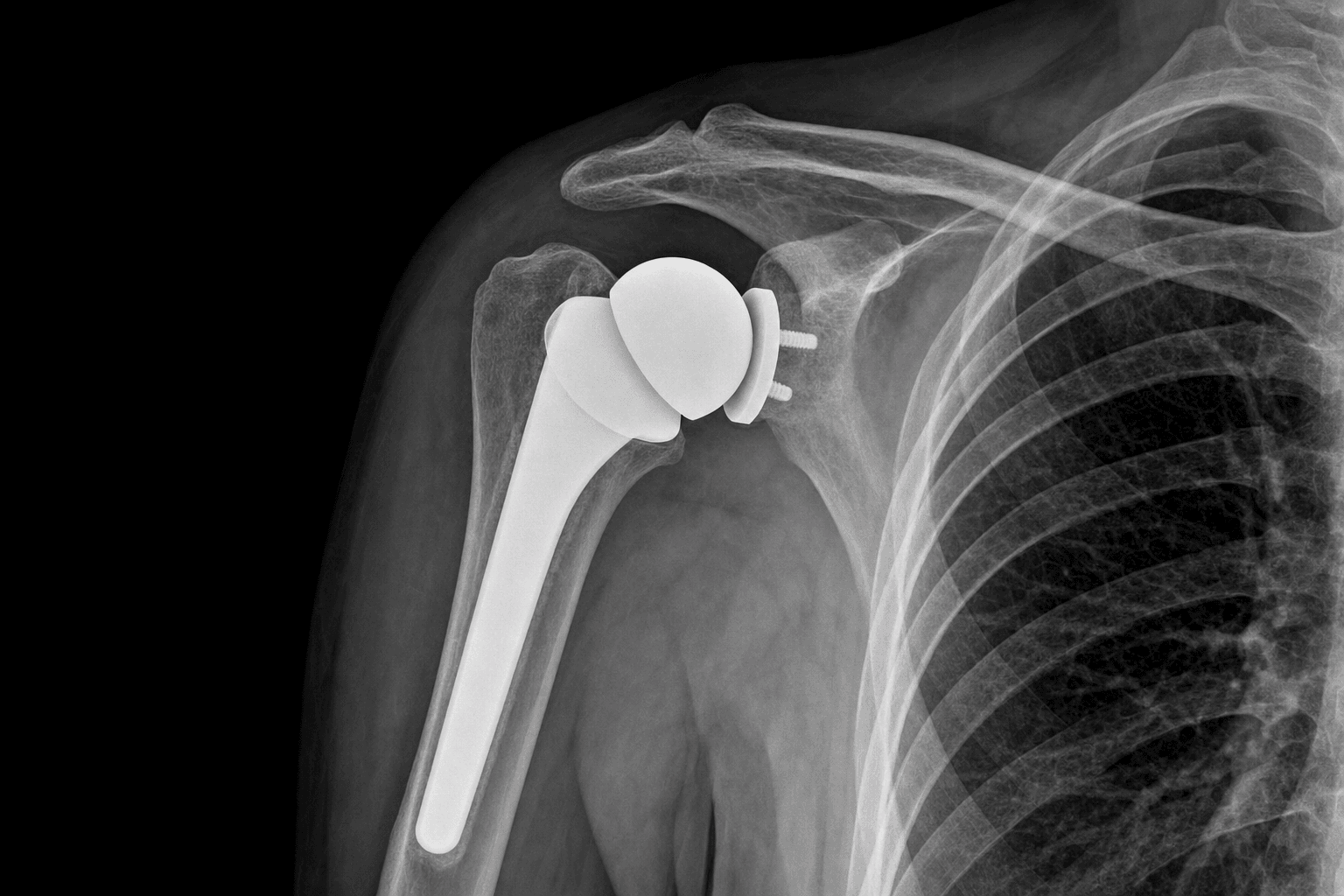
Glenohumeral osteoarthritis with an intact rotator cuff · deltopectoral approach
- Primary indication: glenohumeral osteoarthritis with an INTACT, repairable rotator cuff. Cuff status is the single factor that decides anatomic versus reverse TSA — an irreparable cuff means a reverse.
- The Walch glenoid classification (A1/A2 concentric, B1/B2/B3 posterior subluxation, C dysplastic) drives glenoid preparation. Correct version to neutral or up to 10 degrees retroversion — never more, or posterior loosening is accelerated.
- Subscapularis management: the lesser tuberosity osteotomy is widely preferred for bone-to-bone healing, but the best comparative evidence (Louie et al. systematic review, 1420 shoulders) shows outcomes similar to tenotomy. A secure repair is what matters; its failure causes anterior instability.
- Glenoid component: cemented all-polyethylene pegged is the global default (broadly 90-95% 10-year revision-free survival across registries). Metal-backed components fail substantially more (around 75-85% at 10 years) and are avoided in primary TSA.
