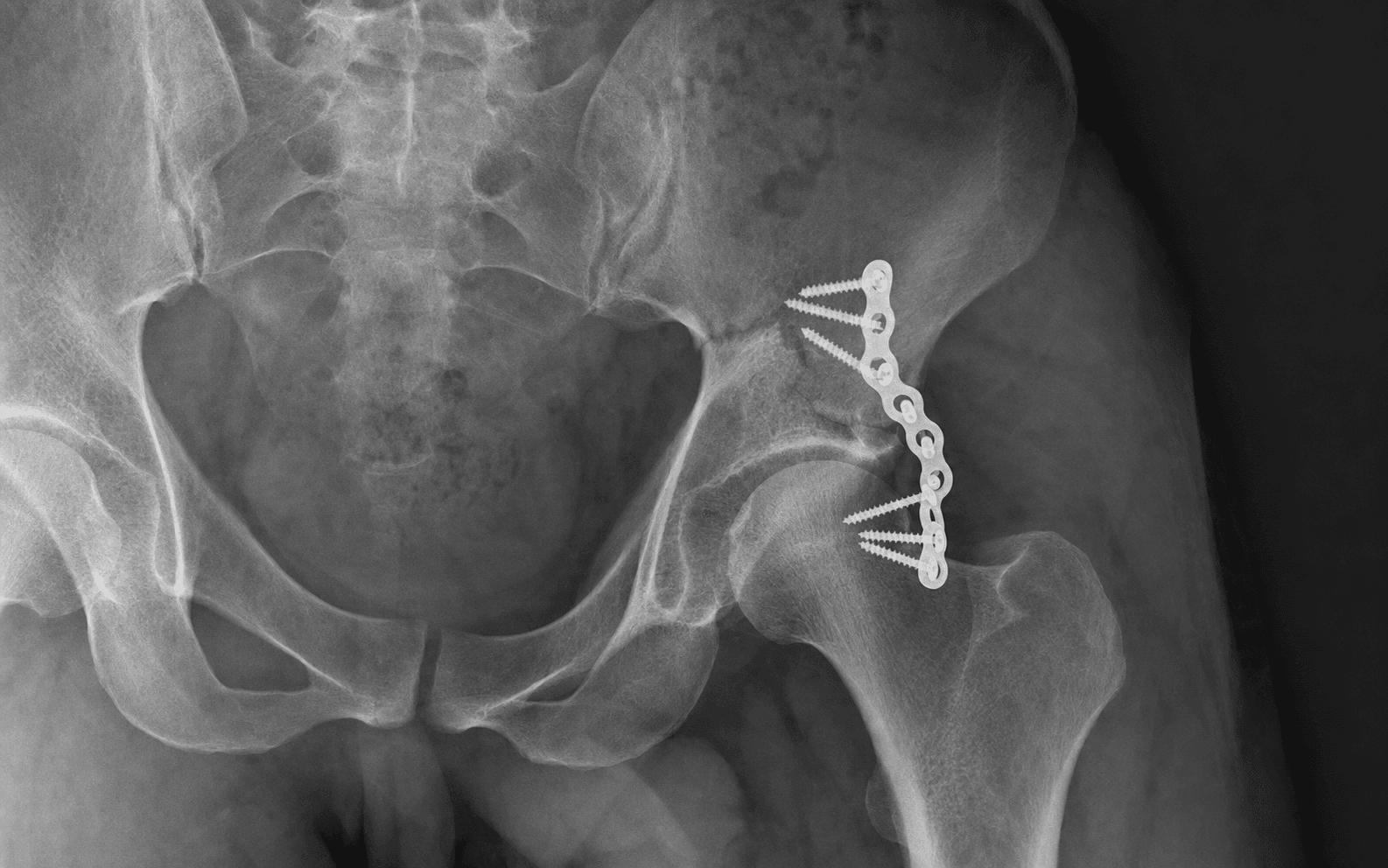
Kocher-Langenbeck Approach | Most Common Acetabular Fracture Pattern
- The posterior wall is the MOST COMMON elementary acetabular fracture pattern (25-30 percent), typically a dashboard injury and associated with posterior hip dislocation in about 70 percent.
