Antecubital Fossa | Lazy-S Incision | Brachial Artery and Median Nerve Protection
- Lazy-S or curved incision reduces skin contracture risk over the antecubital fossa; a straight transverse incision is avoided.
- Brachial artery lies centrally, deep to the bicipital aponeurosis - identify it early and protect it with a vessel loop.
- Median nerve lies immediately medial to the artery - the most commonly injured structure if it is not identified.
- Lateral antebrachial cutaneous nerve emerges lateral to the biceps tendon under the fascia - protect it to avoid permanent lateral forearm numbness.
- Radial nerve and PIN lie in the interval between brachialis and brachioradialis; the PIN sits immediately lateral and deep to the radial tuberosity.
When & Why
What it exposes. The anterior (antecubital) approach gives direct access to the antecubital fossa, the distal biceps tendon insertion, the anterior capsule and coronoid process, and the major neurovascular structures crossing the elbow - the brachial artery, median nerve, lateral antebrachial cutaneous nerve, and radial nerve with its posterior interosseous branch. It is the only approach that allows simultaneous visualisation of all of these. Why this approach. It is the distal continuation of the Henry approach to the arm and is the workhorse exposure for distal biceps tendon repair, anterior capsular release for post-traumatic or post-operative stiffness, and exploration of the brachial artery or median nerve. The lazy-S incision minimises the skin contracture that a straight transverse incision would produce across the flexion crease. Primary indications. - Distal biceps tendon rupture repair (acute and chronic).
- Anterior capsular release for post-traumatic or post-operative elbow stiffness.
- Exploration and repair of the brachial artery after injury.
- Median nerve exploration or decompression at the elbow.
- Coronoid process fracture fixation through anterior access.
- Radial nerve or PIN exploration in the proximal forearm. Contraindications. Active infection in the antecubital fossa; severe soft-tissue scarring from previous surgery or trauma (consider an extensile or alternative approach); isolated posterior pathology (use a posterior approach); patient factors precluding positioning or tourniquet use. Alternative approaches. - Posterior (Kocher or Bryan-Morrey): triceps, olecranon, posterior capsule.
- Medial: ulnar nerve, medial collateral ligament, medial coronoid.
- Lateral (Kocher): radial head, capitellum, lateral collateral ligament.
- Two-incision technique for distal biceps: reduces PIN risk but sacrifices anterior visualisation. Position and landmarks. Supine with the arm abducted on a hand table, the shoulder at the edge of the table, and the elbow slightly flexed (30 to 45 degrees) for the initial exposure. Apply a tourniquet high on the arm and inflate after exsanguination; minimise tourniquet time (ideally less than 120 minutes) and release for at least 20 minutes before any re-inflation. Fluoroscopy should be available. Palpable bony landmarks are the medial and lateral epicondyles, the radial head (rotating in the lateral fossa with forearm rotation), and the olecranon for orientation. The key soft-tissue landmark is the biceps tendon (a palpable cord when the elbow is flexed against resistance), with the bicipital aponeurosis felt as a tense band medial to it and the brachial artery pulse in the midline of the fossa. Plan a lazy-S incision: it begins 5 to 6 cm proximal to the elbow flexion crease on the medial border of the biceps, crosses the fossa in a gentle curve, and extends 5 to 6 cm distal to the crease over the brachioradialis-pronator interval on the lateral forearm - a total length of about 12 to 15 cm.