- Through the deltopectoral internervous interval, protect the cephalic vein, the axillary nerve (5-7mm below the inferior glenoid rim) and the musculocutaneous nerve (never retract medial to the conjoint tendon).
- Distinguish revision survivorship (high) from radiographic loosening (common — around a third of glenoids are radiographically loose at 10-15 years). Examiners reward candidates who separate these two end-points.
When & Why
Indication. Anatomic total shoulder arthroplasty (TSA) replaces the arthritic humeral head with a stemmed component and resurfaces the glenoid, relying on a functioning rotator cuff for stability and movement. The primary indication is glenohumeral osteoarthritis with an intact, repairable rotator cuff that has failed non-operative care. Other accepted indications, all with the cuff still functional, include inflammatory arthritis (rheumatoid, seronegative arthropathies), post-traumatic arthritis with preserved bone stock, and humeral head avascular necrosis (steroids, alcohol, sickle cell) with secondary arthritis. Assess the cuff and the glenoid before committing. Rotator cuff integrity is the deciding factor between anatomic and reverse TSA, and glenoid morphology (the Walch classification) dictates how the glenoid is prepared. Exclude or plan for:
- Rotator cuff tear arthropathy — an irreparable cuff is a contraindication to anatomic TSA; a reverse TSA is used instead.
- Severe glenoid bone loss (vault less than 15mm after reaming), active infection, deltoid dysfunction, or a patient who cannot comply with rehabilitation — all contraindications.
- Glenoid version and posterior erosion (Walch B2/B3) on a preoperative CT — these demand version-correcting strategies, not standard concentric reaming. The one decision that matters. Where the cuff is intact an anatomic TSA restores native anatomy; where it is irreparable a reverse TSA is preferred; in a young patient with avascular necrosis and a pristine glenoid, a hemiarthroplasty may suffice. The choice is driven by the cuff, the glenoid and the patient.
Intact, repairable cuff. Restores native geometry and relies on the cuff for stability. Best pain relief and satisfaction in primary OA — but the cuff must last.
Irreparable rotator cuff, cuff-tear arthropathy, or severe glenoid bone loss. The glenosphere and humeral cup provide a semi-constrained, cuff-independent lever arm.
Selected young patients with humeral head avascular necrosis and a pristine glenoid. The glenoid is not resurfaced, so glenoid arthritis can progress — less favoured when the glenoid is diseased.
Consent specifically for instability (predominantly anterior, linked to subscapularis failure), stiffness, glenoid component loosening, nerve injury (axillary and musculocutaneous), infection, and a lifelong restriction on repetitive heavy overhead lifting for component longevity. Setup. Beach-chair position 30-45 degrees upright, the head secured in a Mayfield or horseshoe headrest to prevent intraoperative movement, and a bump under the medial scapula to improve posterior glenoid exposure. The arm is free-draped for full mobility. General anaesthesia with controlled hypotension reduces bleeding and improves visualisation; an interscalene block provides postoperative analgesia (caution: phrenic nerve palsy in around 5%, so avoid bilateral blocks). Cefazolin 2g IV is given within 60 minutes of incision (vancomycin 15mg/kg if penicillin-allergic or MRSA risk), redosed every 4 hours, and continued for 24 hours.
The Operation
The goal: expose the shoulder through the deltopectoral internervous interval, take down the subscapularis, release the capsule and dislocate the humeral head atraumatically, then prepare and implant the glenoid and humeral components, restore soft-tissue tension, and repair the subscapularis securely. The exposure is laid out in full below (and in depth on the deltopectoral approach to the shoulder page). Critical anatomy in the field. The deltopectoral interval is a true internervous plane between deltoid (axillary nerve, C5-C6) and pectoralis major (medial and lateral pectoral nerves, C5-T1) — no muscle is divided, so denervation risk is minimal. The cephalic vein runs in the fatty triangle between them and is the landmark for the interval. The subscapularis (upper and lower subscapular nerves, C5-C6) is the primary internal rotator and the key anterior stabiliser; it inserts on the lesser tuberosity and must be taken down and repaired. The axillary nerve crosses the inferior capsule 5-7mm below the inferior glenoid rim and is the structure most at risk, while the musculocutaneous nerve enters the conjoint tendon 3-8cm distal to the coracoid.
Operative sequence
- Beach chair 30-45 degrees, bump under the medial scapula, arm free-draped; mark the coracoid tip, the deltopectoral groove and the anterior axillary crease before incising.
- A curvilinear incision 12-15cm from the coracoid to the deltoid insertion: start 2cm lateral and 2cm inferior to the coracoid tip and curve distally along the deltopectoral groove to end 4cm distal to the anterior axillary crease.
- 12cm minimum for an average primary; 15cm for a muscular or revision case — too short an incision causes soft-tissue trauma and poor glenoid visualisation from forced retraction.