- Stability is governed by the 40 percent rule: wall loss greater than 40 percent is unstable and needs ORIF; under 20 percent is stable; the 20-40 percent grey zone is settled by a dynamic stress test under fluoroscopy. Roof arc angles under 45 degrees on any view also indicate instability.
- Marginal impaction - cartilage-covered bone depressed at the fracture edge - is present in 50 percent and MUST be elevated and bone grafted, or early post-traumatic arthritis follows even with an anatomic wall reduction.
- A posterior hip dislocation is an EMERGENCY: reduce within 6 hours to limit femoral-head AVN (5-10 percent isolated, up to 25 percent if dislocation over 12 hours).
- Through the Kocher-Langenbeck approach the sciatic nerve (palsy 5-15 percent) and the medial femoral circumflex artery (the femoral head's blood supply) are the structures you must protect - identify the nerve early, vessel-loop it, and preserve the quadratus femoris.
- Heterotopic ossification prophylaxis is MANDATORY after this approach: indomethacin 75 mg daily for 6 weeks, or a single 7-8 Gy dose of radiation within 72 hours.
When & Why
The single question. You operate on a posterior wall fracture when the hip is unstable or incongruent - and you prove that with the wall percentage, roof arc angles, a dynamic stress test, and the CT. A concentrically reduced, stable hip with a small wall fragment is treated non-operatively. Indications
- Unstable hip: posterior wall involvement over 40 percent, a positive dynamic stress test, subluxation on static imaging, or a failed closed reduction of a dislocation.
- Articular incongruity: intra-articular fragments preventing a concentric reduction, marginal impaction requiring elevation, or a step or gap over 2 mm on CT.
- Mechanical block: incarcerated labral tissue, osteochondral fragments blocking reduction, or an associated femoral head fracture (Pipkin).
Greater than 40 percent wall loss is unstable (operate); under 20 percent is stable (non-operative); the 20-40 percent grey zone is decided by a dynamic stress test under fluoroscopy. Roof arc angles under 45 degrees on any view also mean instability, and over 55 degrees means a stable dome. The obturator oblique Judet view shows the posterior wall best because the wall faces the camera.
- Threshold
- Over 40 percent
- Decision
- Unstable - ORIF
- Threshold
- 20-40 percent
- Decision
- Grey zone - dynamic stress test decides
- Threshold
- Under 20 percent
- Decision
- Stable - non-operative if congruent
- Threshold
- Under 45 degrees
- Decision
- Unstable - ORIF
- Threshold
- Over 55 degrees
- Decision
- Stable dome - non-operative candidate
- Threshold
- Subluxation under posterior force at 90 degrees flexion
- Decision
- Unstable - ORIF
- Threshold
- Hip subluxation or incongruent reduction
- Decision
- Unstable - ORIF
Non-operative criteria and contraindications
- Non-operative requires ALL of: a concentrically reduced hip maintained, under 20 percent wall involvement, a negative dynamic stress test, and roof arc angles over 55 degrees on every view.
- Absolute contraindications: active infection, medically unfit for surgery, severe dementia with a non-ambulatory baseline, or posterior skin compromise precluding the approach.
- Relative: delay over 3 weeks with established callus, severe osteoporosis that will not hold fixation, a stable fracture under 20 percent, or an elderly low-demand patient with a concentrically reduced hip. Timing
- Hip dislocation is an emergency: reduce within 6 hours - AVN risk climbs steeply after 6-12 hours.
- Definitive ORIF: 3-10 days, after swelling resolves but before callus forms.
- Over 3 weeks: significantly more difficult; consider specialist referral.
