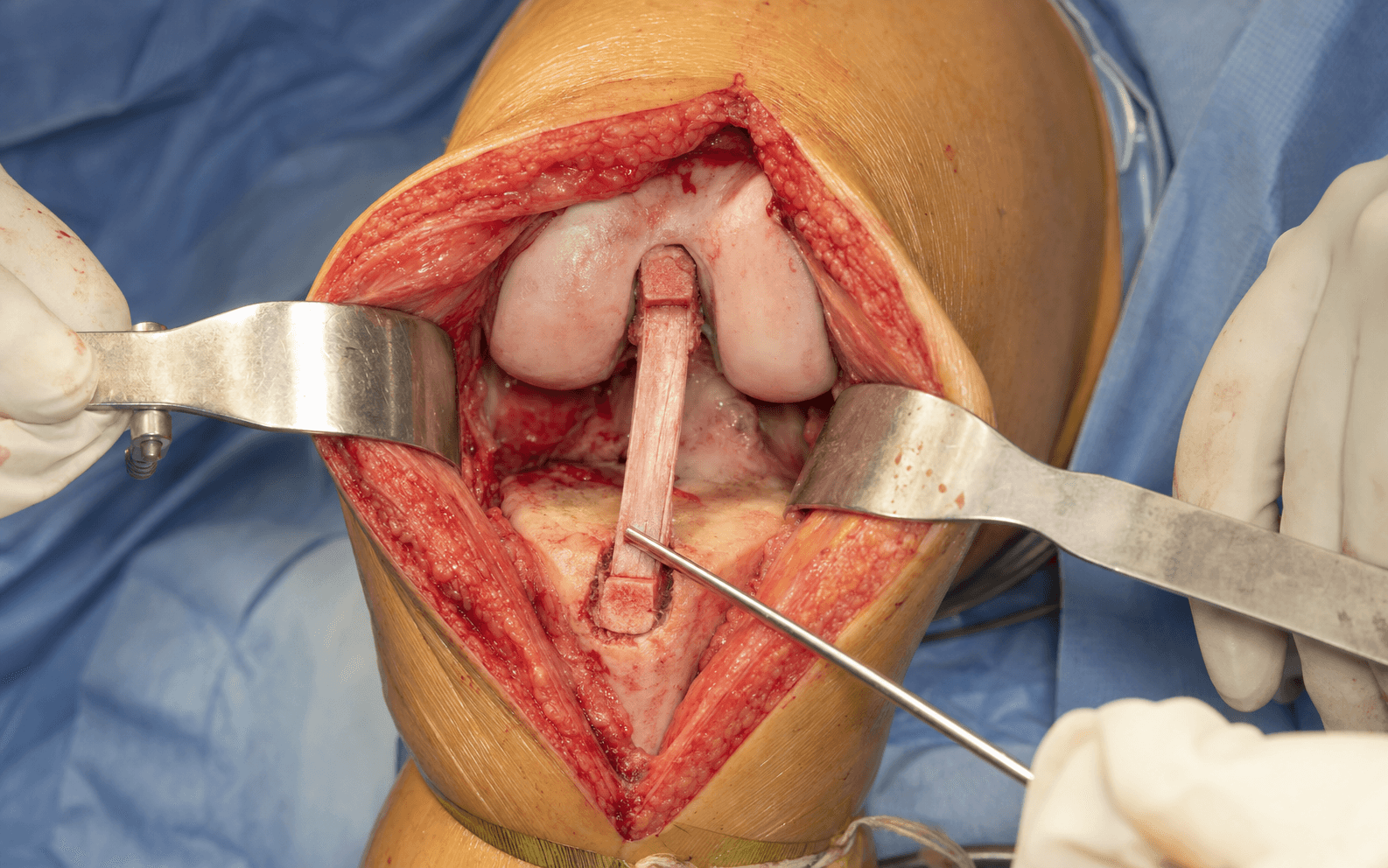
Arthroscopic reconstruction via anterolateral viewing and anteromedial working portals, with a central-third patellar-tendon bone-block graft · intermediate
- BTB autograft heals bone-to-bone in 6-8 weeks versus 12 weeks or more for soft-tissue grafts, and pairs with interference-screw fixation that has the highest pullout strength of any method (greater than 1000 N).
- Harvest the central third of the patellar tendon (10 mm width) and preserve a minimum of 5 mm of tendon laterally on each side (ideally 7-8 mm) - inadequate remnants raise patellar tendon rupture risk 5-10 fold from a baseline of 0.5-1 percent.