- Develop subcutaneous flaps sharply to expose the deltopectoral interval and identify the cephalic vein in the fatty triangle (variable — bifurcates in 15%, large tributaries in 30%).
- Retract the vein laterally with deltoid in most cases (or medially with pectoralis if its tributaries favour that). If injured, ligate proximal and distal with suture — diathermy alone often fails postoperatively.
- Separate deltoid from pectoralis major by blunt finger dissection. This is a true internervous plane (axillary versus pectoral nerves) — stay superficial and do not dive deep too early.
- Palpate the firm strap-like conjoint tendon (coracobrachialis and short head of biceps) medially and retract it medially as a unit.
- Never place a retractor medial to the conjoint tendon — the musculocutaneous nerve enters it 3-8cm distal to the coracoid (mean 5.5cm) and is injured by medial retraction.
- Release the lateral 2-3cm of the pectoralis major insertion only if exposure is limited (revision, very stiff shoulders); tag it for repair.
- Three options: lesser tuberosity osteotomy (commonly preferred — a 5-7mm bone wafer taken with an oscillating saw parallel to the articular surface, tagged with three #5 nonabsorbable sutures through drill holes), a tendon peel (5mm lateral to the insertion), or a tenotomy at the tendon-muscle junction for maximal mobilisation.
- Whichever is chosen, the security of the later repair matters more than the technique — the Louie et al. systematic review found similar complication and revision rates between osteotomy and tenotomy.
- Subscapularis failure after TSA is devastating: it causes anterior instability, recurrent dislocation and poor function, often requiring conversion to a reverse.
- Release the capsule circumferentially: superior (rotator interval and coracohumeral ligament), anterior (with the subscapularis), posterior (electrocautery capsulotomy), and — most critically — inferior.
- The inferior release (3-6 o'clock on the glenoid) is the step most often inadequate. Use a curved osteotome and stay on bone to avoid the axillary nerve 5-7mm below the inferior glenoid rim.
- A complete release lets the humeral head dislocate anteriorly with minimal force; if dislocation is difficult, reassess the inferior release before forcing.
- Gentle longitudinal traction, then 20-30 degrees of external rotation and extension to deliver the head anterior to the glenoid.
- Never force dislocation — it risks an iatrogenic humeral shaft fracture (1-3% in osteoporotic or post-fracture bone), greater tuberosity avulsion, or rotator cuff tear.
- If it will not deliver, complete the inferior and posterior capsular release first; a bone hook on the posterior humeral neck can help lever the head gently.
- With a Fukuda (or similar) retractor behind the humerus and Hohmann retractors on the glenoid rim, inspect the glenoid face.
- Determine the Walch type, version (normal 2-7 degrees retroversion) and bone loss using the preoperative CT — essential for B2/B3 glenoids (greater than 15 degrees retroversion or greater than 10mm posterior bone loss).
- A B2 glenoid needs eccentric (high-side) reaming, an augmented component, or bone grafting; standard concentric reaming over-medialises and accelerates failure.
- Remove all peripheral osteophytes to expose the true anatomic neck, then apply the cutting guide using the bicipital groove (20-30 degrees retroversion), the medullary canal axis (130-140 degrees to the shaft) and templated height.
- Execute the osteotomy with an oscillating saw at 130-140 degrees to the shaft in 20-30 degrees retroversion (reference the forearm with the elbow flexed 90 degrees).
- Osteotomy height is critical: too proud overstuffs the joint (pain, stiffness, accelerated loosening); too low causes instability. When unsure, err slightly low — it is easier to add head height than to remove bone.
- Find the canal axis with a canal finder, then ream sequentially (typically 6mm up to 10-14mm) until cortical chatter — stop at firm engagement.
- Use hand reamers for tactile control, especially in osteoporotic bone. Ream to 10-15cm maximum — the radial nerve spirals around the humerus 14-20cm distal to the acromion.
- Size for proximal metaphyseal fill (press-fit stems) or distal cortical preparation (cemented stems); have multiple stem sizes available as canal diameter varies (8-16mm).
- Ream concentrically, perpendicular to the glenoid face (not the scapular body), progressing until all cartilage is removed and uniform bleeding cancellous bone shows. Correct version toward neutral or up to 10 degrees retroversion.
- For B2/B3 glenoids, use eccentric (high-side anterosuperior) reaming — it can correct up to 15 degrees but risks vault perforation if excessive.
- Drill the central peg/keel and peripheral peg holes with the component-specific guide, perpendicular to the glenoid face. Vault depth averages 25-30mm (range 15-40mm) — use a depth gauge and check the CT before drilling to avoid perforating toward the brachial plexus and axillary vessels (2-3cm medial).
- Pulse-lavage and dry the glenoid completely; fill the peg/keel holes with dough-phase low-viscosity cement and pressurise.
