Subpectoral or suprapectoral tenodesis · simple arthroscopic tenotomy · intermediate
- Tenotomy vs tenodesis turns on patient age, activity demands and cosmesis — pooled randomised-trial evidence (Hartland 2022, Zhou 2021) shows EQUIVALENT pain relief, function and elbow flexion/supination strength; the only consistent difference is a higher Popeye deformity rate after tenotomy. Tenotomy is not the wrong answer for the right patient (elderly, low demand, cosmesis not a concern).
- Subpectoral tenodesis gives the most reliable cosmetic result (lowest Popeye rate; the tendon is fixed distal to the groove at the myotendinous junction). The suprapectoral or in-groove site is simpler but leaves the tendon nearer the pathological groove and brings the axillary nerve to within about 10mm if bicortical drilling is attempted.
- For SLAP Type II, tenodesis is preferred over the age of 35-40 due to poor labral healing biology and a high SLAP-repair failure rate (Provencher 2013 — 37% failure overall, age over 36 relative risk 3.45). A concomitant rotator cuff tear further favours tenodesis.
- Interference screw, cortical button and suture anchor are the three main fixation modalities — biomechanically all achieve a similar ultimate failure load (Mazzocca 2005), but the subpectoral interference screw shows the least cyclic displacement.
- Neurovascular risk is fixation-site dependent: the AXILLARY nerve is closest at the suprapectoral level (about 10mm; Sethi 2014), where bicortical drilling is hazardous; at the SUBpectoral site the musculocutaneous nerve lies a mean 37mm away and the radial nerve about 48mm — keep retractors lateral and on bone.
- LHB pathology rarely occurs in isolation — it commonly coexists with subacromial-subdeltoid (SASD) bursitis, rotator cuff disease (especially the superior subscapularis) or AC joint arthritis; treat the underlying shoulder pathology simultaneously or pain will persist.
When & Why
Indication. Symptomatic long head of biceps (LHB) pathology that has failed non-operative treatment — activity modification, NSAIDs, physiotherapy and usually a subacromial corticosteroid injection. The pathology that brings a patient to biceps surgery spans four patterns: - Bicipital tenosynovitis — inflammation within the synovial sheath in the bicipital groove. Anterior shoulder pain, a positive Speed test (resisted forward flexion in supination with the elbow extended), a positive Yergason test (resisted supination with the elbow flexed 90 degrees), and tenderness in the groove.
- LHB partial tear — fraying or partial-thickness tearing in the groove or at the intertubercular entrance. MRI shows focal signal change, an irregular contour or a partial defect; often associated with a superior-fibre tear of the subscapularis.
- LHB instability (medial subluxation) — a subscapularis tear or rotator interval disruption lets the LHB sublux or dislocate medially over the lesser tuberosity, with clicking on rotation. A subscapularis tear is present in virtually all cases — treat both.
- SLAP lesions (Superior Labrum Anterior to Posterior) — Snyder Types I-IV. Type II (detachment of the superior labrum and LHB anchor from the supraglenoid tubercle) is the most common operative type and poses the repair-versus-tenodesis decision. The one decision that matters — tenotomy or tenodesis. Once you have decided to operate on the biceps, the choice between a simple tenotomy and a tenodesis rests on patient age, activity demands and cosmesis. The highest-level evidence shows the two give equivalent pain relief and strength, so the decision turns on whether the patient will accept a Popeye deformity.
An older, low-demand, non-manual patient who explicitly accepts a possible Popeye deformity; a frail patient where a shorter operative time is advantageous; bilateral shoulder surgery in the elderly; or a massive irreparable rotator cuff tear where tenotomy is performed during cuff debridement. Pooled RCT evidence shows equivalent pain relief and strength to tenodesis, with a shorter operative time.
A younger, active patient or manual worker concerned about cosmesis; a patient who prioritises arm symmetry and contour; SLAP II over the age of 35-40 (tenodesis preferred to SLAP repair); or a young patient with isolated LHB pathology and an intact cuff. The subpectoral site gives the most reliable contour.
