weeks, 3 months, 6 months and 1 year, with a post-operative CT within 48 hours to confirm reduction and hardware position and a 6-week AP-and-Judet radiograph series. Long-term, monitor for post-traumatic arthritis (around 20-30 percent at 10 years), late-presenting AVN (6-24 months) and function-limiting HO. Heterotopic ossification prophylaxis is standard. Because gluteal muscle is split and stripped, the K-L approach has the highest HO rate of the standard approaches (up to about 50 percent without prophylaxis, though only a minority are clinically significant Brooker III-IV). Minimise soft-tissue stripping, achieve meticulous haemostasis, lavage bone debris, and leave a deep drain for 48-72 hours. Start prophylaxis within 24-72 hours: - Indomethacin (for example 25mg three times daily for a 3-6 week course), OR
- Single-fraction radiotherapy of about 700cGy within 72 hours - as effective as fractionated 1200cGy (Moed and Letournel), and preferred when NSAIDs are contraindicated. Deep vein thrombosis prophylaxis. LMWH (enoxaparin 40mg daily) from day 1, accepting that risk persists despite prophylaxis in polytrauma. Complications
- Recognition
- Usually not apparent intra-operatively; post-operative foot drop (peroneal division), weakness of ankle dorsi-/plantar-flexion, sensory change
- Prevention
- Identify early in the fat over quadratus femoris; keep the knee flexed; blunt retractors only; keep reflected rotators between instruments and nerve; release retractors intermittently
- Management
- Most are traction neuropraxias recovering over 6-18 months; AFO for foot drop; EMG at 6 weeks; explore if no recovery by 6 months
- Recognition
- Hip stiffness and pain with passive motion developing 6-12 weeks post-operatively; ossification in the surgical field graded by Brooker class
- Prevention
- Minimise stripping; meticulous haemostasis and lavage; deep drain 48-72h; indomethacin or single-fraction 700cGy XRT within 24-72h
- Management
- Physiotherapy to maintain ROM; surgical excision only for severe (Brooker III-IV) functional limitation, after maturation at 12-18 months, with re-prophylaxis
- Recognition
- Progressive hip pain 6-24 months post-operatively; MRI signal change; late femoral head collapse on X-ray
- Prevention
- Reduce an associated dislocation urgently (the dislocation, not the approach, drives risk); one gentle well-relaxed reduction attempt; preserve obturator externus and quadratus femoris; avoid excessive traction
- Management
- Non-weight-bearing if early; core decompression pre-collapse; THA if the head collapses
- Recognition
- Wound erythema or discharge; deep infection with systemic signs
- Prevention
- Antibiotics within 60 minutes (repeat 4-hourly or after 1.5L loss); meticulous haemostasis; deep drain; delay surgery for a Morel-Lavallee lesion
- Management
- Superficial: oral antibiotics and wound care. Deep: debridement, hardware retention if stable, 6 weeks IV antibiotics
- Recognition
- Progressive pain and stiffness; joint-space narrowing on radiographs
- Prevention
- Anatomic reduction (less than 2mm step) is the strongest modifiable protector
- Management
- Conservative measures; arthroplasty for end-stage disease
- Recognition
- Sense of instability or recurrent subluxation
- Prevention
- Anatomic reduction plus anatomic repair of the short rotators and posterior capsule
- Management
- Reassess fixation; revision stabilisation if genuinely unstable
Viva & Exam Focus
PGOGOQThe short external rotators of the hip
Strictly, the Kocher-Langenbeck is NOT a true internervous approach. Gluteus maximus is split along its fibres (it is not detached from its femoral insertion), and this split inevitably denervates the muscle fibres distal or inferior to the split, because the inferior gluteal nerve (L5, S1, S2) enters the muscle from its deep surface. The practical safe proximal boundary is therefore the superior gluteal neurovascular bundle, which exits through the greater sciatic notch above piriformis. So: "The K-L is not a true internervous approach - gluteus maximus is split along its fibres, which denervates the inferior portion; the structure defining the proximal safe limit is the superior gluteal neurovascular bundle above piriformis."
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man sustains a posterior wall acetabular fracture with an associated posterior hip dislocation, and presents four hours after the injury. Describe your management.”
“During a Kocher-Langenbeck approach for posterior wall ORIF the patient has a post-operative foot drop; the pre-operative sciatic examination was normal. How do you assess and manage this?”
“What is marginal impaction in posterior wall fractures and how do you manage it?”