- Insert an all-polyethylene component (pegged preferred over keeled) perpendicular to the face, maintain pressure until fully seated, and remove excess cement meticulously (especially posteriorly).
- Maintain impactor pressure until the cement hardens (8-10 minutes). Pressurisation drives cement interdigitation and lowers early loosening — radiolucent lines greater than 2mm, or progressive lines, signal concern.
- Reduce a trial stem and head (typically 38-52mm). Check head coverage of the osteotomy (greater than 70%), soft-tissue tension (moderate resistance, humeral head translates 25-50% of the glenoid diameter), and stability through a full arc (forward elevation 150 degrees, external rotation 40 degrees, internal rotation to L3).
- If too tight (overstuffed), downsize the head or recheck the osteotomy level; if unstable, consider a larger head, more offset, or recheck the soft tissues.
- Insert the final stem — press-fit metaphyseal in good bone, cemented in osteoporotic or inflammatory bone — maintaining version (reference the bicipital groove and forearm throughout).
- For a lesser tuberosity osteotomy: reduce the fragment anatomically, drill three 2mm tunnels in the humeral shaft exiting laterally 2-3cm distal to the osteotomy, pass #2 or #5 nonabsorbable sutures, and tie them with the arm in 30 degrees internal rotation — a 6-point repair.
- For a peel or tenotomy: repair tendon to bone with suture anchors or bone tunnels, side-to-side if tissue allows, arm in 30 degrees internal rotation.
- Repair strength sets the rehabilitation pace: a secure osteotomy allows passive ROM early and active motion around 4 weeks; less secure repairs need 6 weeks of passive-only motion with no internal-rotation strengthening until 12 weeks.
- Repair the rotator interval if it was released (not routine). Never suture the deltopectoral interval closed — it causes compartment syndrome and deltoid denervation; let the tissue planes appose naturally.
- Repair the pectoralis major if more than half was released (transosseous sutures or bone tunnels). Layered closure: subcutaneous 2-0 absorbable, subcuticular 3-0 monofilament. Apply a sterile dressing and a sling with the arm in neutral rotation.
- Where it lies
- Crosses the inferior capsule 5-7mm below the inferior glenoid rim, then runs on the deep surface of deltoid
- How to protect it
- Stay on bone with a curved osteotome during inferior capsular release; never force dislocation; limit inferior retraction to less than 1cm
- Where it lies
- Enters the conjoint tendon 3-8cm distal to the coracoid (mean 5.5cm)
- How to protect it
- Never place a retractor medial to the conjoint tendon; retract the conjoint as a unit; limit continuous medial retraction to less than 90 minutes
- Where it lies
- Runs in the fatty deltopectoral triangle; bifurcates in 15%, large tributaries in 30%
- How to protect it
- Identify early and retract laterally with deltoid; if injured, ligate proximal and distal with suture, not diathermy alone
- Where it lies
- 2-3cm medial to the glenoid face, deep to the field
- How to protect it
- Use a depth gauge before glenoid drilling; check the CT for vault depth (average 25-30mm); never retract medial to the conjoint
- Where it lies
- Spirals around the posterior humeral shaft 14-20cm distal to the acromion
- How to protect it
- Limit humeral reaming to 10-15cm depth; avoid lateral retractors on the distal humerus
The axillary nerve lies only 5-7mm below the inferior glenoid rim and is at risk during the inferior capsular release, during humeral dislocation, and from inferior retraction. Stay on bone with a curved osteotome, never force dislocation, and limit inferior retraction to less than 1cm. If the nerve is injured it is usually a neuropraxia that recovers in 3-6 months (85-90%), but document the deficit immediately and obtain a baseline EMG at 3-4 weeks.
The brachial plexus and axillary vessels lie 2-3cm medial to the glenoid face. Vault perforation during peg-hole drilling is catastrophic. Always check the preoperative CT for vault depth (average 25-30mm, range 15-40mm), use a depth gauge before drilling, and reduce depth or omit the posterior peg in a B2/B3 glenoid with posterior bone loss.
Correct glenoid version to neutral or up to 10 degrees retroversion. Greater than 10 degrees in the final position accelerates posterior eccentric loading and loosening. Eccentric (high-side anterosuperior) reaming can correct up to 15 degrees if the vault is adequate; beyond that, use an augmented component, bone graft, or — if the cuff is questionable — a reverse TSA. Never accept excessive retroversion as close enough.
A cemented all-polyethylene pegged glenoid is the gold standard — broadly 90-95% 10-year revision-free survival across registries. Dry bone, dough-phase cement, pressurisation into the peg holes, and maintaining pressure until set are what give durable fixation. Metal-backed components are substantially worse and are avoided in primary TSA. Remember that radiographic loosening is far more common than revision (around a third of glenoids at 10-15 years).