- Figure
- 80-90 percent
- Note
- With anatomic reduction; may need THA in 10-20 percent long-term
- Figure
- 5-15 percent (1-3 percent permanent)
- Note
- Mostly neuropraxia; peroneal division more often affected
- Figure
- 20-30 percent without prophylaxis
- Note
- Falls to 5-10 percent with indomethacin or radiation
- Figure
- 20-40 percent long-term
- Note
- Tracks reduction quality
- Figure
- 5-10 percent
- Note
- Up to 25 percent if dislocation over 12 hours
- Figure
- 2-5 percent superficial, 1-3 percent deep
- Note
- Higher with an open injury or delay
- Figure
- 5-10 percent DVT, 1-2 percent PE
- Note
- Chemical prophylaxis is routine
- Figure
- 30-50 percent
- Note
- Blood loss typically 500-1500 mL; cell saver used
The Operation
The goal is an anatomic, stable reconstruction of the posterior wall through the Kocher-Langenbeck approach: identify and protect the sciatic nerve and the femoral head's blood supply, reduce the wall and any marginal impaction, hold it with lag screws and a buttress plate, and repair the posterior soft-tissue sleeve. The exposure is laid out in full below (and in depth on the Kocher-Langenbeck approach page).
Operative sequence
- Lateral decubitus, affected side up, on a beanbag or pegboard; axillary roll to protect the brachial plexus.
- Pad every bony prominence - fibular head (peroneal nerve), lateral malleolus, and the contralateral greater trochanter.
- General anaesthesia with muscle relaxation; arterial line, large-bore access, and a cell saver (blood loss typically 500-1500 mL). Induced hypotension (MAP 60-70 mmHg) may be used.
- Cefazolin 2 g IV within 60 minutes of incision (clindamycin 900 mg if penicillin-allergic); redose at 4 hours or 1500 mL blood loss.
- Confirm a radiolucent table and C-arm access for AP, obturator oblique and iliac oblique views before prepping.
- Palpate the PSIS, the greater trochanter, and the ischial tuberosity.
- Mark a curved incision from the PSIS toward the greater trochanter (apex at the trochanter), then distally along the posterior femoral shaft - total length 15-20 cm.
- Incise skin and subcutaneous tissue; identify the fascia lata and gluteus maximus fibres.
- Split gluteus maximus bluntly in the line of its fibres (superolateral to inferomedial): proximally between the upper one-third and lower two-thirds, distally posterior to the iliotibial band.
- Stay inferior to a point 4-5 cm above the greater trochanter to avoid the superior gluteal nerve.
- Palpate the greater sciatic notch and identify the piriformis tendon (the most superior rotator).
- The sciatic nerve exits below piriformis and lies 2-3 cm medial to the acetabular rim; gently mobilise it and protect it with a vessel loop for the rest of the case.
- Working superior to inferior, identify Piriformis, Gemellus superior, Obturator internus, Gemellus inferior, and Quadratus femoris.
- Tag each tendon with a heavy suture for later repair, then divide them about 1 cm from their trochanteric insertion; preserve the muscle bellies for vascularity.
- Leave the quadratus femoris intact - the medial femoral circumflex artery runs on its proximal border and supplies the femoral head.
- Flex and internally rotate the hip to relax the structures and improve exposure.
- Palpate the femoral head through the intact capsule, then make a T-shaped or inverted-L capsulotomy along the acetabular rim and down the femoral neck.
- Limit anterior capsular dissection to preserve the MFCA and its retinacular vessels.
- Identify the posterior wall fragment(s), assess comminution, extract intra-articular debris, and look specifically for marginal impaction (present in 50 percent).
- Place a cobra retractor on the ischium inferiorly and a Hohmann on the ilium superiorly, avoiding excess traction on the nerve.
- Clear the fracture surfaces of soft tissue and clot; use Schanz pins in the ilium or ischium as joysticks, ball-spike pushers for fine control, and pointed reduction clamps for provisional fixation.
- Goal: anatomic reduction - step and gap both under 2 mm, ideally under 1 mm at the weight-bearing dome; outcome tracks reduction quality.
