Lateral Thigh | Fascia Lata Split | Vastus Lateralis Elevation | Perforator Ligation
- Lateral thigh incision in line with the greater trochanter and the lateral femoral condyle.
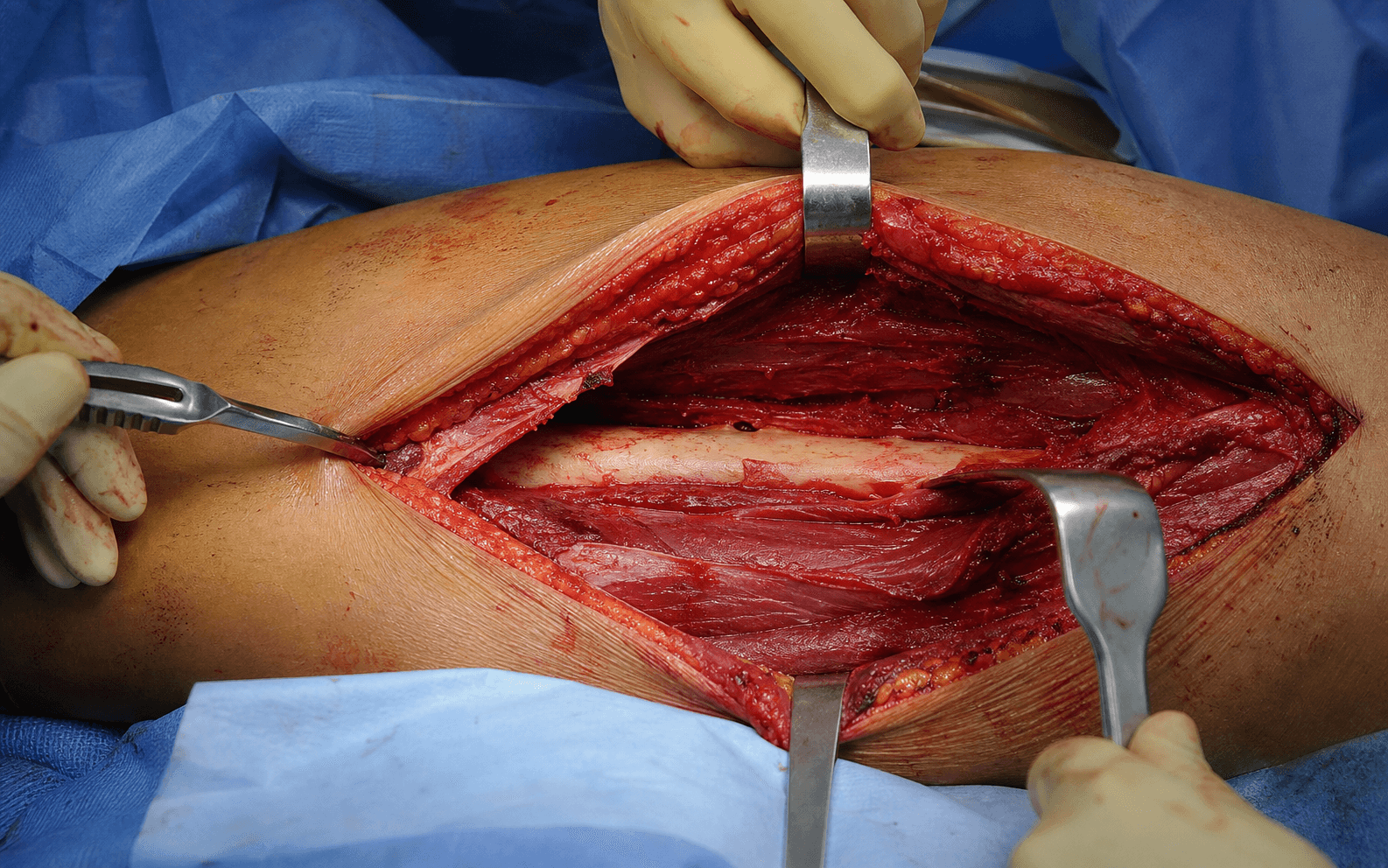
- Split the fascia lata longitudinally, then elevate vastus lateralis anteriorly off the lateral intermuscular septum.
- Ligate the perforating branches of profunda femoris as they pierce the septum - the key bleeding step.
- The femoral neurovascular bundle lies medial to the femur - stay strictly subperiosteal on bone.
- There is no true internervous plane - vastus lateralis is elevated, not divided.