Closing the deltopectoral interval is a cardinal error — it causes compartment syndrome and deltoid denervation. Let the tissue planes appose naturally. Meticulous haemostasis and layered skin closure are superior to a drain, which is not routine in primary surgery.
Aftercare & Complications
Rehabilitation The protocol is paced to the security of the subscapularis repair — a secure lesser tuberosity osteotomy moves faster than a peel or tenotomy. | Phase | Timing | Immobilisation | Therapy | |-------|--------|-----------------|---------| | 1 | 0-4 weeks (osteotomy) or 0-6 weeks (peel/tenotomy) | Sling; remove for hygiene; sleep in sling | Passive ROM only — pendulums, therapist-assisted elevation and ER; no active motion (no active IR for a peel/tenotomy) | | 2 | 4-6 weeks / 6-12 weeks | Sling for comfort | Active-assisted ROM with stick or pulley; gradual progression | | 3 | 6-12 weeks / 12-18 weeks | Wean sling | Active ROM; gentle strengthening with resistance bands from 0.5kg | | 4 | 12-24 weeks | — | Progressive strengthening; return to swimming or golf from 4-6 months | Most patients return to desk work by 6-8 weeks. Lifelong restriction on repetitive heavy overhead lifting (greater than 25 pounds) protects component longevity. Low-impact activities (swimming, golf, cycling) are encouraged; high-impact and contact activities are discouraged. Follow-up at 2 weeks (wound), 6 and 12 weeks (radiographs and therapy progress), 6 and 12 months, then annually, monitoring for radiolucent lines (greater than 2mm or progressive is concerning), subsidence, osteolysis and heterotopic bone. Complications
- Recognition
- Early (less than 3 months): drainage, fever, pain; late: insidious pain, stiffness, loosening, raised CRP. Aspiration WBC greater than 3,000 with greater than 80% PMNs and positive culture
- Prevention
- Cefazolin 2g IV within 60 min and redose q4h; optimise HbA1c less than 7% and albumin greater than 3.5; meticulous haemostasis and minimal theatre traffic
- Management
- Early with stable components: DAIR plus 6 weeks IV antibiotics (success 55-70%). Late or loose: two-stage revision. Uncontrolled: resection arthroplasty as salvage
- Recognition
- Anterior (90%): subscapularis failure or excessive humeral retroversion, positive belly-press and lift-off; posterior (10%): excessive anteversion or posterior glenoid erosion
- Prevention
- Secure subscapularis repair; correct version (humeral 20-30 degrees retroversion, glenoid neutral to 10 degrees); appropriate tensioning; 6 weeks sling protection
- Management
- Early (less than 6 weeks): closed reduction and immobilisation. Recurrent anterior: MRI the subscapularis, revise or reconstruct, or convert to RSA if irreparable. Recurrent posterior: revise version or convert to RSA
- Recognition
- Activity-related pain, mechanical clicking; radiolucent lines greater than 2mm or progressive, component tilt, osteolysis on serial films and CT
- Prevention
- Neutral to 10 degrees retroversion, no superior inclination; pressurised cementing; all-polyethylene pegged component; address B2/B3 bone loss preoperatively
- Management
- Asymptomatic: observe. Symptomatic with good bone: revise the glenoid. Poor bone: hemiarthroplasty or convert to RSA. Severe loss: structural graft plus revision
- Recognition
- Immediate postoperative deficit — deltoid (axillary), biceps (musculocutaneous), wrist extension (radial); EMG/NCS at 3-4 weeks
- Prevention
- Identify and protect neurovascular structures; stay on bone during inferior release; never retract medial to the conjoint; limit retraction time
- Management
- Most neuropraxias recover 3-6 months (85-90%); physiotherapy to prevent contracture; baseline EMG then repeat at 3 months; explore only for suspected laceration, compressing haematoma, or no recovery at 6-9 months
- Recognition
- Greater tuberosity during dislocation; humeral shaft during canal preparation or stem insertion; crack heard or abnormal stem seating
- Prevention
- Gentle dislocation after adequate release; hand reamers in poor bone; appropriate stem size; prophylactic cerclage in very osteoporotic bone (T-score less than -3.0)
- Management
- Undisplaced metaphyseal: cerclage and proceed. Displaced shaft: ORIF with plate and cerclage plus a long-stem cemented prosthesis bypassing the fracture by 2 cortical diameters. Vault perforation: abandon the glenoid component (hemiarthroplasty)
- Recognition
- ROM less than 90 degrees elevation or less than 10 degrees ER at 6-12 weeks; worse in diabetics
- Prevention
- Avoid overstuffing (trial components); early passive ROM within pain tolerance; structured physiotherapy; glycaemic control
- Management
- Progressive stretching physiotherapy; pain control; manipulation under anaesthesia at 3-4 months if severe and static; reassess for component malposition, infection or heterotopic bone
- Recognition
- Progressive stiffness 2-6 months postop with a firm end-feel; periarticular bone on radiograph
- Prevention
- Gentle tissue handling; indomethacin 75mg daily for 6 weeks or single-dose radiation 7-8Gy within 72 hours in high-risk patients (male, previous HO, DISH)
- Management
- If not limiting function: observe. Severe and limiting: excise after maturation (12-18 months) with preoperative CT and prophylaxis to prevent recurrence
- Recognition
- Subscapularis: anterior instability, weak IR, positive belly-press/lift-off; superior cuff: weakness, drop-arm, pseudoparalysis, acromiohumeral distance less than 7mm
- Prevention
- Secure subscapularis repair; avoid overstuffing; preserve cuff attachments; gradual ROM; protect the repair 6 weeks
- Management
- Subscapularis with instability: revise or reconstruct (Achilles allograft), or convert to RSA if irreparable. Superior cuff failure with pseudoparalysis: convert to RSA
Viva & Exam Focus
GLENOIDGLENOID positioning principles
SUBSCAPSUBSCAP repair principles (lesser tuberosity osteotomy)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old has shoulder pain and stiffness. Radiographs show glenohumeral arthritis with posterior glenoid erosion and humeral head subluxation; CT shows 18 degrees retroversion. How do you manage this and what are the technical challenges?”
