Anatomic single-bundle ACL reconstruction using central quadriceps tendon autograft | advanced
- Quadriceps tendon graft offers a robust cross-sectional area (greater than 90 mm2 in most adults) with lower donor-site morbidity and anterior knee pain than bone-patellar-tendon-bone; it is particularly advantageous in revision settings and in patients with patellar tendon pathology or high-demand athletes who kneel frequently.
- The central third of the quadriceps tendon (typically 8-10 mm wide, 60-80 mm long) can be harvested with or without a patellar bone block; when a bone block is taken it is usually 15-20 mm long by 8-10 mm wide and provides aperture fixation options on the tibial side.
- Anatomic femoral tunnel placement is achieved via the anteromedial portal with the knee in 120-130 degrees of flexion; the femoral footprint centre lies at the intersection of the lateral intercondylar ridge and the bifurcate ridge, approximately 6-8 mm anterior to the posterior wall and 2-3 mm proximal to the inferior articular margin.
- Graft tensioning is performed at 20-30 degrees of flexion with 80-100 N of force after tibial fixation; the knee is cycled through full range of motion to confirm absence of impingement against the notch roof or PCL before final tibial fixation.
When & Why
Indication. Symptomatic ACL insufficiency with documented instability on pivot-shift or Lachman testing — acute or chronic, having failed non-operative management with recurrent giving-way during pivoting or cutting, or with a concomitant repairable meniscal tear or chondral injury that needs a stable knee to succeed. High-demand athletes and occupational groups needing rotational stability (military, police, firefighter) are also offered reconstruction. Absolute indications
- Acute or chronic ACL insufficiency with documented instability on pivot-shift or Lachman testing
- Failed non-operative management with recurrent giving-way during pivoting or cutting activities
- Concomitant repairable meniscal tear or chondral injury requiring stabilisation for a successful outcome
- High-demand athlete or occupational requirement for rotational stability Relative indications
- Revision ACL reconstruction when hamstring or patellar tendon grafts were previously used or are unavailable
- Skeletally immature patients with significant growth remaining (quadriceps tendon avoids the physeal violation concerns associated with bone blocks)
- Patients with patellar tendinopathy, previous patellar tendon harvest, or anterior knee pain that bone-patellar-tendon-bone would exacerbate
- Large patients (greater than 100 kg) or those with a wide intercondylar notch requiring a robust graft cross-section The graft-choice decision. The quadriceps tendon is preferred in revision, skeletally immature and patellar-tendon-pathology settings, and in high-demand athletes who kneel — the graft chosen shapes donor morbidity far more than it shapes long-term stability.
Robust cross-section (greater than 90 mm2), tensile strength exceeding 2000 N, and anterior knee pain in only 5-15 percent versus 20-40 percent for patellar tendon. Harvest with or without a patellar bone block. Ideal for revision, the skeletally immature, patellar tendon pathology, and kneeling athletes.
Cross-section 35-50 mm2 with no bone block and a popular primary choice. Slightly higher reported failure rates in high-level pivoting athletes and possible persistent hamstring weakness affecting sprinting and cutting.
Cross-section 45-60 mm2 with bone blocks allowing aperture fixation and rapid incorporation, but the highest donor morbidity and anterior knee pain (20-40 percent); kneeling is uncomfortable.
Contraindications. Absolute: active knee infection or septic arthritis; severe osteoarthritis with joint-space narrowing greater than 50 percent or Kellgren-Lawrence grade 4 changes; fixed varus or valgus malalignment greater than 10 degrees requiring osteotomy first. Relative: poor quadriceps strength or neuromuscular control (optimise with prehabilitation); inability to comply with the rehabilitation protocol; a low-demand patient with minimal functional instability manageable with bracing and activity modification. Consent specifically for anterior knee discomfort, harvest-site quadriceps weakness (5-10 percent still present at 6 months), patellar fracture if a bone block is taken (0.5-1.5 percent), residual laxity or graft failure (2-6 percent primary), stiffness and cyclops lesion, infection (less than 1 percent), and the 9-12 month return-to-sport timeline with criteria-based clearance. Setup. Supine on a radiolucent table with 0-130 degrees of knee flexion achievable; a lateral post or leg holder allows valgus stress for the medial compartment. General or spinal anaesthesia with a single-shot adductor canal block (preferred over a femoral block to preserve quadriceps motor function for early mobilisation). Examine under anaesthesia — confirm Lachman and pivot-shift grade, side-to-side difference with KT-1000 or Rolimeter, and any meniscal or collateral pathology, comparing with the contralateral knee. Equipment: 30-degree and 70-degree arthroscopes, an ACL guide system with offset femoral aimer, 4.5 mm and 7-10 mm cannulated reamers, a suspensory fixation device (Endobutton, TightRope or similar), interference screws (7-9 mm), and an oscillating saw or osteotome for the bone block.
