Structural fresh-frozen allograft reconstruction of segmental defects after wide resection | advanced
- Allograft is indicated when the goal is biologic reconstruction with restoration of bone stock and soft-tissue attachment sites — particularly in young patients with diaphyseal or intercalary defects and in osteoarticular reconstructions where ligament or tendon reattachment is required.
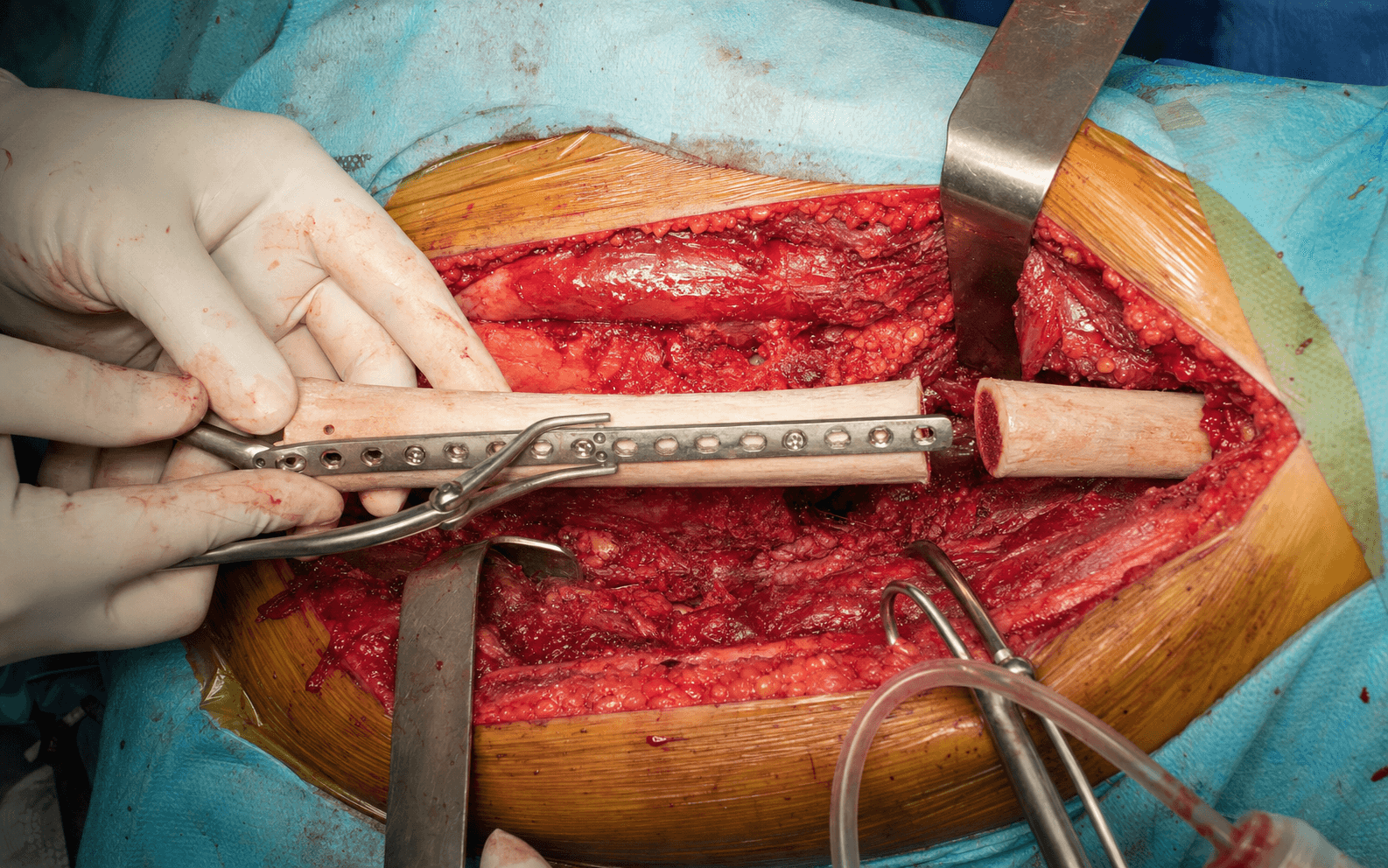
- Fresh-frozen size-matched allograft is the standard; the graft must be rigidly fixed with plates or an intramedullary device that spans both host-graft junctions by at least two cortical diameters on each side. Supplemental autograft at the junctions and meticulous compression are mandatory to promote union.