- The anatomic femoral tunnel is drilled through the anteromedial portal at 110-120 degrees of flexion, targeting the centre of the femoral footprint (10:30 right knee, 1:30 left knee); a minimum 2 mm posterior wall prevents blowout.
- The tibial tunnel (55 degrees) must run parallel to Blumensaat's line in full extension - too anterior causes roof impingement and a cyclops lesion, too posterior leaves a vertical graft and residual instability.
When & Why
Indication. ACL reconstruction is offered for symptomatic ACL deficiency - functional instability with a positive pivot shift, recurrent giving-way, or an associated repairable meniscal injury - particularly in young, active patients in whom non-operative management (physiotherapy, activity modification, bracing) has failed or is unlikely to restore stability. The bone-patellar tendon-bone (BTB) autograft is one of three standard graft choices and is selected for specific patients. Why BTB specifically. BTB is the historical gold standard with over 30 years of outcome data. Its defining advantage is bone-to-bone healing in 6-8 weeks (versus 12 weeks or more for soft-tissue grafts) combined with interference-screw fixation that has the highest pullout strength of any method (greater than 1000 N). It carries no concerns about inadequate graft diameter, and there is some evidence it may allow a return to sport 4-6 weeks earlier than hamstring, though this is debated. Its trade-off is donor-site morbidity: anterior knee pain in 20-30 percent (versus 10-15 percent for hamstring) and kneeling difficulty in 30-40 percent (often permanent), plus small risks of patella fracture and patellar tendon rupture. Patient-specific graft selection drives the choice - meta-analysis (Samuelsen, 47,613 patients) shows low rupture rates in both grafts (BTB 2.80 percent versus hamstring 2.84 percent, OR 0.83, p=0.01) with no significant difference in laxity or pivot shift, so the decision rests on morbidity profile and activity demands, not on one graft being "better":
High-demand collision athletes (rugby, AFL, NFL, hockey), military and law enforcement, revision ACL reconstruction (bone-to-bone healing advantage), multi-ligamentous injury needing strong fixation, patient preference for the gold standard, concurrent bony procedures (HTO, meniscal transplant).
Occupations requiring kneeling (carpet layers, plumbers, tilers), patients prioritising cosmesis (smaller incision), smaller or younger patients, pre-existing anterior knee pain or patellofemoral symptoms, patellar tendinopathy.
A compromise - larger graft diameter (9-11 mm), lower donor-site morbidity than BTB, bone-block option for faster healing than hamstring; increasingly used for revision and salvage.
Consent specifically for anterior knee pain (20-30 percent) and kneeling difficulty (30-40 percent, often permanent), universal infrapatellar-nerve numbness (anterolateral knee numbness, permanent and unavoidable), patella fracture (0.5-3 percent), patellar tendon rupture (0.5-1 percent), patella baja from scarring (3-5 percent), graft failure/re-rupture (5-10 percent at 5-10 years), arthrofibrosis and loss of extension (5-10 percent), and infection (0.5-1.5 percent). Setup. Supine with a leg holder or lateral thigh post allowing full range of motion. Tourniquet on the thigh (optional). Confirm full passive extension to 0 degrees and flexion greater than 120 degrees, hip flexed 30-45 degrees. The operation begins with a systematic examination under anaesthesia (Step 1).
The Operation
The goal: confirm the diagnosis under anaesthesia, expose the joint through standard arthroscopic portals and harvest the BTB graft through a midline incision, place anatomic femoral and tibial tunnels, pass and fix the bone-block graft with interference screws, and close the extensor mechanism meticulously. The exposure - the portals and the harvest incision - is laid out in Steps 1-3.
Operative sequence
- Systematic bilateral examination before prep and drape. Grade the Lachman (20-30 degrees flexion; anterior translation Grade 1 = 3-5 mm, Grade 2 = 5-10 mm, Grade 3 = greater than 10 mm), anterior drawer (90 degrees flexion) and pivot shift (Grade 0-3: glide, clunk, gross).
- Test varus/valgus stability at 0 degrees and 30 degrees to exclude collateral or posterolateral-corner injury; document full range of motion and compare with the contralateral side for medicolegal recording.
- A high-grade positive pivot shift confirms rotational instability and strongly supports reconstruction. Concurrent ligamentous injuries occur in 30-40 percent of cases.
- Establish the anterolateral viewing portal - a 5 mm stab 1 cm lateral to the patellar tendon at the joint line - and the anteromedial working portal at the medial border of the patellar tendon at the joint line, created under direct vision.