Indications
- Posterior wall - if UNSTABLE (EUA is the gold standard, not a fixed wall percentage) or incongruent
- Posterior column displaced more than 2mm
- Transverse and T-type when posterior displacement predominates
- Transverse plus posterior wall (the classic indication)
- The default approach for the posterior-pattern fracture family
Key anatomy
- NOT a true internervous plane - gluteus maximus is SPLIT along its fibres (denervates the inferior portion)
- Proximal safe limit = the superior gluteal neurovascular bundle, exiting ABOVE piriformis
- Sciatic nerve: exits the notch (below piriformis in about 85-90 percent), lies in the fat over quadratus femoris
- MFCA deep branch: protected by obturator externus and quadratus femoris - preserve both to protect the femoral head supply
Sciatic nerve protection
- Keep the KNEE FLEXED and avoid hip extension to slacken the nerve
- Identify it early in the fat over the short rotators and quadratus femoris
- BLUNT retractors only; keep the tagged rotators between instruments and nerve
- Release retractors intermittently; never extend the hip with retractors in
- Iatrogenic injury up to about 10 percent (near-zero in expert hands) - document pre-operative function
Key surgical steps
- Reduce the column FIRST (obturator oblique view)
- Address marginal impaction BEFORE wall reduction
- Column plate along the posterior column from ischium to ilium
- Wall plate perpendicular as a BUTTRESS
- REPAIR the short rotators and posterior capsule (restores posterior restraints)
Complications
- Iatrogenic sciatic injury up to about 10 percent (mostly neuropraxia; near-zero with protection)
- HO up to about 50 percent without prophylaxis - the HIGHEST of the standard approaches - prophylax routinely
- AVN is dislocation-driven - reduce the dislocation urgently
- Post-traumatic arthritis correlates with reduction quality; secondary THA in a minority
Background & Evidence
Mechanism and epidemiology. Acetabular fractures are high-energy injuries. The classic mechanism for a posterior wall fracture (often with a posterior hip dislocation) is the dashboard injury - a flexed knee driven backward into the dashboard transmitting force through the femoral head to the posterior wall. Falls from height and motor-vehicle accidents account for most transverse and column patterns. Polytrauma is common, so an ATLS workup is mandatory, and the time from injury to reduction of any associated dislocation matters: a delay beyond about six hours increases the risk of femoral head AVN, and in posterior wall series a delay greater than 12 hours was an independent predictor of poor outcome (Moed 2002). The Judet-Letournel classification. Letournel and Judet divided acetabular fractures into elementary and associated patterns. The Kocher-Langenbeck approach addresses the posterior-accessible members of this system.
- Type
- Elementary
- Usual approach
- Kocher-Langenbeck (if unstable or incongruent)
- Type
- Elementary
- Usual approach
- Kocher-Langenbeck
- Type
- Elementary
- Usual approach
- K-L if posterior displacement predominates; otherwise ilioinguinal/Stoppa
- Type
- Associated
- Usual approach
- K-L when the posterior component is primary
- Type
- Associated
- Usual approach
- Kocher-Langenbeck (the classic indication)
- Type
- Associated
- Usual approach
- Kocher-Langenbeck
- Type
- Elementary / Associated
- Usual approach
- Anterior approach (ilioinguinal or Stoppa), not K-L
Imaging: the Judet series and CT. The Judet radiographic series defines what each oblique view shows - essential for both diagnosis and intra-operative assessment.
- Best demonstrates
- Overall alignment; roof-arc measurement
- Best demonstrates
- POSTERIOR COLUMN and anterior wall
- Best demonstrates
- Anterior column and POSTERIOR WALL (the key view for joint penetration)
References
Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury
- 262 displaced acetabular fractures operated within 21 days; reduction anatomic in 185 (71%).
- Clinical result excellent 40%, good 36% (good-to-excellent 76%), fair 8%, poor 16%.
- Anatomic reduction was the strongest modifiable predictor of a good clinical and radiographic outcome.
- Osteonecrosis in 3% and secondary total hip replacement in 6%; anatomic reduction rate fell with fracture complexity, older age and delay.
Results of operative treatment of fractures of the posterior wall of the acetabulum
- 100 unstable isolated posterior wall fractures treated by ORIF; reduction anatomic in 97.
- Good-to-excellent clinical result in 89 of 100 despite the deceptively 'simple' pattern.
- Risk factors for a poor result: delay greater than 12 hours to reduce an associated dislocation, age 55 or older, intra-articular comminution, and osteonecrosis.
- Strong association between final radiographic grade and clinical outcome.
Determining stability in posterior wall acetabular fractures
- 185 isolated posterior wall fractures assessed with examination under anaesthesia (EUA) and dynamic stress fluoroscopy as the reference standard.
- 23% of hips judged unstable on EUA had a wall size less than 20% - so small walls are NOT reliably stable.
- Fractures exiting closer to the acetabular dome (mean cranial exit 5.0mm unstable vs 9.5mm stable) were significantly more likely to be unstable.
- Static radiographic wall-percentage thresholds were unreliable predictors of stability.
Incidence of sciatic nerve injury in operatively treated acetabular fractures without somatosensory evoked potential monitoring
- 129 acetabular fractures via posterior or extensile approaches (65 Kocher-Langenbeck) without SSEP monitoring.
- Only one iatrogenic injury (a sensory deficit); no patient had exacerbation of a pre-existing nerve injury.
- With direct visualisation and protection of the sciatic nerve the iatrogenic injury rate was negligible.
- Authors concluded routine SSEP/EMG monitoring is not justified in experienced hands.
Low-dose irradiation and indomethacin prevent heterotopic ossification after acetabular fracture surgery
- 54 acetabular fractures via posterior or extended iliofemoral approaches given combined indomethacin plus perioperative irradiation.
- Indomethacin 25mg daily started within 24 hours and continued 4 weeks; irradiation as 700cGy single dose or 1200cGy in three fractions.
- 44 of 54 had NO heterotopic ossification and 10 had only Brooker class I; functional results good with no prophylaxis complications.
- A single 700cGy dose was as effective as 1200cGy in three fractions.
Ectopic ossification following total hip replacement: incidence and a method of classification
- Original description of the Brooker classification of heterotopic ossification around the hip.
- Class I = islands of bone; Class II = bone spurs leaving more than 1cm between opposing surfaces; Class III = spurs leaving less than 1cm; Class IV = apparent ankylosis.
- Higher Brooker grades correlate with reduced hip motion.
Foundational texts (not PubMed-indexed): - Kocher T. Textbook of Operative Surgery. 3rd ed. London: Adam and Charles Black; 1911. (early description of the posterior exposure)
- Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open reduction. J Bone Joint Surg Am. 1964;46:1615-1646. (Judet-Letournel classification and the formal Kocher-Langenbeck approach)
- Letournel E, Judet R. Fractures of the Acetabulum. 2nd ed. Berlin: Springer-Verlag; 1993. (definitive reference on acetabular fracture surgery)