- Nonunion at the host-graft junction occurs in 10-30 percent of cases and is the most common cause of failure — risk factors include chemotherapy, radiation, infection, and inadequate fixation or compression. Management requires revision fixation, autografting and optimisation of biology.
- Deep infection (5-15 percent) and allograft fracture (5-15 percent) are the other major complications that define this reconstruction; infection often necessitates graft removal and staged revision, while fracture may be treated with internal fixation if the graft is otherwise incorporated.
When & Why
Indication. Structural fresh-frozen allograft is used to reconstruct a segmental bone defect after the wide resection of a bone tumour, when the goal is biologic reconstruction — restoring living-quality bone stock and providing sites for tendon and ligament reattachment — rather than simply bridging the gap with metal. It is chosen in three broad situations: - Absolute indications - A diaphyseal or intercalary segmental defect after wide resection of a bone sarcoma (osteosarcoma, Ewing sarcoma, chondrosarcoma) in a patient younger than 40-50 years who desires biologic reconstruction and restoration of bone stock. - An osteoarticular defect requiring joint surface and ligament reconstruction (proximal tibia, distal femur, proximal humerus) in a young, high-demand patient. - The need for tendon or ligament attachment sites that cannot be achieved with a megaprosthesis (patellar tendon, hip abductors, rotator cuff). - Patient preference for allograft after informed discussion of the risks versus endoprosthetic reconstruction.
- Relative indications - Allograft-prosthesis composite (APC) when the joint surface is not reconstructible with osteoarticular allograft but soft-tissue attachment is still desired. - Revision of a failed megaprosthesis where bone stock restoration is required for future longevity. - Aggressive benign tumours (giant cell tumour, chondroblastoma) with massive bone loss after curettage and resection. Contraindications. Absolute: active infection at the resection site, inability to achieve wide surgical margins, patient non-compliance with prolonged protected weight-bearing (minimum 6 months), and severe immunocompromise or uncontrolled diabetes with high infection risk. Relative: age greater than 60-65 years (megaprosthesis usually preferred for faster rehabilitation), a requirement for post-operative radiation (increases nonunion and fracture risk), and smoking or a poor soft-tissue envelope that cannot be optimised. The decision — allograft versus megaprosthesis. This is the central pre-operative choice, and it drives everything that follows:
Superior long-term bone stock restoration and the option for biologic tendon or ligament attachment. The trade-off is a 20-40 percent major complication rate in the first two years and 6-18 months of protected weight-bearing. Favoured in patients younger than 40 years with diaphyseal defects when the soft-tissue envelope allows.
A cemented prosthesis implanted into the allograft on the back table — combines prosthetic joint stability with biologic tendon attachment. Indicated when the joint surface cannot be reliably reconstructed with osteoarticular allograft but soft-tissue reattachment (e.g. patellar tendon) is still wanted.
Immediate stability and faster return to weight-bearing (6-12 weeks), but it sacrifices bone stock and future revision options, and tendon reattachment to metal is inferior. Preferred when rapid rehabilitation is the priority or the soft-tissue envelope is poor.
Choose allograft over megaprosthesis in patients younger than 40-50 years with diaphyseal defects, when future revision surgery is anticipated, and when tendon or ligament attachment to the reconstruction is required — for example patellar tendon reconstruction in proximal tibial resection. In these patients the biologic advantages usually outweigh the slower recovery.