- Inflate the joint via a superolateral approach with 30-60 ml saline. Insert the 30-degree arthroscope and perform a systematic diagnostic sweep (see Step 5) before any tunnel work.
- A 6-8 cm vertical midline incision from the inferior pole of the patella to the tibial tubercle, centred over the patellar tendon (a small medial parapatellar incision is an alternative but a vertical midline incision is preferred - it preserves tendon remnants and reduces anterior knee pain).
- Incise the paratenon sharply in the midline and elevate it for later closure; this layer is critical for a gliding surface and vascularisation.
- Mark the central third of the patellar tendon (10 mm width) with a ruler and elevate the medial and lateral strips, preserving a minimum of 5 mm of tendon on each side (ideally 7-8 mm) for closure and to prevent rupture.
- Using an oscillating saw, cut the patellar bone plug (10 mm wide x 20-25 mm long x 7-8 mm deep) from the inferior pole and the tibial bone plug (10 mm wide x 20-25 mm long x 7-8 mm deep) from the tubercle; harvest the tendon sharply with a scalpel. Limit depth to less than 8 mm and width to 10 mm maximum to avoid patella fracture.
- Contour the bone plugs to a cylindrical shape matching the tunnel diameter (9-10 mm) with a rongeur or burr; chamfer the leading edges for smooth passage. Drill a 2.0-2.4 mm hole through the centre of each plug and pass a #5 Ethibond suture to aid passage and provide back-up fixation.
- Measure the final graft (total length 55-65 mm with bone plugs) and place it on a tensioning device, pretensioning at 20-30 pounds for a minimum of 10 minutes to eliminate creep. Keep the graft moist with saline-soaked gauze throughout.
- Systematic examination of every compartment: suprapatellar pouch, patellofemoral tracking, medial and lateral gutters, both menisci (posterior horn, body, anterior horn), the intercondylar notch, the ACL remnant and PCL, and all chondral surfaces.
- Associated injuries are common - meniscal tears 40-50 percent (medial more than lateral), chondral injuries 20-30 percent, MCL injury 30-40 percent. Repair meniscal pathology where possible, as meniscectomy worsens long-term outcomes.
- Debride the ACL remnant with a shaver and basket forceps, preserving the posterior fibres to protect the PCL. Clear synovium from the lateral wall and roof to expose the bony landmarks.
- Identify the lateral intercondylar ridge (resident's ridge) on the lateral wall, the bifurcate ridge between the AM and PL bundles, and the over-the-top position posteriorly. Notchplasty is not routine - perform a limited 2-3 mm removal only if true bony impingement in extension is demonstrated.
- Flex the knee to 110-120 degrees (critical) and drill through the anteromedial portal (the current gold standard, which reaches the true footprint that transtibial drilling cannot). Target the centre of the femoral footprint - 1-2 mm anterior to the over-the-top position, at the resident's ridge, clock position 10:30 (right knee) or 1:30 (left knee).
- Place a 2.4 mm guidewire, check arthroscopically from the anterolateral portal, then overdrill with a cannulated reamer to 10 mm to a depth of 25-30 mm. Confirm a minimum 2 mm posterior wall with a depth gauge before proceeding - blowout causes fixation failure.
- Set the tibial ACL guide at 55 degrees to the tibial shaft. The intra-articular target is the centre of the tibial footprint - just anterior to the anterior horn of the lateral meniscus, just anterior to the tibial spine, lateral to the medial tibial spine. The extra-articular start point is 3-4 cm distal to the joint line and 2-3 cm medial to the tibial tubercle (within the harvest site).
- Drill a 2.4 mm guidewire under arthroscopic vision and overdrill to 10 mm. Most critical check: in full extension the tunnel must be parallel to Blumensaat's line - too anterior causes roof impingement and a cyclops lesion; too posterior leaves a vertical graft and instability.
- Pass a suture retrograde through the tibial tunnel, across the joint and out the femoral tunnel; secure it to the femoral bone-plug sutures and pull the plug into the femoral tunnel from the cortical side until it sits flush at the aperture.
- Then pass the suture to the tibial plug and draw it through the tibial tunnel until it seats at the tibial aperture. Confirm arthroscopically that both plugs are fully seated, the tendon portion is not twisted, and there is no soft-tissue interposition.