The Exposure
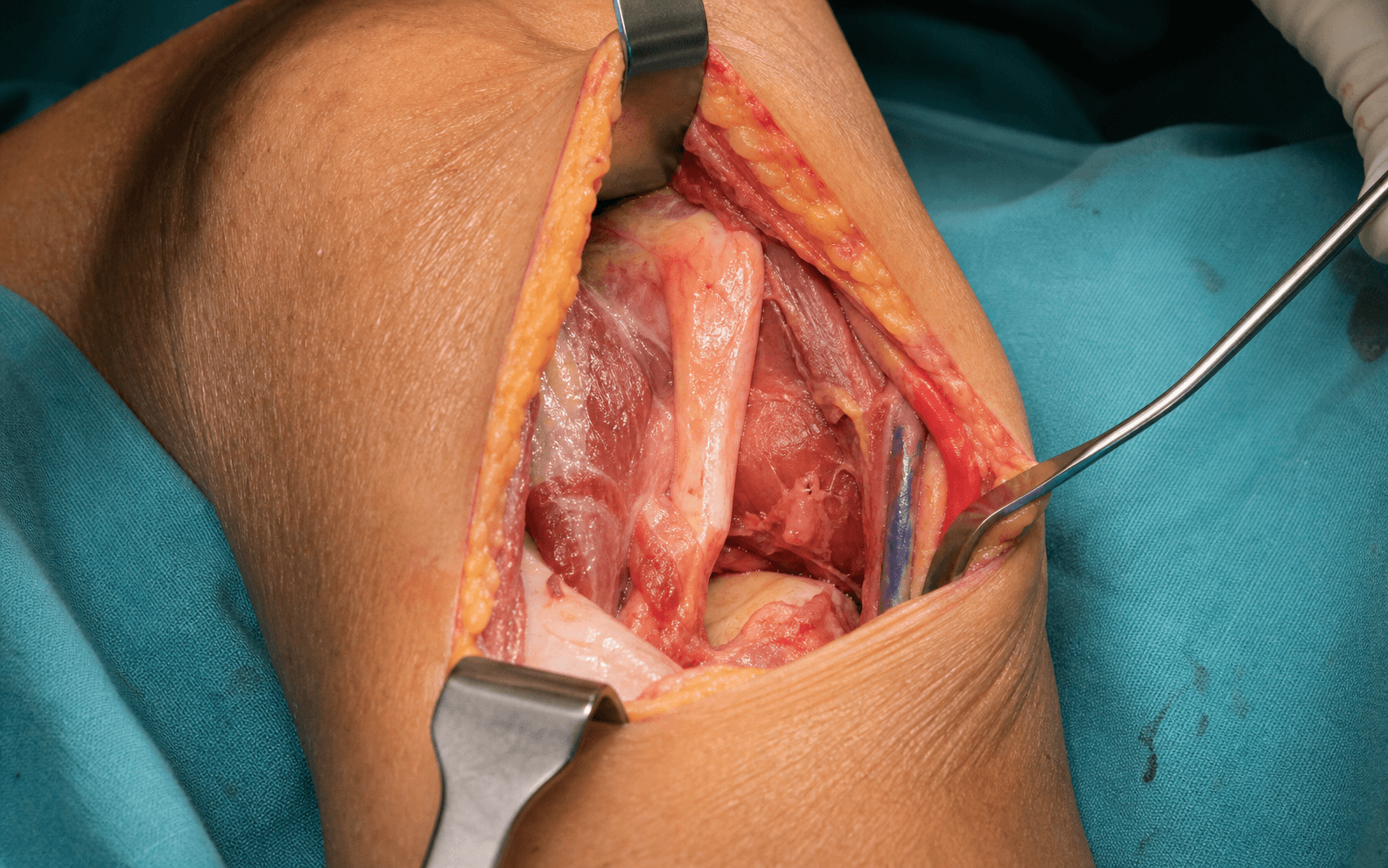
Work down through the layers across the antecubital fossa, identifying and protecting the cutaneous nerve first, then the central neurovascular bundle, and finally developing the brachialis-brachioradialis internervous plane to reach the capsule and the radial tuberosity.
Exposure sequence
- Begin 5 to 6 cm proximal to the elbow flexion crease on the medial border of the biceps, cross the antecubital fossa in a gentle curve from medial-proximal to lateral-distal, and extend 5 to 6 cm distal to the crease over the brachioradialis-pronator interval (total 12 to 15 cm).
- The lazy-S curve, centred on the flexion crease, allows skin relaxation and prevents the contracture a straight transverse incision would cause.
- Incise skin and subcutaneous fat; immediately beneath the superficial fascia on the lateral side of the biceps tendon, identify the lateral antebrachial cutaneous nerve as it emerges from beneath the tendon and runs distally on the brachioradialis.
- Tag it with a vessel loop and protect it throughout - injury causes permanent lateral forearm numbness.
- Identify the biceps tendon and the bicipital aponeurosis (a broad fascial expansion from the medial border of the tendon into the forearm deep fascia); incise it in line with the incision to expose the underlying neurovascular bundle.
- The brachial artery lies centrally, surrounded by venae comitantes; the median nerve lies immediately medial to it.
- Place vessel loops around the brachial artery (with its venae comitantes) and the median nerve separately, and gently retract the bundle medially.
- Identify the artery first, then the nerve medial to it - this protects them during deeper dissection and gives safe access to the capsule and the distal biceps insertion.
- Develop the internervous interval between brachialis (musculocutaneous nerve, medial) and brachioradialis (radial nerve, lateral) - the deep internervous plane.