- For marginal impaction, make a window in the wall fragment, elevate the depressed cartilage with a curved osteotome until flush, bone-graft the void, and support it with subchondral screws if needed before reducing the wall.
- Hold the reduction with pointed clamps (several for comminuted patterns), confirmed by direct vision and fluoroscopy.
- Drill perpendicular to the fracture plane, overdrill the near cortex for a glide hole, and insert a 3.5 mm cortical screw for interfragmentary compression - typically 2-4 lag screws.
- Aim from posterior toward anterosuperior at roughly 45 degrees cranial; palpate the joint surface to avoid intra-articular penetration.
- Apply a 3.5 mm pelvic reconstruction plate (pre-contoured posterior wall plate, or spring plates for small or comminuted fragments) along the posterior column.
- Engage 3-4 bicortical screws in the ilium above the fracture and 3-4 in the ischium below; additional screws pass through the plate into the wall fragment.
- Contour the plate precisely to the posterior column with bending irons - poor contour means loss of reduction as screws are tightened.
- Remove provisional clamps and palpate the articular surface through the capsulotomy.
- Stress-test the hip: flex to 90 degrees and apply a posterior force with internal rotation - it must not subluxate.
- Confirm on fluoroscopy in all four views: AP pelvis (concentric reduction, no roof step), obturator oblique (wall reduction - best view), iliac oblique (column integrity), and lateral (femoral head congruity).
- Repair the posterior capsule with interrupted number-1 absorbable sutures - this adds stability to the construct.
- Repair the short external rotators to the greater trochanter with heavy non-absorbable suture (number-2 Ethibond) using the tagged sutures, in sequence: piriformis, then obturator/gemelli, then quadratus - reconstructing posterior stability.
- Place a deep 19 Fr drain, then close gluteus maximus fascia, fascia lata, subcutaneous and skin in layers.
- Document a neurovascular check (sciatic nerve function) and an AP pelvis film to confirm reduction and hardware.
- Mobilise with physiotherapy when stable: toe-touch weight bearing with a frame or crutches.
- Start DVT prophylaxis (LMWH or DOAC); remove the drain when output is under 30 mL per 8 hours (usually 24-48 hours).
- Begin mandatory heterotopic ossification prophylaxis within 24 hours.
The sciatic nerve exits the greater sciatic notch below piriformis and runs 2-3 cm medial to the acetabular rim, just superficial to obturator internus. Identify it early, protect it with a vessel loop for the whole case, flex the hip and knee to reduce tension, limit continuous retraction to under 60 minutes, and avoid posterior screws aimed toward the notch. Injury occurs in 5-15 percent (mostly neuropraxia; 1-3 percent permanent).
The MFCA runs along the inferior hip capsule over obturator externus and is the primary blood supply to the femoral head. Limit anterior capsular dissection, preserve the quadratus femoris insertion, and handle the femoral head gently. Do not dissect onto obturator externus or divide the quadratus too proximally - either risks AVN.
Marginal impaction is cartilage-covered bone depressed at the fracture edge, present in 50 percent of posterior wall fractures. On CT look for the double-density sign at the posterior wall margin. If missed and not elevated and grafted, it leads to rapid post-traumatic arthritis even with an anatomic wall reduction.
Risk is 5-15 percent if not carefully assessed. Prevent it by checking fluoroscopy in multiple views (AP, obturator oblique, iliac oblique) AND directly palpating the articular surface through the capsulotomy before final tightening of every screw.
Flexing the hip and knee relaxes the sciatic nerve and improves visualisation. The ability to manipulate the leg during surgery is the key advantage of the lateral position for this approach.
The reconstruction plate functions as a buttress, not a compression device - it prevents posterior displacement of the wall. The lag screws provide interfragmentary compression across the fracture. Confusing the two is a classic viva error.
The short external rotators are dynamic stabilisers of the hip. Failing to repair them increases posterior instability and may worsen heterotopic ossification - repair them anatomically every time.