When & Why
What it exposes. The anterolateral approach gives direct access to the lateral and anterior surfaces of the femoral shaft. It allows direct visualisation for fracture reduction, application of a lateral or anterior plate, and placement of anterior bone graft. The femoral neurovascular bundle is safely medial and the approach avoids the posterior compartment structures. Primary indications. Femoral shaft fractures requiring open reduction and plate fixation; aseptic nonunion of the femoral shaft needing direct bone grafting; malunion requiring corrective osteotomy and plating; pathological fractures requiring curettage and stabilisation; and anterior bone grafting for delayed union. Why this approach is chosen. It is the workhorse exposure for femoral shaft plating whenever intramedullary nailing is not feasible (for example a narrow canal) or when direct reduction and stable plate fixation with anterior bone grafting are required. Contraindications. Active infection at the surgical site; severe soft-tissue compromise over the lateral thigh requiring an alternative exposure; patient factors precluding supine or lateral positioning; and isolated medial femoral pathology better addressed by a medial approach. Alternative approaches. A lateral approach that splits the vastus lateralis in its substance rather than elevating it from the septum; a posterior approach for posterior-cortex access or when lateral soft tissues are compromised; minimally invasive percutaneous plating when indirect reduction is acceptable; and antegrade or retrograde nailing when intramedullary fixation is preferred. Position & landmarks. The patient is supine on a radiolucent table with a small bump under the ipsilateral buttock to neutralise femoral rotation. Pad all pressure points, keep the arms abducted less than 90 degrees or tucked, and confirm full-length femur fluoroscopy in AP and lateral with a C-arm. The knee is flexed 10 to 20 degrees over a bolster to relax the quadriceps, and the leg is draped free with an optional high thigh tourniquet. The greater trochanter marks the proximal end and the lateral femoral condyle the distal end of a longitudinal lateral-thigh incision; the linea aspera is felt posteriorly once vastus lateralis is elevated, and the lateral intermuscular septum is the firm deep plane.
A high thigh tourniquet is useful for a bloodless field but limits proximal exposure. For fractures near the lesser trochanter consider tourniquet-free surgery or a sterile tourniquet applied after the proximal dissection is complete.
The Exposure
Work down through the layers of the lateral thigh: split the fascia lata, identify the lateral intermuscular septum, and elevate vastus lateralis anteriorly off it - systematically ligating each perforating branch of profunda femoris as it pierces the septum - until the anterolateral femur is exposed subperiosteally. The plane. There is no true internervous plane: the entire quadriceps, including vastus lateralis, is supplied by the femoral nerve. The dissection is therefore an intermuscular plane anterior to the lateral intermuscular septum. Vastus lateralis is elevated anteriorly (medially in the wound) from its septal attachment, preserving the femoral nerve branches that enter its anterior surface. Staying strictly subperiosteal on the femur is what keeps the medial femoral neurovascular bundle safe.
Exposure sequence
- A longitudinal lateral-thigh incision from the greater trochanter to the lateral femoral condyle, centred over the fracture using fluoroscopy.
- Length is set by the fracture extent - typically 15 to 25 cm for mid-shaft plating.
- Stay anterior to the posterior femoral line to avoid the posterior compartment.
- Incise the thick fascia lata longitudinally in line with the skin incision.
- Place self-retaining retractors under the fascial edges to expose vastus lateralis.
- Identify the lateral intermuscular septum as a firm white longitudinal plane.
- All deep dissection stays anterior to this septum. There is no true internervous plane - the femoral nerve supplies all of the quadriceps.
- Begin proximally or distally where the plane is easiest and elevate vastus lateralis anteriorly off its attachment to the lateral intermuscular septum using a Cobb or periosteal elevator.
- Work systematically toward the fracture, preserving the femoral nerve branches that enter the muscle anteriorly. Elevation from the septum is preferred over splitting the muscle substance.
- As the muscle is elevated, the perforating branches of profunda femoris are encountered piercing the septum from posterior to anterior.
- Identify each vessel and ligate it with absorbable suture or cauterise it before division. This is the most important bleeding-control step in the approach.
- Incise the periosteum and elevate it circumferentially around the anterolateral femur as needed for plate placement.
- Stay strictly on bone to protect the medial femoral neurovascular bundle; the bundle is never visualised when the plane is correct.
The femoral artery, vein and nerve lie medial to the femur, deep to vastus medialis. Blind clamping for a brisk perforator risks devastating injury to the bundle. Control every perforator by direct vision and ligation, and pack with pressure if bleeding is brisk.