- With the femoral plug seated, insert an interference screw (7-9 mm diameter, 20-25 mm length) parallel to the bone plug between the plug and the tunnel wall, using a hand driver until flush or slightly countersunk. Test fixation by pulling on the tibial sutures - it should be rock solid.
- Bioabsorbable screws are preferred (no MRI artefact, no hardware removal); metal screws are an alternative for revision or high-demand cases. Back-up cortical-button or cross-pin fixation is used in soft bone or for small plugs.
- Before tibial fixation, cycle the graft 20-30 times through full range of motion (full extension to greater than 120 degrees flexion) while maintaining moderate tension (20-30 N) to eliminate creep.
- Position the knee at 20-30 degrees flexion (not full extension), apply an anterior-drawer force on the proximal tibia, and tension the tibial sutures until the graft feels firm but not over-constrained; hold this tension during tibial fixation.
- Maintaining tension at 20-30 degrees flexion, insert the tibial interference screw (7-9 mm diameter, 20-25 mm length) parallel to the tibial bone plug, between the plug and the anterior tunnel wall, until flush or slightly below the bone surface.
- Release the tension and cycle the knee through full range of motion, checking for crepitus, catching or loss of motion.
- Systematic checks: (1) range of motion - must achieve full passive extension (0 degrees) and flexion greater than 120 degrees; (2) impingement test - in full extension the graft must not contact the roof or PCL; (3) stability - Lachman and pivot shift under direct vision should be negative; (4) graft tension firm, not lax; (5) no cyclops tissue anterior to the graft; (6) haemostasis.
- Close the harvest site meticulously in layers: repair the paratenon and lateral tendon remnants side-to-side with interrupted 2-0 or #1 Vicryl (the critical layer), then subcutaneous 3-0 Vicryl and a running subcuticular 3-0 Monocryl or staples. Do not use a drain (it increases infection without benefit).
- Irrigate the joint with 3-4 L saline, infiltrate 20-30 ml of 0.25 percent marcaine with 1:200,000 epinephrine, close each portal with a single nylon suture, and apply a compression dressing with cryotherapy. Brace locked in full extension.
Preserve a minimum of 5 mm of patellar tendon laterally on each side (ideally 7-8 mm). Inadequate remnants (less than 5 mm) raise the risk of patellar tendon rupture 5-10 fold from a baseline of 0.5-1 percent. Measure the central third (10 mm maximum) precisely with a ruler before cutting, use an oscillating saw (not an osteotome) to limit depth to less than 8 mm, and close the paratenon meticulously. Avoid re-harvesting the same tendon in staged ipsilateral procedures.
Before reaming the femoral tunnel, confirm a minimum 2 mm posterior wall with a depth gauge. A blowout (tunnel too posterior, shallow, or over-reamed) causes complete fixation failure. If discovered intra-operatively, switch to an outside-in or two-incision technique with suspensory (cortical-button) back-up fixation, as the interference screw will have no posterior wall to compress against.
In full extension the tibial tunnel must run parallel to Blumensaat's line (the roof of the intercondylar notch). Too anterior causes roof impingement, extension loss and a cyclops lesion; too posterior leaves a vertical graft with poor rotational control. Check it arthroscopically before leaving the joint.
Tension and fix the graft at 20-30 degrees of flexion with an anterior-drawer force. Full extension over-constrains the knee (patellofemoral pain, flexion contracture); flexion greater than 30 degrees under-tensions it (residual laxity). Cycle the graft 20-30 times first to remove creep, which otherwise causes 2-3 mm of early post-operative laxity.