Evidence for allograft reconstruction. Fresh-frozen structural allografts achieve union in 60-80 percent of host-graft junctions when rigid fixation and autograft augmentation are used. Osteoarticular allografts carry higher complication rates (fracture, joint degeneration) than intercalary grafts but preserve the option for biologic joint reconstruction in young patients. APCs combine the advantages of both techniques and are particularly useful in the proximal tibia, where patellar tendon reattachment is critical. Against a megaprosthesis, allograft offers superior long-term bone stock and the possibility of tendon attachment but requires 6-18 months of protected weight-bearing and carries a 20-40 percent major complication rate in the first two years. Consent. Discuss nonunion (10-30 percent), fracture (5-15 percent), infection (5-15 percent), disease transmission (less than 1 in 1 million), prolonged protected weight-bearing (6-18 months), and the possibility of graft removal and revision to megaprosthesis or amputation if complications occur. Setup. Supine on a radiolucent table with the entire limb prepared and draped free. A tourniquet is usually not used because of the length of the procedure and the need for proximal exposure; a bump under the ipsilateral buttock facilitates lateral access if needed. A size-matched fresh-frozen allograft is ordered from an accredited tissue bank after CT templating of both the defect and the contralateral limb; the graft is thawed in warm saline on the morning of surgery and cultured, and autograft is harvested from the iliac crest or obtained from reamings if an intramedullary nail is used.
The Operation
The goal: restore a segmental defect after wide tumour resection with a fresh-frozen structural allograft that is rigidly fixed under compression at both host-graft junctions, biologically augmented with autograft, and overlaid with a healthy soft-tissue envelope. The exposure is the wide resection itself — performed through the approach appropriate to the tumour (for the distal femur example, the anterolateral femoral shaft or medial parapatellar approach) — and it is laid out in full as the first steps below.
Operative sequence — intercalary allograft (distal femur example)
- Supine on a radiolucent table, entire limb prepared and draped free; no tourniquet (long procedure, need proximal exposure); bump under the ipsilateral buttock for lateral access.
- The size-matched fresh-frozen allograft (diameter within 1-2 mm of the host canal) is thawed in warm saline on the morning of surgery and cultured; autograft is harvested from the iliac crest or from reamings if an intramedullary nail is planned.
- Approach through the incision appropriate to the tumour — for a distal femur example, the anterolateral femoral shaft or medial parapatellar approach as indicated.
- Perform the planned wide resection of the bone tumour, protecting the neurovascular bundle throughout.
- Obtain frozen-section confirmation of margins, then measure the defect length and diameter precisely so the graft can be trimmed to match.
- Trim the thawed allograft to the exact length required with an oscillating saw under irrigation.
- Create step-cut or oblique ends to increase the surface area and rotational stability at the junctions.
- Drill any planned screw holes or tendon attachment sites before implantation, and culture the graft.
- Freshen the host bone ends with a saw to bleeding bone.
- If an intramedullary nail is planned, ream the host canal to accept the largest possible nail.
- If plate fixation is used, contour the plate or plates to the host and graft before final insertion.
- Insert the graft and achieve compression at both junctions.
- Apply the spanning fixation construct — dual compression plates in different planes, or a locked intramedullary nail with a supplemental plate.
- Confirm that at least two cortical diameters of host bone are engaged on each side.
- Impact autograft around both junctions to promote creeping substitution.
- Reattach any resected tendons or ligaments to the allograft using heavy non-absorbable suture through drill holes (or through the preserved soft-tissue sleeve on the graft).
- If a muscle flap is required (gastrocnemius, soleus, latissimus), perform or coordinate the flap coverage before closure.
- Close the wound over drains with meticulous haemostasis.
- Obtain intra-operative radiographs to confirm alignment, fixation length and junction compression.
- Check that the limb is stable through a full range of motion and that any joint reconstruction is congruent.
Inadequate overlap of fixation on host bone creates a stress riser and leads to early failure. A gap at the junction greater than 1 mm dramatically increases nonunion risk — accept no visible gap, and shorten the graft or add an intercalary segment rather than compromise. During insertion, protect the allograft articular surface (if osteoarticular) and guard the neurovascular bundle during graft manipulation and drilling.
Achieve absolute compression at the host-graft junctions before applying the final fixation — use lag screws or a compression device across the junction, then lock the construct. Any visible gap is unacceptable; shorten the graft or add a small intercalary segment rather than accept a gap.