The anterolateral femoral approach is an intermuscular plane anterior to the lateral intermuscular septum: vastus lateralis (femoral nerve) is elevated medially from the septum, its nerve branches are preserved, perforators are ligated systematically, and staying subperiosteal on bone keeps the medial femoral bundle safe.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Lateral cutaneous nerve of the thigh
- Protection
- Identify and preserve if encountered proximally; division causes only sensory loss
- Structure at risk
- Perforating branches of profunda femoris (four to six in the shaft)
- Protection
- Ligate or cauterise each as it pierces the septum, before muscle elevation
- Structure at risk
- Femoral nerve branches to vastus lateralis
- Protection
- Elevate gently from the septum; avoid splitting the muscle substance
- Structure at risk
- Femoral artery, vein and nerve
- Protection
- Stay strictly subperiosteal on the anterolateral surface; never penetrate medially; never blind-clamp
- Structure at risk
- Lateral femoral circumflex artery
- Protection
- Identify near the greater trochanter; ligate if bleeding
Extensile options. Extend proximally along the greater trochanter into the Watson-Jones interval between tensor fascia lata and gluteus medius (both superior gluteal nerve) to reach the femoral neck and subtrochanteric region for long plates or combined neck-shaft fractures. Extend distally along the lateral femoral condyle, splitting the iliotibial band and elevating vastus lateralis from the condyle, for supracondylar and distal-shaft access; this can be combined with a lateral parapatellar arthrotomy if there is intra-articular extension. Both extensions remain anterior to the intermuscular septum and protect the femoral bundle. A posterior approach is reserved for posterior-cortex comminution needing direct access. Closure. Irrigate thoroughly and achieve haemostasis. Close the fascia lata securely with interrupted absorbable suture to prevent muscle herniation, then close subcutaneous tissue and skin. Apply a sterile dressing and consider a drain if dissection was extensive. Complications
- Incidence
- 3 to 5 percent
- Prevention
- Meticulous haemostasis; drain if dissection is extensive
- Treatment
- Aspiration or evacuation
- Incidence
- 1 to 3 percent
- Prevention
- Prophylactic antibiotics; careful soft-tissue handling
- Treatment
- Debridement and antibiotics
- Incidence
- 5 to 10 percent
- Prevention
- Stable fixation; bone graft for atrophic patterns
- Treatment
- Revision plating or nailing
- Incidence
- 5 to 10 percent
- Prevention
- Accurate reduction; a long plate
- Treatment
- Corrective osteotomy
- Incidence
- 10 to 15 percent
- Prevention
- Early range of motion and physiotherapy
- Treatment
- Manipulation under anaesthesia
Uncontrolled perforator bleeding occurs in up to 10 percent of cases when the vessels are not ligated systematically. Most settle with packing and pressure, but return to theatre for haematoma evacuation occurs in 2 to 3 percent. Permanent femoral nerve or vessel injury is rare, less than 1 percent, when the plane is maintained strictly on bone.
Post-operative care. Document femoral nerve function (quadriceps contraction and knee extension) on the neurovascular check. Weight bearing is touch or partial for 6 to 12 weeks depending on fracture stability and fixation, progressing on radiographic healing. Begin early passive and active-assisted knee range of motion - aim for 0 to 90 degrees by 2 weeks and full range by 6 weeks, with early quadriceps strengthening. Give DVT prophylaxis (LMWH or aspirin per institutional protocol) for a minimum of 2 to 4 weeks.
- Milestone
- Wound check and suture removal
- Milestone
- Radiographs; assess healing; progress weight bearing
- Milestone
- Radiographs; confirm union; full weight bearing
- Milestone
- Clinical and radiographic review
- Milestone
- Final assessment
Procedures Through This Approach
- Open reduction and plate fixation of femoral shaft fractures with a lateral or anterior plate, ideal when direct reduction and stable fixation are required.
- Anterior bone grafting for aseptic nonunion or delayed union, using the direct anterior-cortex access the exposure provides.
- Corrective osteotomy for malunion with plating.
- Curettage and stabilisation of pathological lesions of the shaft.
- Subtrochanteric fractures through the proximal Watson-Jones extension, and supracondylar and distal-femur fractures (distal femur ORIF) through the distal extension.
Viva & Exam Focus
LATERALLATERAL FEMUR - surgical steps
The perforating branches of the profunda femoris artery pierce the lateral intermuscular septum to reach vastus lateralis. They must be identified and ligated as the muscle is elevated; uncontrolled bleeding from them is the most common intra-operative problem.
By remaining strictly subperiosteal on the anterolateral femoral surface and never penetrating medially. The bundle lies deep to vastus medialis on the medial side of the femur and is not visualised when the plane is correct.
No. The entire quadriceps, including vastus lateralis, is supplied by the femoral nerve. The dissection is anterior to the lateral intermuscular septum and relies on muscle elevation rather than crossing a nerve plane.