3.5 mm pelvic reconstruction plates and cortical screws (plus 4.5 mm screws for larger fragments), spring plates for comminution, and absorbable screws as an alternative for small fragments.
Pelvic reduction set, ball-spike pushers, pointed reduction clamps, 5 mm Schanz pins as joysticks, plate-bending irons, and bone-graft instruments.
C-arm fluoroscopy (essential), cell saver, surgical headlight, a radiolucent table, vessel loops for the sciatic nerve, and autograft or allograft for impaction defects.
Aftercare & Complications
Rehabilitation protocol | Phase | Timing | Weight bearing | Motion | |-------|--------|----------------|--------| | 1 | 0-6 weeks | Toe-touch | Gentle passive ROM; no active flexion over 90 degrees and no resisted external rotation for 6 weeks (protects the rotator repair) | | 2 | 6-8 weeks | Partial, if healing on XR | Active-assisted ROM | | 3 | 8-12 weeks | Progress to full | Full ROM and strengthening | | 4 | 3+ months | Full | Return to function - desk work around 6 weeks, heavy labour 3-6 months | Hip precautions for 6 weeks: avoid combined flexion, adduction and internal rotation; use an abduction pillow; avoid low chairs and crossing the legs. Follow-up: wound check at 2 weeks, XR (AP pelvis and Judet) at 6 and 12 weeks, review at 6 months and 1 year (looking for arthritis and AVN), then annual surveillance.
After the Kocher-Langenbeck approach, every patient gets prophylaxis: indomethacin 75 mg daily for 6 weeks (start within 24 hours) OR a single 7-8 Gy radiation dose within 72 hours. It cuts Brooker grade 3-4 heterotopic ossification from about 25 percent to 5-10 percent. Always mention prophylaxis whenever you discuss this approach in a viva.
Complications
- Recognition
- Foot drop, peroneal greater than tibial; compare with the pre-op baseline
- Prevention
- Identify early, vessel-loop, flex hip/knee, retraction under 60 min, avoid screws toward the notch
- Management
- Re-explore if a complete new deficit plus haematoma or screw concern; AFO, EMG at 6 weeks; tibialis posterior transfer if no recovery by 12-18 months
- Recognition
- Decreasing ROM at 4-8 weeks; periarticular calcification on XR at 3-6 weeks
- Prevention
- Indomethacin 75 mg daily for 6 weeks OR radiation 7-8 Gy within 72 hours; minimise soft-tissue trauma
- Management
- Brooker 1-2 observe; Brooker 3-4 excise after maturation at 12-18 months and restart prophylaxis
- Recognition
- Progressive pain and decreasing ROM; joint-space narrowing, osteophytes, sclerosis
- Prevention
- Anatomic reduction (under 1 mm ideal), remove all fragments, elevate marginal impaction
- Management
- Conservative first; injections; total hip arthroplasty for refractory disease
- Recognition
- Groin pain that may appear 6-24 months later; sclerosis then collapse on XR
- Prevention
- Emergency reduction under 6 hours, preserve the MFCA, limit anterior capsular dissection
- Management
- Pre-collapse (Ficat I-II): core decompression; post-collapse (III-IV): total hip arthroplasty
- Recognition
- Increasing pain; loss of reduction on follow-up XR; hardware migration
- Prevention
- Anatomic reduction, adequate lag compression, buttress plate with secure proximal and distal fixation
- Management
- Early: revision ORIF; late with acceptable alignment: accept and progress weight bearing
- Recognition
- Wound erythema, drainage, dehiscence; deep infection may present late
- Prevention
- Antibiotics within 60 minutes, meticulous technique, copious irrigation, drain placement
- Management
- Superficial: oral antibiotics; deep early: washout, retain hardware, IV antibiotics; deep late: hardware removal, spacer, delayed reconstruction
Viva & Exam Focus
WALLWALL - posterior wall assessment
PGOGQPGOGQ - short external rotators (superior to inferior)
- Course / risk
- Exits below piriformis, 2-3 cm medial to the acetabular rim; injury 5-15 percent
- Protection
- Identify early, vessel-loop, flex hip and knee, retraction under 60 min, avoid screws toward the notch
- Course / risk
- Exits the greater sciatic notch ABOVE piriformis; supplies gluteus medius/minimus and TFL; injury causes life-threatening haemorrhage and abductor denervation
- Protection
- No retraction above piriformis; stay inferior to the notch
- Course / risk
- Exits the notch below piriformis alongside the sciatic nerve; major bleeding risk
- Protection
- Careful dissection at the notch; identify before retracting; vascular clamps ready
- Course / risk
- Primary blood supply to the femoral head; runs along the inferior capsule over obturator externus
- Protection
- Limit anterior capsular dissection; preserve the quadratus femoris insertion; gentle femoral head manipulation
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man presents after a motor vehicle accident with a posterior hip dislocation. The hip has been reduced in ED. CT shows a posterior wall fracture involving approximately 35 percent of the wall with a small area of marginal impaction. How do you manage this patient?”