Osteoarticular and APC variants. For an osteoarticular allograft, joint surface matching is confirmed on the back table before implantation, and the joint capsule and ligaments are reconstructed under appropriate tension with the joint reduced; for a proximal tibial osteoarticular graft the patellar tendon is reattached to the allograft tibial tubercle with transosseous sutures or anchors. For an allograft-prosthesis composite (APC), when the joint surface cannot be reliably reconstructed with osteoarticular allograft, a cemented prosthesis is implanted into the allograft on the back table and the composite is fixed to the host with the same junction principles; the patellar tendon or other soft tissues attach to the allograft portion of the composite.
An APC combines the biologic advantages of allograft (tendon attachment) with the immediate stability of a cemented prosthesis — indicated when the joint surface cannot be reliably reconstructed with osteoarticular allograft alone, particularly in the proximal tibia where patellar tendon reattachment is critical.
Aftercare & Complications
Rehabilitation | Phase | Timing | Weight-bearing & protection | Priorities | |-------|--------|-----------------------------|------------| | Early | Day 0 to 6 weeks | Touch-down or partial (10-20 kg) with crutches or walker | Drains out at 48 h; 24-48 h IV antibiotics; DVT prophylaxis; gentle active-assisted ROM | | Union monitoring | 6 weeks to union | Continued protected weight-bearing | Serial radiographs at 6 weeks, 3, 6, 9 and 12 months, then 6-monthly; CT if equivocal at 9-12 months | | Return to function | After union (6-18 months) | Progress to full weight-bearing | Progressive resistance; low-impact activity permitted; high-impact generally discouraged | Union is defined as bridging callus on two orthogonal views without a radiolucent line at either junction, and protected weight-bearing continues until union is confirmed. Strengthening begins once full weight-bearing is allowed; return to high-impact sport is generally discouraged, while low-impact activities (swimming, cycling) may be permitted after union. Oncologic surveillance with local and systemic imaging continues per protocol throughout. Managing nonunion. Nonunion is declared only after 12 months — or 18 months in patients who received chemotherapy or radiation — with no radiographic progress. Low-grade infection must be excluded by aspiration or biopsy before any revision. Revision options are compression plating with autograft (iliac crest or vascularised fibula), exchange nailing with compression and autograft if an IM nail was used initially, a bone stimulator or anabolic agents (teriparatide) in recalcitrant cases, and — if multiple revisions fail or infection is present — conversion to megaprosthesis or amputation.
Host-graft junction union is assessed on serial radiographs by the presence of bridging callus and the absence of radiolucent lines; CT is used when plain films are equivocal. Union typically occurs between 6 and 18 months, and protected weight-bearing continues until radiographic union — so do not declare nonunion before 12 months unless there is clear hardware failure or infection.
Complications
- Incidence
- 10-30 percent
- Recognition
- Persistent radiolucent line at the junction beyond 12 months; lack of bridging callus on orthogonal radiographs; hardware loosening or failure; pain on weight-bearing
- Prevention and management
- Prevention: rigid spanning fixation with compression, autograft at both junctions, optimise nutrition and stop smoking, consider a bone stimulator in high-risk patients (chemotherapy, radiation). Management: revision fixation with compression, additional autograft or vascularised fibula; rule out infection first with aspiration or biopsy
- Incidence
- 5-15 percent
- Recognition
- Sudden pain and deformity; fracture through a screw hole, at the junction or within the graft diaphysis on radiographs; loss of fixation
- Prevention and management
- Prevention: largest possible IM nail or dual-plate fixation in different planes; avoid unnecessary stress risers; protect until radiographic union (often 12-18 months). Management: internal fixation with or without autograft if the graft is otherwise incorporated; revision to megaprosthesis if extensively fractured or infected
- Incidence
- 5-15 percent
- Recognition
- Erythema, warmth, swelling, sinus tract; elevated CRP or ESR; positive aspiration culture; graft loosening or resorption on imaging
- Prevention and management
- Prevention: strict asepsis, laminar flow, perioperative antibiotics, muscle-flap coverage when the soft-tissue envelope is poor, avoid surgery during chemotherapy-induced neutropenia. Management: urgent aspiration; if confirmed, staged graft removal, antibiotic spacer, prolonged IV antibiotics (6-8 weeks), then revision to megaprosthesis or repeat allograft after clearance