Aftercare & Complications
Rehabilitation follows an accelerated, evidence-based protocol - immediate weight-bearing and early range of motion are safe with solid BTB fixation and give faster recovery with no increase in laxity (Beynnon RCT). | Phase | Timing | Immobilisation / loading | Therapy | |-------|--------|--------------------------|---------| | 1 | 0-2 weeks | Brace locked in extension for ambulation; weight-bearing as tolerated with crutches | Quad sets, ankle pumps, heel slides; goal full passive extension 0 degrees by 2 weeks | | 2 | 2-6 weeks | Wean brace (discard by 4 weeks) and crutches (by 2-3 weeks) | Range of motion to 0-120 degrees; closed-chain (leg press, squats, step-ups); cycling, swimming | | 3 | 6-12 weeks | Full range of motion | Progressive resistance, proprioception, gait normalisation; pool running, elliptical | | 4 | 3-6 months | Running progression | Agility and cutting drills, sport-specific training, plyometrics | | 5 | 6-9 months | Return-to-sport testing | Hop tests greater than 90 percent limb symmetry index; isokinetic strength greater than 90 percent; ACL-RSI psychological readiness | Return to sport. Typical return is 6-9 months when criteria are met (potentially 4-6 weeks earlier than hamstring due to faster bone healing, though a minimum of 9 months is strongly recommended regardless of graft). Pooled meta-analysis (Ardern, 7,556 patients): 81 percent return to any sport, 65 percent to pre-injury level, only 55 percent to competitive sport - so clearance should be criteria-based, not date-based, with re-injury risk highest in young athletes returning early. Complications
- Recognition
- Pain with kneeling, stairs, sitting; peak at 3-6 months; tenderness over harvest site; Insall-Salvati ratio less than 0.8 indicates baja
- Prevention
- Vertical midline incision, meticulous paratenon closure, preserve 5 mm remnants, early patellar mobilisation, aggressive quad rehab, pre-operative counselling
- Management
- NSAIDs, activity modification, quad strengthening, patellar mobilisation; 50 percent improve by 2 years; injection or neuroma excision rarely effective
- Recognition
- Acute re-injury with pop and swelling (80 percent), or gradual instability; positive Lachman and pivot shift; side-to-side difference greater than 5 mm
- Prevention
- Anatomic tunnel placement (most critical), adequate tensioning and fixation, delayed return to sport (minimum 9 months), neuromuscular training
- Management
- Revision ACL reconstruction (BTB or allograft); staged bone grafting for malpositioned or widened tunnels (greater than 12 mm); revision success 80-85 percent versus 90-95 percent primary
- Recognition
- Inability to achieve full passive extension (greater than 5 degrees loss); firm endpoint; develops first 3-6 months; cyclops lesion on MRI
- Prevention
- Early surgery once inflammation settles, anatomic tibial tunnel parallel to Blumensaat's line, aggressive early extension (0 degrees by 2 weeks), avoid over-constraint
- Management
- Early (less than 6 weeks): aggressive physio; 6-12 weeks: manipulation under anaesthesia; greater than 12 weeks or cyclops: arthroscopic debridement and lysis of adhesions
- Recognition
- Pain with direct kneeling pressure; tenderness and thickening over harvest site; infrapatellar numbness; symptoms permanent after 2 years
- Prevention
- Patient selection (avoid BTB for kneeling occupations - choose hamstring), precise harvest, meticulous closure, pre-operative counselling about likely permanence
- Management
- Activity modification, knee pads, occupational change in 5-10 percent; surgical debridement rarely effective; adaptation is key
- Recognition
- 0.5 percent intra-operative, 2.5 percent post-operative from trauma; pain, swelling, inability to straight-leg-raise; inferior-pole fracture on X-ray
- Prevention
- Limit bone plug to 10 mm width and less than 8 mm depth, oscillating saw with depth guide, patient education about post-op trauma risk
- Management
- Non-displaced: brace in extension 6 weeks; displaced greater than 2 mm or comminuted: ORIF (tension band or screws); severe salvage may need patellectomy
- Recognition
- Sudden pain, inability to extend, palpable defect, high-riding patella; straight-leg-raise impossible; confirmed on ultrasound or MRI
- Prevention
- Preserve minimum 5 mm remnants bilaterally (ideally 7-8 mm), measure with ruler, meticulous paratenon closure, avoid re-harvesting the same tendon
- Management
- Urgent repair within 2 weeks with heavy non-absorbable sutures, cerclage or allograft augmentation if poor tissue; brace 6 weeks, protected range of motion 6-12 weeks
- Recognition
- Limited flexion, anterior pain with stairs; Insall-Salvati ratio less than 0.8; develops over 3-12 months
- Prevention
- Early patellar mobilisation from week 1, aggressive range of motion, meticulous closure, monitor patella height if stiffness develops
- Management
- Aggressive physio and patellar mobilisation; moderate-severe: surgical release of infrapatellar contracture; severe refractory: tibial tubercle distalisation osteotomy