Extend along the greater trochanter into the Watson-Jones interval between tensor fascia lata and gluteus medius. This gives access to the femoral neck and subtrochanteric region while remaining anterior to the intermuscular septum.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old motorcyclist sustains a closed femoral shaft fracture unsuitable for nailing due to a narrow canal. CT confirms a transverse mid-shaft pattern. How would you approach fixation?”
“A 42-year-old has an atrophic femoral shaft nonunion 9 months after intramedullary nailing. You plan to remove the nail and perform plate fixation with anterior bone grafting. Describe your surgical approach and key steps.”
“Describe how you would extend the anterolateral femoral shaft approach proximally and distally, and name the structures at risk during these extensions.”
Position
- Supine on a radiolucent table
- Ipsilateral buttock bump to neutralise rotation
- Leg draped free with an optional high thigh tourniquet
- Full femur accessible from trochanter to knee
- C-arm for AP and lateral of the entire bone
Landmarks and incision
- Greater trochanter proximally, lateral condyle distally
- Longitudinal lateral-thigh incision over vastus lateralis
- Centre the incision over the fracture using fluoroscopy
- Length 15 to 25 cm typical for mid-shaft plating
- Stay anterior to the posterior femoral line
Internervous plane
- No true internervous plane - femoral nerve supplies the quadriceps
- Dissection anterior to the lateral intermuscular septum
- Elevate vastus lateralis anteriorly from the septum
- Preserve the femoral nerve branches entering anteriorly
- Subperiosteal elevation on the femur
Danger structures
- Perforating branches of profunda femoris - ligate early
- Femoral neurovascular bundle medial - stay on bone
- Lateral femoral circumflex artery proximally
- Lateral cutaneous nerve of the thigh - preserve if possible
- No sciatic nerve risk if the plane is maintained
Key steps
- Split the fascia lata longitudinally
- Elevate vastus lateralis from the lateral intermuscular septum
- Ligate each perforator as encountered
- Subperiosteal exposure of the anterolateral femur
- Apply a long plate with three bicortical screws above and below
Extensions and closure
- Proximal: Watson-Jones interval to the greater trochanter
- Distal: lateral femoral condyle for supracondylar access
- Close the fascia lata securely to prevent herniation
- Subcutaneous and skin closure
- Touch weight bearing 6 to 12 weeks with early knee ROM
References
The anterolateral approach is the standard exposure for open plating of femoral shaft fractures when intramedullary nailing is contraindicated. Systematic perforator ligation reduces bleeding complications, and outcomes are excellent with anatomic reduction and stable fixation: anatomic reduction with less than 5 degrees of angulation and less than 1 cm shortening yields greater than 90 percent good-to-excellent results, nonunion rates fall below 5 percent when bone grafting is used for atrophic nonunions, and knee stiffness is minimised by early motion. Guidelines, registries and global practice. The approach is used worldwide for plate fixation when intramedullary nailing is not feasible, and the principles are consistent across contemporary practice and other examination systems. AO Foundation recommends anatomic reduction and stable fixation for femoral shaft fractures when plating is chosen; BOA and BOAST guidance emphasises soft-tissue handling and early mobilisation; and OTA and AAOS stress restoration of length, alignment and rotation. Femoral shaft fractures have a population incidence of approximately 10 to 15 per 100,000 per year, and plate fixation shows greater than 90 percent union when anatomic reduction is achieved. In high-resource settings locking plates and minimally invasive techniques are common, while in resource-limited settings standard compression plates and open techniques remain effective when the same principles of reduction, perforator control and stable fixation are followed. Informed consent (globally applicable) should cover bleeding from perforators, infection (1 to 3 percent), nonunion (5 to 10 percent), malunion, knee stiffness and the need for protected weight bearing for 6 to 12 weeks.
Plate Fixation of Femoral Shaft Fractures: Long-term Results
- Large series of femoral shaft fractures treated with open plating via the anterolateral approach
- Anatomic reduction and stable fixation achieved in greater than 90 percent of cases with low complication rates
- Anterior bone grafting recommended for comminuted or atrophic patterns
Perforating Arteries of the Thigh: Surgical Anatomy
- Detailed cadaveric study mapping the perforating branches of the profunda femoris as they pierce the lateral intermuscular septum
- Demonstrated a consistent location of four to six perforators along the femoral shaft
- Recommended systematic ligation during elevation of vastus lateralis to reduce bleeding complications
Fractures of the femur treated by femoral plating using the anterolateral approach
- Early clinical series demonstrating successful femoral shaft plating via the anterolateral approach with good functional outcomes
Minimally invasive plate osteosynthesis: femoral blood supply
- Percutaneous plating via the anterolateral approach disrupts femoral blood supply less than traditional open techniques