- Incidence
- 5-10 percent
- Recognition
- Progressive loss of graft density and volume on serial radiographs; fracture through the weakened graft; loss of structural integrity
- Prevention and management
- Prevention: rigid fixation and compression to promote creeping substitution; avoid radiation when possible. Management: observation if asymptomatic; fixation or revision if fracture or instability develops
- Incidence
- 20-40 percent at 5 years
- Recognition
- Progressive joint-space narrowing, osteophytes, subchondral collapse on radiographs; pain and stiffness
- Prevention and management
- Prevention: size-matched graft with a congruent articular surface; stable ligament reconstruction. Management: convert to total knee or shoulder arthroplasty when symptomatic; the allograft bone stock facilitates revision
- Incidence
- 5-10 percent
- Recognition
- Gait abnormality; measured discrepancy on scanogram; pelvic tilt
- Prevention and management
- Prevention: precise pre-operative templating and intra-operative measurement of resection length; consider contralateral epiphysiodesis in skeletally immature patients. Management: shoe lift for discrepancies less than 2 cm; lengthening procedure or contralateral epiphysiodesis for larger discrepancies
Infection risk is higher than with an endoprosthesis because the avascular graft provides a nidus. Deep infection rates of 5-15 percent exceed those of megaprosthesis, and once established, eradication usually requires graft removal, prolonged antibiotics and staged reconstruction. Perioperative antibiotics, laminar-flow theatre and meticulous soft-tissue coverage are critical, and any suspicion mandates urgent aspiration and staged management.
Viva & Exam Focus
GRAFTGRAFT — structural allograft principles
UNIONUNION — monitoring and managing the host-graft junctions
The trap. Treating the host-graft junction like a standard fracture — the allograft is avascular and provides no living cells or growth factors; union depends entirely on creeping substitution from the host. The fix. Achieve absolute stability with compression plating or IM nailing spanning at least two cortical diameters on each side. Impact fresh autograft (iliac crest or reamings) circumferentially at both junctions. Avoid gaps greater than 1 mm. Chemotherapy and radiation delay union — plan for longer protected weight-bearing.
Location. Stress risers at screw holes, the junction itself, or within the graft diaphysis where vascular ingrowth is incomplete. Risk. 5-15 percent incidence; higher with osteoarticular allografts and when adjuvant radiation is used. The graft never fully remodels to living bone — it remains a structural scaffold prone to fatigue failure. Prevention. Use the largest-diameter IM nail possible or multiple plates in different planes. Avoid unnecessary screw holes. Protect the reconstruction until radiographic union (minimum 6 months, often 12-18 months).
Why it is different. The allograft is a large avascular foreign body. Deep infection rates (5-15 percent) exceed those of megaprosthesis. Once infected, eradication usually requires graft removal, prolonged antibiotics and staged reconstruction. Prevention. Strict aseptic technique, laminar-flow theatre, perioperative antibiotics for 24-48 hours (or longer with chemotherapy-induced neutropenia), meticulous soft-tissue coverage and muscle flaps when needed. Any post-operative wound issue must be treated aggressively.
The principle. A main advantage of allograft over megaprosthesis is the ability to reattach host tendons and ligaments directly to the graft (patellar tendon, rotator cuff, hip abductors). Technique. Heavy non-absorbable sutures through drill holes in the graft or through the preserved soft-tissue sleeve. For osteoarticular grafts, reconstruct the joint capsule and ligaments as in a revision arthroplasty. Failure mode. Poor reattachment leads to instability, subluxation or dislocation — particularly devastating in proximal humerus or proximal tibia reconstructions.
Risk. Viral transmission (HIV, hepatitis) is now less than 1 in 1 million with modern screening, but bacterial contamination during procurement or processing remains a concern. Selection. Use only grafts from accredited tissue banks with negative cultures, serology and irradiation where indicated. Size matching is critical — a graft more than 2 mm smaller in diameter than the host canal leads to poor fit and fixation failure. Storage. Fresh-frozen at minus 80 degrees Celsius is standard; never use freeze-dried grafts for structural applications because of reduced mechanical strength.