- Recognition
- Loss of terminal extension (5-15 degrees), firm endpoint, clunk; develops 2-6 months; focal anterior soft-tissue mass on MRI
- Prevention
- Anatomic tibial tunnel parallel to Blumensaat's line, avoid excessive remnant retention, aggressive early extension
- Management
- Arthroscopic excision of the fibrotic nodule, ensure full extension intra-operatively, immediate aggressive post-op range of motion
- Recognition
- Wound erythema, drainage, fever; deep septic arthritis with effusion and inability to weight-bear; aspiration greater than 50,000 white cells diagnostic
- Prevention
- Prophylactic cephalosporin within 60 minutes, chlorhexidine prep, minimise traffic, copious irrigation, avoid drains
- Management
- Superficial: oral antibiotics; deep less than 3 weeks: arthroscopic washout, IV antibiotics, attempt graft retention; greater than 3 weeks or septic loosening: open washout, consider graft removal
- Recognition
- Infrapatellar numbness universal and permanent; foot drop (common peroneal), absent pulses (popliteal), calf swelling (DVT or compartment)
- Prevention
- Careful portal placement, visualise guidewires, avoid over-length posterior screws, do not place retractors blindly posteriorly, monitor perfusion
- Management
- Infrapatellar numbness: counsel pre-operatively; arterial injury: immediate vascular repair; peroneal neuropraxia: observe and splint; compartment syndrome: emergency fasciotomy
Viva & Exam Focus
HARVESTHARVEST - BTB graft procurement checklist
TUNNELTUNNEL - anatomic tunnel-positioning principles
- At risk
- Crosses medially 1-2 cm below the inferior pole in subcutaneous tissue; universal injury causes permanent anterolateral numbness
- How to protect
- Use a vertical midline incision (not medial parapatellar, which transects it); accept and counsel about the unavoidable numbness
- At risk
- Anastomotic ring from the superior and inferior geniculate arteries in the periosteum; excessive stripping risks patellar AVN
- How to protect
- Minimise periosteal stripping during plug harvest, use a saw for precise cuts, maintain paratenon cover
- At risk
- Remaining medial and lateral strips after central-third harvest; remnants less than 5 mm raise rupture risk 5-10 fold
- How to protect
- Measure and mark the 10 mm central third precisely with a ruler; preserve 5 mm minimum (ideally 7-8 mm) each side
- At risk
- Secondary ossification centre fusing at 15-17 years in males, 13-15 in females; avulsion risk in adolescents
- How to protect
- Palpate and visualise the apophyseal line; harvest the tibial plug proximal to the apophysis, avoiding the cartilaginous junction
- At risk
- Lies immediately posterior to the ACL footprint; at risk in notch debridement and posterior tibial malposition
- How to protect
- Stay anterior during debridement, preserve posterior ACL-remnant fibres as a barrier, avoid a tibial tunnel more than 7 mm posterior to the anterior spine
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Compare BTB and hamstring autograft - advantages and disadvantages of each, and how do you choose?”
“What are the specific complications of BTB graft harvest and how do you prevent them?”
“Describe your technique for anatomic femoral tunnel placement in BTB ACL reconstruction and why it is critical.”
Indication & graft choice
- ACL deficiency with instability or repairable meniscal injury failing non-operative care
- BTB for collision athletes, military, revision, multi-ligament injury, patient preference
- Hamstring for kneeling occupations, cosmesis, smaller patients, pre-existing anterior knee pain
- Equivalent failure and stability in meta-analyses - choice is patient-specific
Exposure
- Arthroscopic: anterolateral viewing + anteromedial working portals
- BTB harvest: 6-8 cm vertical midline incision, patella to tibial tubercle
- At risk: infrapatellar nerve (universal numbness), patellar blood supply, tendon remnants, PCL
Critical steps
- Harvest 10 mm central third, 5 mm remnants minimum, plugs 10 x 20-25 mm, depth less than 8 mm
- Femoral tunnel trans-AM portal at 110-120 degrees, 10:30 or 1:30 footprint, minimum 2 mm posterior wall
- Tibial tunnel at 55 degrees, parallel to Blumensaat's line in full extension
- Interference screws 7-9 mm; cycle 20-30 times; tension and fix at 20-30 degrees flexion
Finish
- Achieve full passive extension 0 degrees and flexion greater than 120 degrees before closing
- Negative Lachman and pivot shift under vision, no roof impingement
- Meticulous layered closure (paratenon critical), no drain, brace locked in extension
Donor-site morbidity
- Anterior knee pain 20-30 percent, kneeling 30-40 percent (often permanent)
- Patella fracture 0.5-3 percent, tendon rupture 0.5-1 percent (5-10 fold higher if remnants less than 5 mm)
- Patella baja 3-5 percent, infrapatellar numbness universal and unavoidable
- Counsel pre-operatively - this profile drives graft selection
Outcomes
- Graft survival 90-93 percent at 5 years, 85-90 percent at 10 years