“Six months after anatomic TSA a patient has anterior shoulder pain and recurrent subluxation on overhead activity, with positive belly-press and lift-off tests. What is your differential and management?”
“Describe your technique for subscapularis management in anatomic TSA. Compare the three approaches and justify your preference with evidence.”
Indications
- Primary indication: glenohumeral OA with an INTACT, repairable rotator cuff (cuff integrity decides anatomic versus reverse)
- Inflammatory arthritis, post-traumatic arthritis, and humeral head AVN — all with the cuff intact
- Contraindications: cuff-tear arthropathy (use reverse), active infection, vault less than 15mm, deltoid dysfunction, non-compliance
Key anatomy
- Deltopectoral interval: internervous (axillary versus pectoral nerves), cephalic vein the landmark
- Axillary nerve: 5-7mm below the inferior glenoid rim — at risk during inferior capsular release
- Musculocutaneous nerve: enters the conjoint 3-8cm from the coracoid — never retract medial to the conjoint
- Subscapularis: internal rotator and anterior stabiliser on the lesser tuberosity — failure causes instability
- Glenoid vault: 25-30mm average (15-40mm); plexus and axillary vessels 2-3cm medial to the face
Critical steps
- Deltopectoral approach, protect the cephalic vein, blunt interval development
- Subscapularis take-down — LTO preferred (5-7mm wafer, three #5 sutures); secure repair matters more than the technique
- 360-degree capsular release (inferior is critical, stay on bone) then atraumatic dislocation
- Glenoid: Walch-based planning, concentric reaming, version to neutral to 10 degrees retroversion, all-polyethylene pegged component with pressurised cement
- Humeral osteotomy 130-140 degrees to shaft, 20-30 degrees retroversion; canal to 10-15cm
- Subscapularis repair: 6-point through bone tunnels, arm in 30 degrees IR, 6 weeks sling
Danger zones
- Axillary nerve: 5-7mm inferior to the glenoid — stay on bone, never force dislocation, limit inferior retraction to less than 1cm
- Musculocutaneous nerve: never retract medial to the conjoint; limit medial retraction to less than 90 minutes
- Brachial plexus and axillary vessels: depth gauge and CT before glenoid drilling
- Cephalic vein: retract laterally; ligate with suture if injured
- Radial nerve: limit humeral reaming to 10-15cm
Technique pearls
- Subscapularis: LTO widely favoured but the Louie systematic review shows outcomes similar to tenotomy
- Walch: A1/A2 standard reaming; B1/B2 eccentric reaming or augments; B3 often bone graft; C consider reverse
- Glenoid version neutral to 10 degrees retroversion maximum — greater than 10 degrees accelerates loosening
- Component: cemented all-polyethylene pegged glenoid best survival (90-95% at 10 years); avoid metal-backed; press-fit humeral stem in good bone, cemented in osteoporosis
- Soft-tissue tension: moderate resistance, translate 25-50% of glenoid diameter; overstuffing causes pain, stiffness and loosening
Complications
- Infection 0.5-2%: DAIR success 55-70% early; two-stage revision late; optimise HbA1c and albumin
- Instability 1-3% (5-10% with subscapularis failure): anterior most common; revise or convert to RSA
- Glenoid loosening 2-4% at 10 years: from malposition or inadequate cementing; radiolucent lines greater than 2mm concerning
- Nerve injury 1-4% temporary, less than 1% permanent: axillary most common; most recover 3-6 months
- Intraoperative fracture 1-3% primary, 5-10% revision: cerclage and long stem if displaced
Post-op protocol
- Sling 4 weeks (secure LTO) or 6 weeks (peel/tenotomy)
- LTO: passive 0-4 weeks, active-assisted 4-6, active 6-12, strengthening 12-24
- Peel/tenotomy: passive 0-6, active-assisted 6-12, active 12-18, strengthening 18-24
- No repetitive overhead lifting greater than 25 pounds lifelong
- Follow-up 2, 6, 12 weeks then 6 and 12 months and annually; radiolucent lines greater than 2mm concerning
Exam tips
- Know anatomic versus reverse versus hemiarthroplasty: cuff integrity drives the choice
- Walch in detail: identify on imaging, give a management strategy for B2/B3, never accept greater than 10 degrees retroversion
- Subscapularis management is an examiner favourite: compare LTO, peel and tenotomy; know the Louie systematic review