“During ORIF of a posterior wall fracture, you have difficulty achieving reduction. What are the potential causes and how would you address each?”
“Post-operatively, your patient with posterior wall ORIF develops a foot drop on day 1. How do you assess and manage this?”
Stability and the 40 percent rule
- Greater than 40 percent posterior wall = unstable = ORIF
- 20-40 percent: dynamic stress test under fluoroscopy decides
- Roof arc under 45 degrees on any view = unstable
- Subluxation on any image = unstable
Marginal impaction (50 percent)
- Cartilage-covered bone depressed at the fracture edge
- CT: double-density sign at the posterior wall margin
- Must be elevated and bone grafted
- Missed impaction = early arthritis despite anatomic wall reduction
Sciatic nerve protection
- Identify early at the greater sciatic notch below piriformis
- Protect with a vessel loop throughout the case
- Flex hip and knee to reduce nerve tension
- Limit continuous retraction to under 60 minutes
Critical numbers
- 5-15 percent sciatic palsy (1-3 percent permanent)
- 50 percent have marginal impaction
- 70 percent associated with posterior hip dislocation
- 20-30 percent HO without prophylaxis, 5-10 percent with
Post-operative protocol
- HO prophylaxis mandatory: indomethacin 75 mg for 6 weeks OR radiation
- Toe-touch weight bearing for 6 weeks, then progress on healing
- No active hip flexion over 90 degrees for 6 weeks
- Monitor for AVN - may appear 6-24 months postop
Background & Evidence
Epidemiology. The posterior wall is the most common elementary acetabular fracture pattern, accounting for about 25-30 percent of acetabular fractures. It classically follows a dashboard injury - the flexed knee strikes the dashboard, driving force up the femoral shaft into a flexed hip - and is associated with a posterior hip dislocation in about 70 percent. It predominates in young, active adults, and the same mechanism often produces associated knee (PCL), femoral-shaft and spine injuries that must be sought. Letournel classification. Acetabular fractures divide into elementary (single-column or single-wall) and associated (combined) patterns. The posterior wall is an elementary pattern - the one most often operated on.
- Patterns
- Posterior wall, posterior column, anterior wall, anterior column, transverse
- Note
- Posterior wall is the most common elementary pattern
- Patterns
- Both-column, T-shaped, posterior column plus wall, transverse plus posterior wall, anterior plus posterior hemitransverse
- Note
- More complex; demand tailored or combined approaches
Pathoanatomy of marginal impaction. At the moment of posterior dislocation the femoral head drives into the posterior wall, shearing off the wall fragment and impacting a segment of articular cartilage and subchondral bone at the fracture edge. This marginal impaction - hidden behind the wall fragment and visible on CT as a double-density sign - is present in about 50 percent. Unless it is elevated back flush and supported with graft, the femoral head rides on a depressed surface and post-traumatic arthritis follows rapidly, even when the wall itself looks well reduced. This is the single most important technical point of the operation and a favourite viva topic. The stability rule and its basis. The "under 20 percent stable, over 40 percent unstable, 20-40 percent grey zone" rule rests on two cadaveric serial-osteotomy models - Keith (1988) and Vailas (1989) - which independently showed that small fragments leave the hip stable, large fragments destabilise it, and the mid-range depends on capsular and soft-tissue integrity. That mid-range dependence on the soft tissues is exactly why a dynamic stress test under anaesthesia is the arbiter for borderline walls. The full studies are summarised in the References below.