- The radial nerve lies within or just lateral to this interval; identify and protect it before any deep retraction. It divides into the superficial radial nerve (sensory) and the posterior interosseous nerve (motor) at about the level of the radial head.
- With the bundle protected medially and the radial nerve protected laterally, incise the anterior capsule in the midline or just medial to the radial head, protecting the coronoid and radial head articular surfaces.
- For distal biceps repair, identify the retracted tendon and the bare radial tuberosity (supinate the forearm to expose it); for capsular release, elevate the capsule from the anterior humerus and coronoid.
The posterior interosseous nerve lies immediately lateral and deep to the radial tuberosity and is the structure most at risk during distal biceps repair - it is injured in 1 to 3 percent of single-incision repairs. Supinate the forearm to swing the tuberosity and the nerve apart, keep the dissection on bone, stay aware of the lateral and deep interval, and never place retractors aggressively against the lateral radial neck.
Superficially the incision crosses the territories of the lateral antebrachial cutaneous nerve laterally and the medial antebrachial cutaneous nerve medially - both must be identified and protected under the subcutaneous fat. The genuine internervous plane is deep, between brachialis (musculocutaneous) and brachioradialis (radial); proximally this is a direct continuation of the Henry approach.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Lateral antebrachial cutaneous nerve (lateral to biceps, under fascia)
- Protection
- Identify under fascia before deeper dissection; vessel loop; avoid traction
- Structure at risk
- Medial antebrachial cutaneous nerve; cephalic and basilic veins
- Protection
- Protect during medial dissection; ligate veins only as needed
- Structure at risk
- Brachial artery (central, deep to bicipital aponeurosis) and median nerve (medial to artery)
- Protection
- Identify artery first, nerve medial; separate vessel loops; gentle medial retraction; no blind clamping
- Structure at risk
- Radial nerve between brachialis and brachioradialis
- Protection
- Identify in the interval before deep retraction; vessel loop
- Structure at risk
- Posterior interosseous nerve (lateral and deep to the radial tuberosity)
- Protection
- Supinate the forearm; stay on bone at the tuberosity; careful retractor placement
Anterior scarring - the major long-term risk. Anterior elbow scarring leading to flexion contracture is the most significant long-term complication, occurring in 10 to 20 percent of cases. It is more common after prolonged surgery, excessive retraction, or a straight rather than lazy-S incision. Prevention is meticulous soft-tissue handling, a layered closure without tension, and early range-of-motion exercises; an established contracture may require surgical release. Extensile options. Extend proximally along the medial border of the biceps (a direct continuation of the Henry approach) to reach the distal humerus and the brachial artery in the arm. Extend distally along the lateral forearm, developing the brachioradialis-pronator interval, to reach the proximal radius and radial head - identify and protect the PIN as it enters the supinator. The radial head is accessible through the lateral aspect of the fossa for replacement or ORIF, and for complex trauma the anterior approach can be combined with a lateral (Kocher) or medial approach. Closure. Copious irrigation and meticulous haemostasis (particularly around the venae comitantes) before tourniquet release. Close the deep fascia loosely if it was opened, approximate the subcutaneous tissue with absorbable suture, and close skin without tension. Apply a well-padded posterior splint or hinged brace and document neurovascular status immediately.
- Incidence
- 10 to 20 percent
- Prevention
- Lazy-S incision, layered closure, early motion
- Treatment
- Physiotherapy; possible re-release
- Incidence
- 5 to 15 percent
- Prevention
- Identify under fascia; vessel loop
- Treatment
- Often permanent numbness; desensitisation
- Incidence
- 5 to 10 percent
- Prevention
- Early motion; prophylaxis in high-risk cases
- Treatment
- Excision after maturation if symptomatic
- Incidence
- 2 to 5 percent
- Prevention
- Careful retraction
- Treatment
- Observe; most recover in 3 to 6 months
- Incidence
- 3 to 5 percent
- Prevention
- Avoid tight closure; meticulous haemostasis
- Treatment
- Wound care; possible skin graft
- Incidence
- 1 to 3 percent
- Prevention
- Protect during tuberosity work
- Treatment
- Wrist-drop splint; observe; explore if no recovery
- Incidence
- 1 to 2 percent
- Prevention
- Prophylactic antibiotics; sterile technique
- Treatment
- Irrigation and debridement; antibiotics
Procedures Through This Approach
- Distal biceps tendon repair - prepare the tendon with locking sutures and reattach to the posterior aspect of the radial tuberosity using a cortical button, suture anchors, or transosseous tunnels; confirm full supination and flexion strength and protect the PIN throughout tuberosity preparation.