Consent specifically for a Popeye deformity (far more common after tenotomy — counsel every patient and document it), bicipital cramping or fatigue pain, residual achiness at the tenodesis site for 6-12 months, the small risk of nerve injury (axillary or musculocutaneous), fixation failure or re-rupture, and the rare periprosthetic humeral fracture. Setup. Beach chair at about 45 degrees (or lateral decubitus), a standard shoulder arthroscopy setup, and an interscalene regional block. The operation is two stages: arthroscopic first (to treat concomitant pathology and release the LHB), then the subpectoral incision for tenodesis. The arm is draped free so it can be repositioned into slight abduction and external rotation to expose the axillary fold.
The Operation
The goal is to confirm the LHB pathology arthroscopically, release the tendon, and then — for a tenodesis — retrieve it distal to the pathological groove through a subpectoral exposure and fix it at physiological tension so the muscle belly does not retract. The exposure (the subpectoral approach to the bicipital groove) is laid out in full as the first operative steps below — it is the heart of the operation.
Operative sequence — subpectoral tenodesis (Mazzocca)
- Beach chair at about 45 degrees, interscalene block, standard shoulder arthroscopy setup, arm draped free.
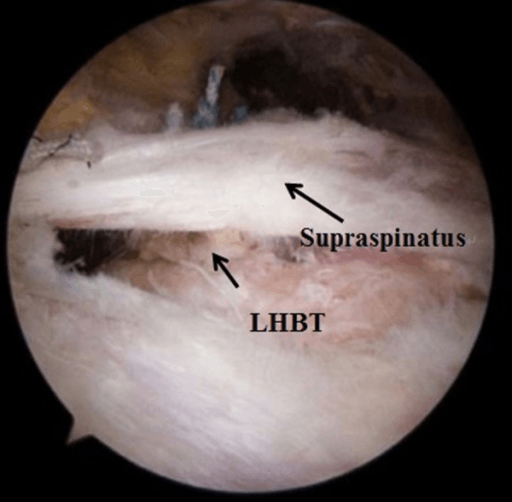
- Posterior viewing portal with an anterior rotator-interval working portal. Identify the LHB at its origin on the supraglenoid tubercle and superior labrum; assess tendon quality, fraying, intra-articular length, and the rotator interval and superior subscapularis fibres.
- Address whatever else is driving the pain before touching the biceps — subacromial decompression for impingement, rotator cuff repair for a tear, rotator interval closure for instability, AC joint arthroplasty for AC arthritis.
- LHB pathology is rarely isolated. Operating on the biceps alone, without treating the source of subacromial bursitis or a cuff tear, will not relieve the pain.
- With arthroscopic scissors or a radiofrequency device, transect the LHB at or just proximal to the bicipital groove entrance.
- Cut here rather than up at the supraglenoid origin — a long intra-articular stump can impinge. The tendon then retracts distally into the groove.
- For a planned tenotomy the procedure effectively stops at this cut (see the tenotomy note below).
- Reposition the arm into slight abduction and external rotation to expose the axillary fold and bring the pectoralis major inferior border into view.
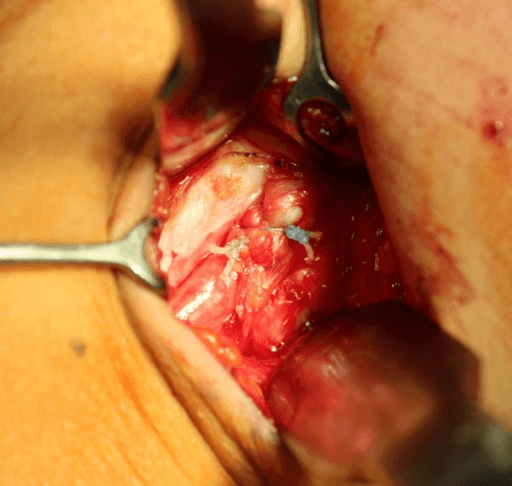
- Make a 3-4cm longitudinal incision in the axillary crease, centred on the inferior border of the pectoralis major tendon (its anterior or inferior lamina is the surface landmark). Incise skin and subcutaneous fat.