The Operation
The goal is an anatomic single-bundle reconstruction: harvest a robust central quadriceps tendon graft, recreate the femoral and tibial footprints through independent anatomic tunnels, tension and fix the graft without impingement, and restore rotational stability. The exposure is the graft-harvest incision above the patella and the standard arthroscopy portals — both are laid out as the opening steps below.
Operative sequence
- Supine, radiolucent table, proximal-thigh tourniquet (inflate only if needed for visualisation); confirm instability under anaesthesia.
- Establish anterolateral and anteromedial portals; perform a complete diagnostic arthroscopy and address meniscal and chondral pathology first.
- Debride the residual ACL stump from the tibial footprint; perform notchplasty (remove 2-4 mm from the roof and lateral wall with an arthroscopic burr) if the intercondylar notch width is less than 12 mm or osteophytes are present.
- Make a 3-4 cm longitudinal midline incision centred 2-3 cm proximal to the superior pole of the patella.
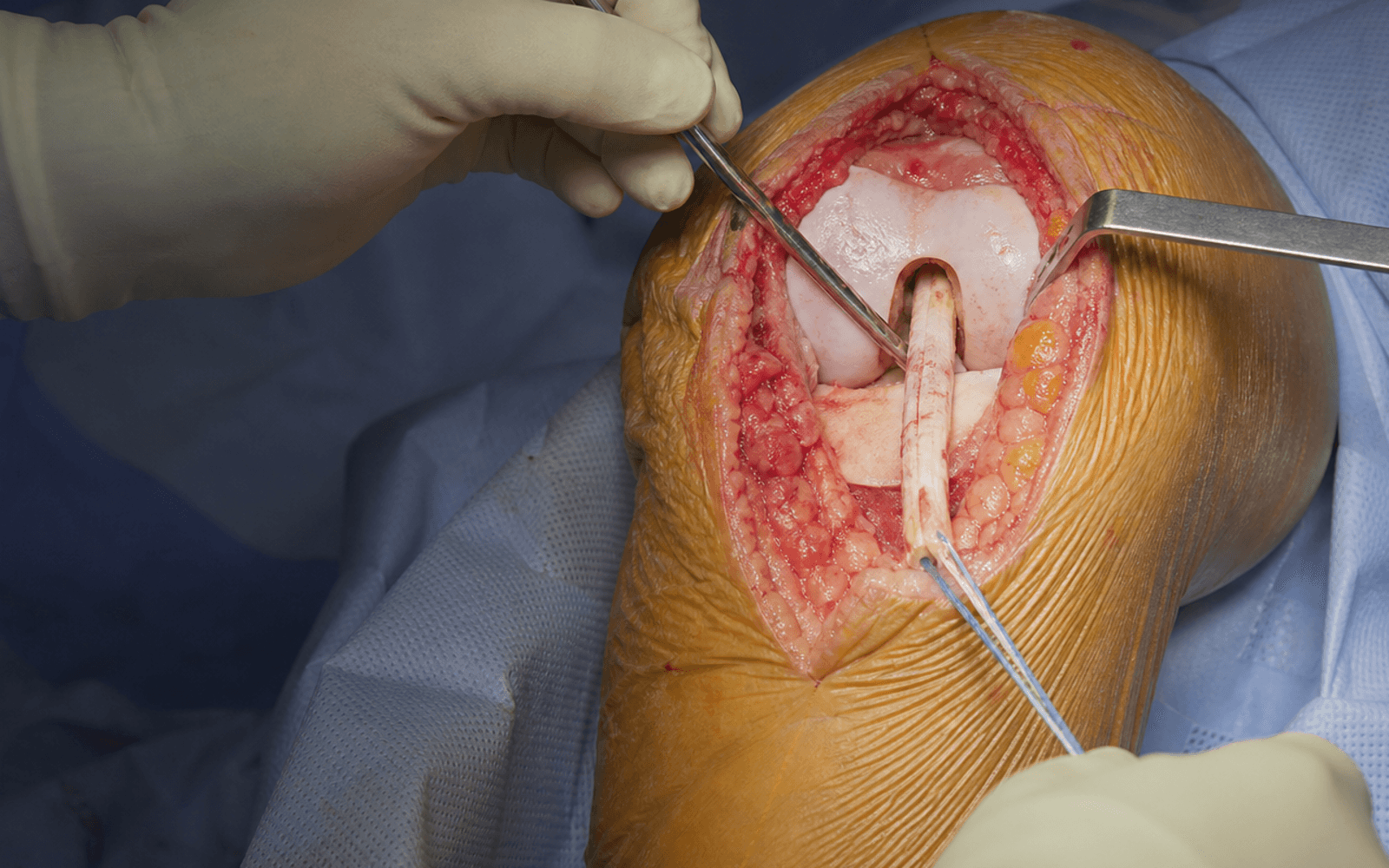
- Incise skin and subcutaneous tissue; identify and split the paratenon longitudinally, then incise the rectus femoris fascia in the midline to expose the quadriceps tendon (a trilaminar structure — superficial rectus femoris, middle vastus lateralis and medialis, deep vastus intermedius).