References
Accuracy of reduction and clinical results of operative acetabular fracture treatment
- 259 patients, 262 displaced acetabular fractures fixed within 21 days; mean 6-year follow-up
- Anatomical reduction achieved in 185 hips (71 percent); rate fell with greater fracture complexity, older age and longer injury-to-surgery interval
- Overall clinical result excellent 40 percent, good 36 percent (76 percent good or excellent); outcome closely tracked the radiographic result
- Anatomical reduction and femoral-head/roof congruity were the key positive predictors of outcome
Stability of posterior fracture-dislocations of the hip: quantitative CT assessment
- Cadaveric study with serial posterior-wall osteotomies measured by CT in 16 hips
- Hips with under 20 percent of the posterior wall removed were all stable
- Hips with over 40 percent of the wall removed were all unstable
- The 20 to 40 percent transitional range is indeterminate and requires functional assessment
Posterior acetabular fracture-dislocations: fragment size, joint capsule and stability
- Cadaveric serial-osteotomy model evaluating fragment size and the posterior capsule
- Fragments involving 25 percent or less of the wall did not affect stability
- Fragments of 50 percent or more were consistently destabilising
- Stability of transitional 25 to 50 percent fragments was determined by the integrity of the posterior capsule
CT assessment of posterior-wall fractures after operative treatment
- 67 surgically treated posterior-wall fractures with postoperative 2D CT and mean 4-year follow-up
- CT detected residual displacement missed on plain films: offset over 2 mm in 11 hips and gaps of 2 mm or more in 52, despite 65 of 67 graded anatomical on radiographs
- Residual gap of 10 mm or more, total gap area of 35 mm squared or more, and femoral-head osteonecrosis predicted poor results
- Clinical outcome correlated strongly with CT-graded reduction accuracy
Displaced acetabular fractures: indications for operative and nonoperative management
- Review establishing that displaced acetabular fractures are operative unless strict non-operative criteria are met
- Non-operative criteria: congruent hip on AP and Judet views, an intact weight-bearing dome by roof-arc and subchondral-arc measurements, and a stable joint
- Decision must also weigh patient demand, physiology and surgeon/institutional experience
- Older, lower-demand patients are reasonable candidates for non-operative management when criteria are met
HO prophylaxis with indomethacin increases the risk of long-bone nonunion
- Randomised comparison within 282 acetabular ORIF patients of indomethacin versus radiation versus no prophylaxis
- Of 112 patients with a concomitant long-bone fracture, the indomethacin group had a 26 percent nonunion rate versus 7 percent in those not given indomethacin (p = 0.004)
- Radiation therapy provided HO prophylaxis without the nonunion penalty
- Risk is specific to associated long-bone fractures being healed concurrently
Further reading - Letournel E, Judet R (1993). Fractures of the Acetabulum, 2nd ed. Berlin: Springer-Verlag - the definitive classification and surgical-approach atlas (textbook reference, no PMID).
- Kreder HJ, Rozen N, Borkhoff CM, et al (2006). Determinants of functional outcome after simple and complex acetabular fractures involving the posterior wall. J Bone Joint Surg Br 88(6):776-82. PMID 16720773 - marginal impaction, comminution and residual displacement over 2 mm predict arthritis; consider primary THA in patients over 50 with marginal impaction and wall comminution.
- Brooker AF, Bowerman JW, Robinson RA, Riley LH (1973). Ectopic ossification following total hip replacement. J Bone Joint Surg Am 55(8):1629-32 - the Brooker HO grading system (classic reference).