- Anterior capsular release for post-traumatic or post-operative stiffness - elevate the capsule from the anterior humerus and coronoid, release heterotopic ossification or scar, and perform a gentle manipulation; avoid over-release, which causes instability.
- Brachial artery exploration and repair - expose the artery proximal and distal to the zone of injury and repair with direct suture, vein patch, or interposition graft.
- Median nerve exploration or neurolysis, and radial nerve or PIN exploration in the proximal forearm.
- Coronoid process fracture fixation through anterior access.
Viva & Exam Focus
ELBOW SAFEELBOW SAFE - the anterior elbow approach
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old man presents with a distal biceps tendon rupture after lifting a heavy object. How would you approach the repair?”
“A 35-year-old patient has post-traumatic elbow stiffness with only 30 to 110 degrees of motion nine months after a distal humerus fracture. How would you plan an anterior capsular release?”
“A patient presents with an elbow dislocation and an absent radial pulse after closed reduction. How would you approach vascular exploration?”
Incision
- Lazy-S or curved incision (medial proximal to lateral distal)
- Prevents skin and flexion contracture; total length 12 to 15 cm
- Proximal limb over the medial biceps, distal over the brachioradialis-pronator interval
Superficial structures at risk
- Lateral antebrachial cutaneous nerve - lateral to the biceps under fascia
- Injury causes permanent lateral forearm numbness
- Medial antebrachial cutaneous nerve and cephalic/basilic veins
Deep neurovascular bundle
- Brachial artery - central, deep to the bicipital aponeurosis
- Median nerve - immediately medial to the artery
- Identify the artery first, then the nerve; separate vessel loops
Internervous plane
- Brachialis (musculocutaneous) versus brachioradialis (radial)
- Radial nerve lies within or just lateral to the interval
- PIN lies lateral and deep to the radial tuberosity
Key procedures
- Distal biceps repair to the posterior radial tuberosity
- Anterior capsular release for stiffness
- Brachial artery or nerve exploration
Major complications
- Anterior scarring and flexion contracture (10 to 20 percent)
- Lateral antebrachial cutaneous nerve injury (5 to 15 percent)
- Median nerve neurapraxia (2 to 5 percent), PIN injury (1 to 3 percent)
References
The anterior elbow approach is used worldwide for distal biceps repair, anterior capsular release, and neurovascular exploration. The lazy-S incision, early identification of the brachial artery and median nerve, and protection of the lateral antebrachial cutaneous nerve and PIN are universal requirements across contemporary practice. Population evidence. Distal biceps rupture has an incidence of approximately 1.5 to 5.4 per 100,000 person-years, predominantly in men aged 40 to 60. Single-incision repair is the most common technique globally, with PIN injury rates of 1 to 3 percent and anterior scarring rates of 10 to 20 percent. Early motion protocols reduce post-operative stiffness. Consent (globally applicable). Discuss brachial artery injury (less than 1 percent), median nerve injury (2 to 5 percent, mostly transient), lateral antebrachial cutaneous nerve injury (5 to 15 percent, often permanent numbness), PIN injury (1 to 3 percent), anterior scarring and flexion contracture (10 to 20 percent), infection (1 to 2 percent), and the possibility of incomplete recovery of motion or strength.
Correction of post-traumatic flexion contracture of the elbow by anterior capsulotomy.
- Anterior capsular release through the anterior approach reliably improves extension in post-traumatic stiffness
- Average gain of 30 to 40 degrees of extension with a low complication rate when performed carefully
- The key to success is complete release of the anterior capsule and any heterotopic bone while protecting neurovascular structures
Complications of repair of the distal biceps tendon with the modified two-incision technique.
- PIN injury occurs in 1 to 3 percent of single-incision distal biceps repairs
- The nerve lies immediately lateral and deep to the radial tuberosity and is at greatest risk during tuberosity preparation
- Two-incision techniques reduce but do not eliminate PIN risk
Complications After Distal Biceps Tendon Repair: A Systematic Review.
- The overall complication rate following distal biceps tendon repair is substantial
- Lateral antebrachial cutaneous nerve palsy is a frequent complication of the anterior single-incision approach
- Meticulous soft-tissue handling is needed to prevent neurological injuries
Optimization of Anterior Incision Placement for Distal Biceps Repair.
- A transverse or lazy-S incision in the antecubital fossa helps reduce scarring and contracture
- Anatomical landmarks aid proper incision placement over the interval to protect neurovascular structures
- Optimised incision placement minimises cutaneous nerve injury and post-operative flexion contractures