- Component positioning: glenoid neutral to 10 degrees retroversion, humeral 20-30 degrees retroversion
- Registry themes: all-poly glenoid 90-95% 10-year survival; younger patients revise more; radiographic loosening far exceeds revision (around a third at 10-15 years)
Background & Evidence
Epidemiology and outcomes. Anatomic TSA is performed for glenohumeral arthritis with an intact, repairable rotator cuff, and primary osteoarthritis is the commonest indication — it also gives the most durable result. Inflammatory arthropathies do worse, driven largely by late rotator cuff failure (Khan et al.: up to 75% cuff failure at 10 years in rheumatoid arthritis) rather than glenoid loosening alone. Around 95% of well-selected patients achieve significant pain relief and 85-90% are satisfied in primary OA with an intact cuff; forward elevation typically improves by 40-60 degrees and function plateaus at 12-18 months. Younger, higher-demand patients have consistently higher revision rates across registries. The commonest reasons for revision are glenoid loosening, instability (predominantly anterior, linked to subscapularis failure) and infection. Biomechanics. Anatomic TSA is unconstrained — stability relies on the rotator cuff, capsule and component conformity (concavity-compression), which is why cuff integrity is essential. Eccentric loading generates a rocking-horse moment on the glenoid: maximum forces reach 2-3 times body weight during elevation, oriented superiorly and posteriorly, driving cement-bone micromotion and loosening. Excessive retroversion increases posterior eccentric load. Overstuffing (oversized head or proud osteotomy) causes pain, stiffness and accelerated loosening; understuffing causes instability. Pathoanatomy and the Walch classification. Posterior humeral head subluxation in primary OA drives asymmetric posterior glenoid wear — the basis of the Walch classification, which governs glenoid preparation.
- Morphology
- Concentric, centred head, minor central erosion, less than 10 degrees retroversion
- Management
- Standard concentric reaming; all-polyethylene component; excellent outcomes
- Morphology
- Centred head, major central erosion, maintained version
- Management
- Deeper reaming to a flat surface; watch for medialisation
- Morphology
- Narrowed posterior joint space, biconcave, less than 70% posterior subluxation, 10-15 degrees retroversion
- Management
- Eccentric (high-side) reaming to neutral or 5 degrees retroversion
- Morphology
- Biconcave, greater than 70% posterior subluxation, 10-20 degrees retroversion
- Management
- Eccentric reaming if vault adequate; posterior augment or bone graft if not
- Morphology
- Monoconcave posterior defect, greater than 25 degrees retroversion
- Management
- Often needs posterior bone graft or an augment; consider reverse TSA if cuff questionable
- Morphology
- Dysplastic, greater than 25 degrees retroversion
- Management
- Complex reconstruction; anatomic outcomes inferior, consider reverse TSA
Component choice. On the glenoid side, a cemented all-polyethylene pegged component is the global default; the alternatives are reserved or avoided:
Gold standard. Best long-term survival across registries (broadly 90-95% at 10 years). Central peg plus peripheral pegs, pressurised cement.
Traditional single central keel with simpler instrumentation, but slightly higher loosening than pegged in some registries.
Avoid in primary TSA. Boileau RCT found 20% loosening versus 0% all-polyethylene, with osteolysis and insert dissociation.
For Walch B2/B3 posterior bone loss; corrects version without excessive reaming. Limited long-term data, and some designs are metal-backed.
On the humeral side, a press-fit metaphyseal stem is the modern trend in good bone quality (bone-preserving, easier revision), a cemented stem is preferred in osteoporotic or inflammatory bone and for older smooth stems, and a stemless component maximally preserves bone in carefully selected good-quality, non-dysplastic bone. Subscapularis management. The three take-down techniques differ in the healing interface and mobilisation they offer, but the best comparative evidence does not establish one as superior — a secure repair and protected rehabilitation matter more than the specific method.