The trap. Offering allograft to every young patient without considering the higher early complication rate and slower rehabilitation. The reality. Allograft offers superior long-term bone stock and biologic attachment but at the cost of a 20-40 percent major complication rate in the first two years. Megaprosthesis provides immediate stability and faster return to function but sacrifices future revision options. Decision factors. Patient age, defect location (diaphyseal favours intercalary allograft), need for tendon attachment, anticipated adjuvant therapy, and patient tolerance for prolonged protected weight-bearing.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old man undergoes wide resection of a distal femoral osteosarcoma with a 12 cm intercalary defect. He has completed neoadjuvant chemotherapy and is eager to return to construction work. Discuss your choice of reconstruction and the key technical points.”
“A 35-year-old woman with a proximal tibial giant cell tumour has undergone wide resection with sacrifice of the patellar tendon insertion. She desires reconstruction that maximises her chance of returning to recreational running. Compare allograft-prosthesis composite versus megaprosthesis.”
“A 42-year-old man with a distal femoral osteosarcoma treated with neoadjuvant chemotherapy and wide resection with intercalary allograft reconstruction now presents at 16 months with persistent pain on weight-bearing. Radiographs show no bridging callus at the proximal host-graft junction and a 2 mm gap. How do you approach this?”
Indications
- Young patient (younger than 40-50 years) with a diaphyseal or intercalary defect after wide resection
- Desire for biologic reconstruction and restoration of bone stock for future revision
- Need for tendon or ligament attachment (patellar tendon, hip abductors, rotator cuff)
- Osteoarticular reconstruction when joint surface matching is achievable
- APC when the joint surface cannot be reliably reconstructed but soft-tissue attachment is required
Key technical principles
- Size-matched fresh-frozen allograft from an accredited tissue bank (diameter within 1-2 mm of host)
- Rigid spanning fixation with compression at both host-graft junctions (minimum two cortical diameters overlap)
- Impacted autograft at every junction to promote creeping substitution
- Tendon reattachment through drill holes or the preserved soft-tissue envelope on the allograft
- Muscle-flap coverage when the soft-tissue envelope is compromised
Host-graft junction biology
- The allograft is avascular — union occurs by creeping substitution from the host over 6-18 months
- Compression and absolute stability are mandatory; a gap greater than 1 mm increases nonunion risk
- Chemotherapy and radiation delay union — plan for longer protected weight-bearing
- Nonunion is declared only after 12-18 months with no radiographic progress
- Infection must be excluded before any revision for nonunion
Major complications
- Nonunion (10-30 percent): revision compression plating, autograft, optimise biology
- Allograft fracture (5-15 percent): internal fixation if graft incorporated; revision to megaprosthesis if extensive
- Deep infection (5-15 percent): staged removal, antibiotic spacer, conversion to megaprosthesis
- Graft resorption and joint degeneration (osteoarticular): surveillance and conversion when symptomatic
- Limb-length discrepancy: shoe lift or contralateral epiphysiodesis
Rehabilitation principles
- Protected weight-bearing (touch-down to partial) for a minimum of 6 months, often 12-18 months
- Serial radiographs at 6 weeks, 3, 6, 9 and 12 months until union confirmed
- CT if plain films are equivocal at 9-12 months
- Full weight-bearing only after bridging callus on two orthogonal views
- High-impact activities generally discouraged; low-impact permitted after union
Allograft versus megaprosthesis decision
- Allograft: superior bone stock restoration, biologic tendon attachment, slower rehabilitation, higher early complication rate
- Megaprosthesis: immediate stability, faster return to function (6-12 weeks), sacrifices future revision options
- APC: combines prosthetic joint with biologic tendon attachment — useful in the proximal tibia
- Choose allograft in young patients with diaphyseal defects when biology can be optimised
- Choose megaprosthesis when rapid rehabilitation is the priority or the soft-tissue envelope is poor
Special situations
- Osteoarticular allograft: size-matched joint surface, ligament reconstruction, higher degeneration risk
- APC: cemented prosthesis in allograft on the back table, tendon attachment to the allograft portion
- Infection: staged removal and conversion to megaprosthesis; repeat allograft rarely successful
- Nonunion revision: compression plating or exchange nailing plus autograft or vascularised fibula
- Paediatric patients: consider contralateral epiphysiodesis for length discrepancy