- Return to sport: 81 percent any, 65 percent pre-injury, 55 percent competitive (Ardern)
- Failure highest under 18 years (15-20 percent); criteria-based return, minimum 9 months
- Registry data (Gifstad 45,998): hazard ratio 0.63 favouring BTB for revision
Background & Evidence
Epidemiology. ACL injury and reconstruction are common, with reconstruction incidence and graft-choice trends documented in large population data (Mall, 2014). Risk factors for re-injury and failure include young age (under 18 years highest, 15-20 percent failure), return to pivoting sports, non-anatomic tunnel position and female sex. Surgical anatomy. The patellar tendon is 40-50 mm long, 25-35 mm wide and 4-6 mm thick (cross-sectional area 100-150 mm squared), with a central-third tensile strength of 2200-2600 N (entire tendon 2900-3500 N); it is predominantly type I collagen (70-80 percent dry weight). Its blood supply is the extraosseous anastomotic ring from the superior and inferior geniculate arteries, and the cruciates are supplied by the middle geniculate. The femoral ACL footprint lies on the lateral wall of the medial femoral condyle (18-22 mm anteroposterior, 8-12 mm superoinferior), centred at 10:30 (right) or 1:30 (left), bounded anteriorly by the resident's ridge and subdivided by the bifurcate ridge into an anteromedial bundle (8-10 mm) and a posterolateral bundle (6-8 mm). The tibial footprint (14-18 mm anteroposterior, 10-14 mm mediolateral) lies just anterior to the tibial spine and the anterior horn of the lateral meniscus. The intercondylar notch has a normal notch-width index of 0.25-0.30; an index less than 0.20 is a stenotic notch with a historical (controversial) association with ACL injury. Tunnel-drilling techniques. Femoral tunnel position is the single most important technical factor. The four approaches differ in whether they reach the true anatomic footprint:
- Position achieved
- Through the tibial tunnel at 90 degrees; high, anterior, vertical (~11:00 or 1:00)
- Pros
- Single portal, simple, short learning curve
- Cons and status
- Non-anatomic; vertical graft with poor rotational control; higher failure (10-15 percent); largely abandoned
- Position achieved
- Independent drilling at 110-120 degrees flexion; anatomic 10:30 or 1:30 footprint
- Pros
- Anatomic position, horizontal graft, superior pivot-shift control, lower failure (5-8 percent)
- Cons and status
- Technically demanding; needs hyperflexion; risk of posterior-wall blowout if incorrect
- Position achieved
- From the lateral femoral cortex to the footprint, retrograde
- Pros
- Excellent intra-articular control, anatomic, no posterior-wall blowout
- Cons and status
- Technically demanding; ITB or vastus lateralis injury; awkward tunnel-graft angle; two incisions
- Position achieved
- Retrograde socket with suspensory cortical fixation
- Pros
- Preserves lateral cortex for revision; very anatomic; no cortical breach
- Cons and status
- Loses the bone-to-bone healing advantage of BTB (better for soft-tissue grafts); more expensive
Fixation. Interference-screw fixation (7-9 mm diameter, 20-25 mm length) is preferred for BTB on both sides, giving the highest pullout strength (greater than 1000 N). Bioabsorbable screws (PLLA/PLGA) avoid MRI artefact and need no removal (cyst formation 5-10 percent, usually asymptomatic); biocomposite screws (PLLA plus hydroxyapatite) reduce tunnel widening; metal (titanium) screws are used for revision or high-demand cases. Back-up fixation (cortical button femorally, post-and-washer tibially) is reserved for osteoporotic bone, small plugs (less than 20 mm), widened revision tunnels, or a belt-and-suspenders approach. Graft-selection evidence. Meta-analysis (Samuelsen, 47,613 patients) found rupture 2.80 percent BTB versus 2.84 percent hamstring (OR 0.83, p=0.01) - a small absolute difference - with no significant difference in laxity, pivot shift or Lachman. The Cochrane review (Mohtadi, 19 RCTs) found no significant difference in re-rupture, hop, Tegner, Lysholm or IKDC scores, though static stability tests favoured BTB while BTB carried more anterior-knee and kneeling symptoms. Pooled Scandinavian registries (Gifstad, 45,998 reconstructions) reported a revision hazard rate ratio of 0.63 favouring BTB, consistent across subgroups and more pronounced in pivoting sports - the same direction seen in the AOANJRR and other national registries. Differences are small and patient-specific factors remain more important. Outcomes. Graft survival is approximately 95-97 percent at 2 years, 90-93 percent at 5 years, 85-90 percent at 10 years and 80-85 percent at 15 years, with most revisions (60-70 percent) occurring within the first 5 years. Radiographic osteoarthritis develops in 20-30 percent at 10 years and 40-60 percent at 15-20 years (meniscectomy is the strongest predictor, at 3-4 times the risk), with symptomatic OA in 10-15 percent at 10 years. Patient-reported outcomes stabilise around an IKDC of 85-92 and a Lysholm of 88-94, with 75-85 percent satisfied at 10 years.