- Technique
- 5-7mm bone wafer with an oscillating saw parallel to the articular surface; three #5 nonabsorbable sutures through drill holes; repaired through shaft tunnels in 30 degrees IR (6-point)
- Advantages
- Bone-to-bone healing; anatomic re-attachment; may allow earlier mobilisation where fixation is secure
- Disadvantages
- Technically more demanding; risk of tuberosity fracture or nonunion
- Technique
- Release 5mm lateral to the lesser tuberosity insertion sharply; tag with sutures; repair to bone with anchors or tunnels
- Advantages
- Preserves bone stock; familiar; no tuberosity fracture risk
- Disadvantages
- Tendon-to-bone healing; harder to restore anatomic length
- Technique
- Divide at the tendon-muscle junction 2-3cm medial to insertion; side-to-side repair
- Advantages
- Maximal mobilisation (useful in stiff or revision shoulders); fastest release
- Disadvantages
- Tendon-to-tendon healing; harder to restore length; historically linked to internal-rotation weakness
Registry survivorship and key studies. Across the National Joint Registry (UK), AJRR (US), AOANJRR (Australia), SHAR (Sweden) and NZJR (New Zealand), a cemented all-polyethylene glenoid gives broadly 90-95% 10-year revision-free survival, while metal-backed designs are substantially worse and avoided. The pivotal nuance is that revision survivorship is high but radiographic loosening is common: Raiss et al. found 36% of glenoids radiographically loose and only 48% survivorship at 13 years using radiographic loosening, despite 100% revision-free survival. Walch et al. defined the glenoid morphology classification (A 59%, B 32%, C 9%); Boileau et al. (RCT) showed 20% metal-backed loosening versus 0% all-polyethylene and abandoned the metal-backed design; Louie et al. (systematic review) showed subscapularis tenotomy and osteotomy have similar outcomes. These are summarised in the references below.
References
Morphologic study of the glenoid in primary glenohumeral osteoarthritis
- CT review of 113 osteoarthritic shoulders defined three glenoid types: A (concentric) 59%, B (posterior subluxation) 32%, C (dysplastic, retroversion greater than 25 degrees) 9%
- Posterior humeral-head subluxation drives asymmetric posterior wear in Type B glenoids
- Type C retroversion is primarily dysplastic in origin and associated with early-onset osteoarthritis
Cemented polyethylene versus uncemented metal-backed glenoid components in total shoulder arthroplasty: a prospective, double-blind, randomized study
- 40 shoulders randomised; metal-backed glenoid loosening 20% versus 0% for cemented all-polyethylene at minimum 3 years (P less than 0.001)
- Four revisions in the metal-backed group versus none in the all-polyethylene group (P = 0.02), with severe osteolysis and metal-on-metal wear
- All-polyethylene radiolucent lines were frequent (85%) but largely non-progressive and did not correlate with function
Subscapularis tenotomy versus lesser tuberosity osteotomy for total shoulder arthroplasty: a systematic review
- PRISMA systematic review of 20 studies (1420 shoulders) comparing subscapularis tenotomy and lesser tuberosity osteotomy
- Both techniques produced excellent outcomes; complication rates were almost identical, with a non-significant trend toward fewer revisions after tenotomy (10.0% vs 16.2%)
- No difference in Constant scores, pain scores or radiolucencies between approaches
Results of cemented total shoulder replacement with a minimum follow-up of ten years
- 39 third-generation cemented TSAs at mean 11 years: mean Constant score improved from 27 to 61 points
- 36% of glenoid components were radiographically loose; survivorship with radiographic loosening as the end-point was only 48% at 13 years despite 100% revision-free survival
- Cranial humeral migration (cuff insufficiency) seen in 69% of cases at 10-15 years
Clinical and radiological follow-up of the Aequalis third-generation cemented total shoulder replacement: a minimum ten-year study
- Minimum 10-year follow-up of a third-generation cemented total shoulder replacement
- Glenoid loosening and late rotator-cuff failure were the principal long-term problems
- Inflammatory arthropathy was associated with late cuff failure (up to 75% at 10 years in rheumatoid arthritis) rather than isolated glenoid loosening
Rupture of the subscapularis tendon after shoulder arthroplasty: diagnosis, treatment, and outcome
- Post-arthroplasty subscapularis rupture is associated with anterior instability and poorer outcomes
- Diagnosis rests on clinical signs (lift-off, belly-press) and imaging confirmation
- Management depends on tissue quality and ranges from repair to reconstruction, with variable outcomes
Complications of total shoulder arthroplasty
- Comprehensive review of complications after TSA: component loosening (glenoid greater than humeral) is the most frequently reported complication
- Glenoid loosening, instability, periprosthetic fracture, rotator-cuff tearing, neural injury and infection are the principal modes of failure
- Rotator-cuff failure and glenoid loosening are the leading long-term causes of unsatisfactory outcome