- Mark a central 8-10 mm wide strip; using a number 15 blade or tendon stripper, harvest a full-thickness central-third graft 60-80 mm long, leaving at least 5 mm of tendon on each side.
- For a bone block, use an oscillating saw with a depth stop to create a 15-20 mm long by 8-10 mm wide by 8 mm deep trapezoidal osteotomy of the superior patella, keeping the cut within the central 15 mm to avoid fracture.
- Elevate the graft off the vastus intermedius and deliver it; close the harvest defect in layers (rectus fascia, paratenon) before proceeding to limit fluid extravasation.
- Whip-stitch both soft-tissue ends with non-absorbable suture (FiberWire or similar); if a bone block is present, trim it to 8-10 mm diameter for interference-screw fixation.
- Measure graft diameter at both ends and select suspensory button or interference screw accordingly; store the graft in saline-soaked gauze until passage.
- Through the anteromedial portal with the knee flexed 120-130 degrees, identify the lateral intercondylar ridge (resident's ridge) on the medial wall of the lateral femoral condyle.
- Place the guide pin at the anatomic footprint centre — 6-8 mm anterior to the posterior wall and immediately distal to the ridge (intersection with the bifurcate ridge).
- Ream a 4.5 mm pilot tunnel, then over-ream with a cannulated reamer matched to graft diameter plus 0.5 mm; aim for greater than 20 mm intraosseous length and plan suspensory fixation if the tunnel is short.
- With the tibial guide through the anteromedial portal and the knee at 90 degrees, place the guide tip at the centre of the tibial footprint — 7-10 mm anterior to the PCL and 1-2 mm posterior to the anterior horn of the lateral meniscus.
- Drill the guide pin, confirm position arthroscopically or fluoroscopically, over-ream to graft diameter, and chamfer the aperture to prevent graft abrasion.
- Pass the graft via a passing suture through the tibial then the femoral tunnel.
- For suspensory femoral fixation, flip the button on the lateral cortex and confirm with fluoroscopy; for aperture fixation use an interference screw.
- Fix the tibial side with a 7-9 mm interference screw at 20-30 degrees flexion under 80-100 N tension; cycle the knee 20 times through full range before final screw insertion.
- Confirm no notch impingement in full extension and no PCL impingement in flexion.
- Close all portals with absorbable suture; close the harvest incision in layers (rectus fascia, subcutaneous, skin).
- Apply a sterile dressing and a hinged knee brace locked in extension; no drain is required.
The harvest incision is centred 2-3 cm proximal to the superior pole of the patella in the midline; split the paratenon and rectus femoris fascia longitudinally. Measure tendon width before harvest and leave at least 5 mm of tendon on each side of the 10 mm strip. When taking a bone block, use a depth stop and keep the osteotomy within the central 15 mm and no deeper than 8 mm; close the defect in layers before arthroscopy to minimise fluid extravasation.
The trap is placing the femoral tunnel too anterior (the high-noon position) by failing to identify the lateral intercondylar ridge on the medial wall of the lateral femoral condyle. The ridge defines the posterior limit of the footprint; the anatomic centre lies 6-8 mm anterior to the posterior wall and immediately distal to the ridge. Through the anteromedial portal in deep flexion (greater than 120 degrees) the whole medial wall is visible — place the pin posteriorly, cycle the knee and confirm posterior-wall integrity before over-reaming. Malposition greater than 3 mm anterior or posterior to the anatomic centre dramatically increases failure risk: anterior placement lengthens the graft in flexion and impinges in extension; posterior placement over-constrains and limits flexion; vertical tunnels fail to control rotation.