References
Hamstring versus Patellar Tendon Autograft for ACL Reconstruction: Is There a Difference in Graft Failure Rate? A Meta-analysis of 47,613 Patients
- Pooled 47,613 reconstructions (39,768 BTB, 7,845 hamstring) from 14 RCTs, 10 prospective cohorts and one national registry; mean age 28 years, mean follow-up 68 months
- Rupture rate 2.80 percent BTB versus 2.84 percent hamstring - low in both; odds ratio 0.83 (95 percent CI 0.72-0.96, p=0.01) favouring BTB, but number needed to treat to prevent one rupture was 235
- No significant difference in residual laxity (KT, p=0.16), pivot shift (p=0.51) or Lachman (p=0.84) between graft types
Patellar Tendon versus Hamstring Tendon Autograft for Anterior Cruciate Ligament Rupture in Adults (Cochrane Review)
- Nineteen randomised or quasi-randomised trials, 1,597 young to middle-aged adults with minimum 2-year follow-up
- No significant difference in re-rupture, single-leg hop, Tegner, Lysholm or IKDC scores between BTB and hamstring
- Static stability tests (instrumented, Lachman, pivot shift) consistently favoured BTB; BTB had more anterior knee problems (notably kneeling) and a small loss of extension, while hamstring showed a trend to flexion-strength loss
Lower Risk of Revision with Patellar Tendon Autografts Compared with Hamstring Autografts: A Registry Study Based on 45,998 Primary ACL Reconstructions in Scandinavia
- Pooled Norwegian, Swedish and Danish ACL registries: 45,998 primary reconstructions (6,736 BTB, 38,666 hamstring), median follow-up 3 years
- Risk of revision significantly lower with BTB - hazard rate ratio 0.63 (95 percent CI 0.53-0.74) versus hamstring
- Effect consistent across sex, age and cartilage-injury subgroups, and slightly more pronounced for pivoting sports (soccer, handball, alpine)
Nonanatomic Tunnel Position in Traditional Transtibial Single-Bundle ACL Reconstruction Evaluated by Three-Dimensional Computed Tomography
- 3D CT of 32 transtibial single-bundle reconstructions compared with reference anatomic insertion data
- Femoral tunnels were positioned significantly anterior to both the anteromedial and posterolateral anatomic footprints (p less than 0.001), and tibial tunnels medial to the anatomic posterolateral position (p less than 0.001)
- Transtibial drilling failed to place tunnels within the native ACL insertion site
Fifty-Five Per Cent Return to Competitive Sport Following ACL Reconstruction Surgery: An Updated Systematic Review and Meta-analysis
- Sixty-nine studies, 7,556 participants pooled by random-effects meta-analysis
- 81 percent returned to any sport, 65 percent to pre-injury level, but only 55 percent to competitive sport after reconstruction
- Hamstring autograft favoured return to competitive sport (OR 2.4) and BTB favoured return to pre-injury level (OR 1.2); younger age, male sex, elite status and a positive psychological response also predicted return
Anterior Cruciate Ligament Replacement: Comparison of Bone-Patellar Tendon-Bone Grafts with Two-Strand Hamstring Grafts - A Prospective, Randomized Study
Prospective RCT comparing BTB and two-strand hamstring grafts, informing the trade-off between static stability and donor-site morbidity. The same group's accelerated-versus-conservative rehabilitation RCT (Am J Sports Med, 2005) showed accelerated weight-bearing and early range of motion were safe with no increase in laxity.
Rehabilitation After Anterior Cruciate Ligament Reconstruction: A Systematic Review
Systematic review supporting immediate weight-bearing and early closed-chain rehabilitation after reconstruction, and showing that delaying return to sport reduces re-injury risk.
Incidence and Trends of Anterior Cruciate Ligament Reconstruction in the United States
Epidemiological data on ACL reconstruction incidence and graft-choice trends in a large population, underpinning the epidemiology of graft selection.