Background & Evidence
Host-graft junction biology. The success of structural allograft reconstruction depends on understanding that the graft is avascular. Union occurs by creeping substitution — host vessels and osteoblasts invade the graft from the junction, resorbing and replacing necrotic bone over months to years. The central portion of a long intercalary graft may remain avascular indefinitely, which is why fixation must protect the junctions until union and why the graft never fully remodels to living bone. Fixation principles. The fixation construct must span both host-graft junctions with sufficient working length on the host bone (minimum two cortical diameters) to resist bending and torsional forces during the prolonged healing period. Compression at the junction is achieved with lag screws or compression plating; any gap greater than 1 mm dramatically increases nonunion risk. When an intramedullary nail is used it must be locked proximally and distally, and the junctions should still receive supplemental plate or cerclage compression where possible. Soft-tissue considerations. The soft-tissue envelope after tumour resection is often compromised by the resection itself and by adjuvant therapy. Muscle flaps (gastrocnemius, soleus, latissimus) are frequently required to cover the allograft and provide a vascularised bed. Tendon reattachment (patellar tendon, hip abductors, rotator cuff) is performed with heavy non-absorbable suture through drill holes or through the preserved soft-tissue sleeve on the allograft. For osteoarticular grafts, joint surface matching is critical — the donor is size-matched on pre-operative CT, the articular cartilage is preserved during implantation, and the capsule and ligaments are sutured to the corresponding structures on the allograft under appropriate tension. Graft selection and storage. Use only grafts from accredited tissue banks with negative cultures, serology and irradiation where indicated; size matching is critical, as a graft more than 2 mm smaller in diameter than the host canal leads to poor fit and fixation failure. Fresh-frozen storage at minus 80 degrees Celsius is standard; freeze-dried grafts must never be used for structural applications because of reduced mechanical strength. Viral transmission (HIV, hepatitis) is now less than 1 in 1 million with modern screening, but bacterial contamination during procurement or processing remains a concern.
- Best for
- Diaphyseal defects with preserved joints in young patients
- Advantages
- Biologic reconstruction, restores bone stock, joints preserved
- Trade-offs
- Union 60-80 percent; 6-18 months protected weight-bearing; nonunion 10-30 percent
- Best for
- Young, high-demand patients needing biologic joint reconstruction
- Advantages
- Joint surface plus ligament and capsule reattachment
- Trade-offs
- Joint degeneration 20-40 percent at 5 years; higher fracture rate
- Best for
- Joint surface not reconstructible but tendon attachment wanted (e.g. proximal tibia)
- Advantages
- Prosthetic stability plus biologic tendon attachment
- Trade-offs
- Surveillance for both prosthetic loosening and junction union
- Best for
- Older patients, poor soft-tissue envelope, or when rapid rehab is the priority
- Advantages
- Immediate stability, faster return to weight-bearing (6-12 weeks)
- Trade-offs
- Sacrifices bone stock and future revision options; inferior tendon attachment
References
Long-term results of allograft reconstruction after resection of bone tumours
- Large single-institution series of structural allografts with greater than 20-year follow-up
- Overall success rate approximately 70 percent at 10 years when union was achieved
- Major complications were nonunion (15-20 percent), fracture (10-15 percent) and infection (8-12 percent)
Allograft-prosthesis composite reconstruction of the proximal tibia after tumour resection
- Comparative series of allograft-prosthesis composites versus megaprostheses for proximal tibial reconstruction
- APC provided superior extensor mechanism function and patellar tendon reattachment
- Nonunion at the host-graft junction remained the most common complication requiring revision
Allograft reconstruction of intercalary defects after bone tumour resection
- Early series establishing intercalary allograft as a viable option for diaphyseal defects
- Union rates improved with rigid plate fixation spanning the junctions and supplemental autograft
- Limb salvage rates greater than 80 percent when infection was avoided
Observations on massive retrieved human allografts
- Histologic study of retrieved massive human allografts showed persistent central avascularity and slow creeping substitution over years
- Union at host-graft junctions occurs by host-derived creeping substitution; the graft itself remains largely necrotic
- Complications correlated with extent of revascularization and mechanical stress at junctions