- Patellar fracture: osteotomy wider than 15 mm or deeper than 8-10 mm, or extension into a facet — recognise the crack or step-off intraoperatively and fix immediately.
- Posterior wall blowout: femoral tunnel placed too posterior — maintain knee flexion greater than 90 degrees during reaming and confirm wall integrity before over-reaming.
- Short femoral tunnel (less than 20 mm intraosseous): compromises fixation — plan suspensory fixation when the tunnel is short.
- Popliteal artery: lies 10-15 mm posterior to the tibial tunnel exit — keep the knee flexed and the guide controlled during tibial reaming.
- Cyclops lesion: residual stump or anterior notch osteophytes cause an extension block — debride thoroughly and confirm full extension after graft passage.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation & weight-bearing | Therapy focus & goal | |-------|--------|--------------------------------|----------------------| | 1 | 0-2 weeks | Brace locked in extension 2-3 weeks (longer if bone block harvested); weight-bearing as tolerated with crutches | Quadriceps sets, straight-leg raises, ankle pumps, patellar mobilisation, cryotherapy. Goal: full extension, 90 degrees flexion, independent straight-leg raise | | 2 | 3-8 weeks | Brace progressively unlocked; transition to functional brace at 4-6 weeks | Progressive open- and closed-chain strengthening; stationary bike, elliptical, swimming once healed; NMES if activation poor. Goal: greater than 80 percent quadriceps symmetry, full painless ROM | | 3 | 9-16 weeks | Brace weaned | Single-leg strengthening, perturbation and balance training; plyometrics from 12-16 weeks. Goal: greater than 85 percent quadriceps symmetry, hop test greater than 85 percent | | 4 | 5-9+ months | None | Sport-specific agility, cutting and pivoting drills; ACL-RSI assessment. Goal: greater than 90 percent quadriceps and hop symmetry; return to pivoting sport at 9-12 months | Return-to-sport criteria (evidence-based)
- Quadriceps strength symmetry greater than 90 percent (isokinetic testing at 60 and 180 degrees per second)
- Single-leg hop test symmetry greater than 90 percent (single, triple, crossover, timed)
- Y-balance or star excursion balance test within 4 cm of the contralateral limb
- ACL Return to Sport after Injury (ACL-RSI) score greater than 65
- Completion of sport-specific training without apprehension
- Surgeon and physical therapist clearance Complications
- Incidence
- 0.5-1.5 percent
- Recognition
- Crack or loss of resistance during osteotomy; postoperative inability to extend, palpable step-off, radiographic confirmation
- Prevention & management
- Limit osteotomy to central 15 mm width and 8 mm depth with a saw depth-stop; immediate screw fixation or tension-band wiring; protected weight-bearing and extension bracing for 6-8 weeks
- Incidence
- less than 0.5 percent
- Recognition
- Inability to actively extend the knee; palpable gap proximal to the patella; MRI confirmation
- Prevention & management
- Meticulous layered closure of rectus fascia and paratenon; immediate surgical repair with non-absorbable suture through bone tunnels or anchors; 6-8 weeks extension bracing
- Incidence
- 5-10 percent (most common technical error)
- Recognition
- Postoperative positive pivot-shift; KT-1000 side-to-side difference greater than 5 mm; CT or MRI confirms position
- Prevention & management
- Anteromedial portal with knee greater than 120 degrees flexion; identify the lateral intercondylar ridge; confirm with fluoroscopy; revise with anatomic tunnel placement
- Incidence
- 2-5 percent
- Recognition
- Extension deficit greater than 5 degrees; palpable clunk at terminal extension; MRI shows nodular scar anterior to the graft
- Prevention & management
- Thorough stump debridement and notchplasty; confirm full extension intraoperatively; arthroscopic excision and aggressive extension therapy
- Incidence
- 2-6 percent primary; 10-20 percent revision
- Recognition
- Recurrent instability; positive Lachman or pivot-shift; MRI confirms graft discontinuity or elongation
- Prevention & management
- Anatomic tunnels, adequate graft diameter, compliant rehab and criteria-based return; revise, considering lateral extra-articular tenodesis in high-risk patients
- Incidence
- 5-10 percent at 6 months
- Recognition
- Isokinetic symmetry less than 80 percent; limitation climbing stairs or jumping
- Prevention & management
- Preoperative strengthening, immediate postoperative activation, NMES if inhibited; structured progressive strengthening; delay sport until greater than 90 percent symmetry
- Incidence
- less than 1 percent
- Recognition
- Increasing pain, swelling, warmth, fever; raised CRP, ESR, WBC; synovial fluid greater than 50,000 WBC and positive culture
- Prevention & management
- Sterile technique, prophylactic antibiotics, avoid suprapatellar pouch penetration; urgent arthroscopic washout and IV antibiotics for 4-6 weeks; retain graft if stable
- Incidence
- 5-15 percent (more with suspensory fixation)
- Recognition
- Progressive tunnel enlargement on radiograph or CT; may be asymptomatic or associated with laxity
- Prevention & management
- Aperture fixation when possible, avoid aggressive early rehab, ensure graft-tunnel fill; usually observed; revision may bone-graft tunnels greater than 12 mm
Viva & Exam Focus
QUADQUAD — graft harvest and preparation
GRAFTGRAFT — femoral and tibial tunnel principles
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old professional footballer sustains a non-contact ACL rupture confirmed on MRI with a concomitant grade 2 medial meniscal tear. He has no prior knee surgery and excellent quadriceps strength. Discuss your graft choice and operative plan, including why quadriceps tendon may be preferred over hamstring or patellar tendon in this patient.”
“During ACL reconstruction with quadriceps tendon autograft, you encounter a patellar fracture while harvesting the bone block. How do you recognise, manage intraoperatively, and counsel the patient postoperatively?”
“A 28-year-old patient 8 months after ACL reconstruction with quadriceps tendon autograft reports recurrent instability with pivoting. KT-1000 shows 7 mm side-to-side difference and pivot-shift is grade 2. CT demonstrates the femoral tunnel is 5 mm anterior to the anatomic centre. How do you manage this failure?”
Graft properties & indications
- Cross-section greater than 90 mm2 — larger than hamstring or patellar tendon
- Lower anterior knee pain (5-15 percent) than bone-patellar-tendon-bone (20-40 percent)
- Preferred in revision, the skeletally immature, patellar tendon pathology and kneeling athletes
- Harvest with or without a patellar bone block; the block gives tibial aperture fixation
- Contraindicated in active infection, severe osteoarthritis or fixed malalignment greater than 10 degrees
Key surgical anatomy
- Femoral footprint: lateral intercondylar ridge is the posterior landmark; anatomic centre 6-8 mm anterior to the posterior wall
- Tibial footprint: centre 7-10 mm anterior to the PCL, 1-2 mm posterior to the anterior horn of the lateral meniscus
- Quadriceps tendon: trilaminar; harvest a central 8-10 mm full-thickness strip 60-80 mm long
- Patellar bone block: limit to central 15 mm width and 8 mm depth to avoid fracture
- Intercondylar notch: notchplasty if width less than 12 mm or osteophytes present
Operative technique — critical steps
- Anteromedial portal with the knee at 120-130 degrees flexion for the femoral tunnel
- Identify the lateral intercondylar ridge and bifurcate ridge before drilling the femoral tunnel
- Place the tibial guide tip at the footprint centre; chamfer the aperture
- Tension at 20-30 degrees flexion with 80-100 N; cycle 20 times before final tibial fixation
- Confirm no notch impingement in extension and no PCL impingement in flexion before closure
Danger zones & prevention
- Patellar fracture: limit osteotomy to 15 mm width and 8 mm depth; immediate fixation if it occurs
- Femoral tunnel malposition: anterior placement causes rotational failure; use the ridge landmarks
- Quadriceps tendon rupture: meticulous layered closure of rectus fascia; less than 0.5 percent incidence
- Cyclops lesion: thorough debridement and notchplasty; causes an extension block
- Popliteal artery: 10-15 mm posterior to the tibial tunnel; keep the knee flexed greater than 90 degrees when drilling
Complications & management
- Patellar fracture 0.5-1.5 percent: immediate fixation, 6-8 weeks extension bracing
- Graft failure 2-6 percent primary: most often anterior femoral tunnel; revise with anatomic placement
- Persistent quadriceps weakness 5-10 percent at 6 months: structured strengthening; delay sport until greater than 90 percent symmetry
- Infection less than 1 percent: urgent washout, IV antibiotics 4-6 weeks; retain graft if stable
- Tunnel widening 5-15 percent: more common with suspensory fixation; revision may require bone grafting
Rehabilitation & return to sport
- Phase 1 (0-2 weeks): brace locked in extension, immediate quadriceps sets; goal full extension and 90 degrees flexion
- Phase 2 (3-8 weeks): progressive strengthening; NMES if inhibited
- Phase 3 (9-16 weeks): plyometrics and proprioception; goal greater than 85 percent strength symmetry
- Return-to-sport criteria: greater than 90 percent quadriceps symmetry, hop tests greater than 90 percent, ACL-RSI greater than 65
- Timeline: 9-12 months typical; earlier only if all objective criteria are met
Evidence summary
- Systematic reviews show equivalent or superior IKDC and Lysholm scores versus hamstring and patellar tendon at 2-5 years
- Graft failure rates 2-6 percent at 2 years in primary reconstruction
- Return to sport greater than 80 percent when objective criteria are used
- Quadriceps weakness is transient in most; greater than 90 percent symmetry by 6-9 months with structured rehab
- Lower donor-site morbidity than bone-patellar-tendon-bone in kneeling athletes
Background & Evidence
Graft properties and biomechanics. The quadriceps tendon is a trilaminar structure (superficial rectus femoris, middle vastus lateralis and medialis, deep vastus intermedius) whose central third can be harvested without compromising the extensor mechanism when closed properly. Its cross-sectional area averages 90-110 mm2 versus 35-50 mm2 for four-strand hamstring and 45-60 mm2 for bone-patellar-tendon-bone, and its ultimate tensile strength exceeds 2000 N — comparable to the native ACL and superior to doubled hamstring in most cadaveric studies. Donor-site morbidity is lower than bone-patellar-tendon-bone: anterior knee pain at two years is reported in 5-15 percent versus 20-40 percent for patellar tendon, and harvest-site quadriceps weakness is transient, with isokinetic testing returning to greater than 90 percent symmetry by 6-9 months with structured rehabilitation. Comparative outcomes. Systematic reviews demonstrate equivalent or superior patient-reported outcomes (IKDC, Lysholm, KOOS) compared with hamstring and patellar tendon autografts at 2-5 year follow-up. Graft failure rates in primary reconstruction range from 2-6 percent at two years — comparable to other autografts — with lower revision rates in some high-risk series. Return-to-sport rates exceed 80 percent at 9-12 months when objective criteria (strength symmetry, hop testing, psychological readiness) rather than time alone guide clearance. Surgical anatomy (reference). The ACL femoral footprint lies on the medial wall of the lateral femoral condyle; the lateral intercondylar ridge (resident's ridge) defines the posterior limit of the footprint and the bifurcate ridge separates the anteromedial and posterolateral bundle footprints. The anatomic centre sits approximately 6-8 mm anterior to the posterior wall and 2-3 mm proximal to the inferior articular margin — placement posterior to the ridge risks posterior wall blowout, and anterior placement causes rotational instability. The tibial footprint lies in the centre of the intercondylar eminence just anterior and medial to the PCL insertion; the anterior horn of the lateral meniscus is the key landmark, the centre lying 1-2 mm posterior to it and the anterior edge approximately 7-10 mm anterior to the PCL. A tibial tunnel placed too anterior impinges in extension and one too posterior causes rotational laxity. A notch width index less than 0.2 is associated with increased ACL injury risk; notchplasty of 2-4 mm from the roof and lateral wall is performed when the intercondylar notch is stenotic (less than 12 mm) or osteophytes are present.
References
Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Outcomes for Quadriceps Tendon Autograft Versus Bone-Patellar Tendon-Bone and Hamstring-Tendon Autografts
- Meta-analysis of 15 studies, 1482 patients comparing quadriceps tendon versus bone-patellar-tendon-bone autograft
- No significant difference in graft failure rates or patient-reported outcomes at 2-5 years
- Anterior knee pain significantly lower with quadriceps tendon (5-15 percent versus 20-40 percent)
Is Quadriceps Tendon Autograft a Better Choice Than Hamstring Autograft for Anterior Cruciate Ligament Reconstruction? A Comparative Study With a Mean Follow-up of 3.6 Years
- Comparative study with mean 3.6 year follow-up; quadriceps tendon autograft showed good clinical outcomes and lower donor-site morbidity versus hamstring
Graft Failure Rates in Bone-Patellar Tendon-Bone, Hamstring, and Quadriceps Tendon Autografts in Patients Younger Than 25 Years: A Meta-analysis
- Meta-analysis of graft failure rates including quadriceps tendon autograft in high-risk young patients
Comparison of Autograft Types in Anterior Cruciate Ligament Reconstruction: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Clinical Trials
- Network meta-analysis of randomized trials comparing autograft types including quadriceps tendon for ACL reconstruction