- Develop the interval between the medial aspect of the pectoralis major tendon insertion and the proximal humerus with blunt dissection (a finger or a small Cobb elevator).
- Palpate the bicipital groove on the anterior humeral shaft 1-2cm below the pectoralis major inferior border. Identify the groove before placing any drill guide.
- With a small curved haemostat or tendon-grasping forceps, retrieve the retracted LHB from within the groove and deliver it gently into the wound.
- Keep retractors lateral and on bone or the pectoralis major tendon — never deep and medial, where the musculocutaneous nerve lies.
- Whipstitch (Krakow) the distal 2cm of the LHB with a No. 2 non-absorbable suture such as FiberWire.
- Do not trim the tendon excessively — maintain length to avoid shortening the biceps and producing a flexion contracture.
- On the anterior proximal humerus, 1-2cm below the inferior pectoralis major border, prepare an intramedullary socket with a cannulated drill over a guide wire — typically 7-8mm diameter and about 2.5cm depth.
- Do not over-ream (it risks a humeral fracture) and do not breach the posterior cortex at this proximal level (the axillary nerve — see the safety note). Confirm position with fluoroscopy if available.
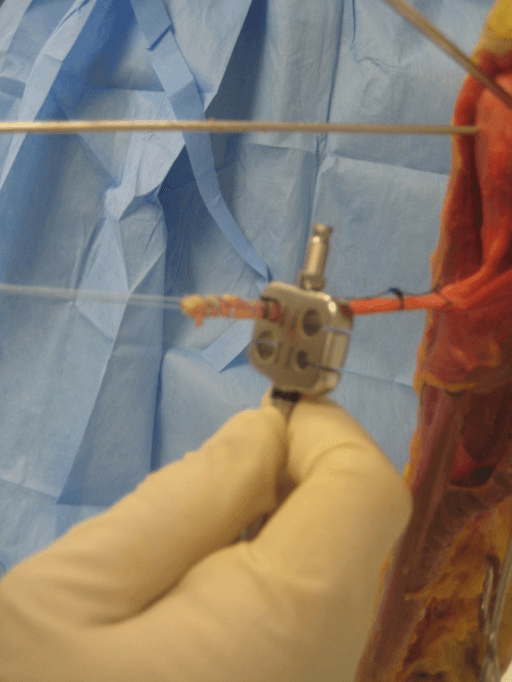
- Pass the tendon-loaded suture into the socket and insert a matching-diameter (7-8mm, 2.5cm) bioabsorbable or metal interference screw while maintaining tension on the whipstitch sutures; tie the sutures over the screw for added security.
- Alternative — a cortical button (Endobutton): the tendon is passed through a bone tunnel and the button flipped on the far cortex. This is useful if socket preparation is difficult, though the button may be palpable on the lateral cortex.
- Tension the biceps in a comfortable resting position — elbow at 90 degrees, forearm neutral rotation, no excessive distal traction on the tendon. Overtensioning causes an elbow flexion contracture; undertensioning lets the belly retract into a Popeye deformity.
- Close subcutaneous fat with an absorbable suture and skin with a subcuticular absorbable suture.
The arthroscopic and fixation moments of the same operation:
At the SUPRApectoral level the axillary nerve lies only about 10mm from the tenodesis site (the guide pin contacted it in 20% of cadaveric suprapectoral tenodeses, Sethi 2014). Never perform bicortical posterior-cortex drilling here — keep fixation unicortical or use a low-profile socket. At the SUBpectoral site the musculocutaneous nerve lies a mean 37mm away and the radial nerve about 48mm away, so direct hardware injury is uncommon — the real subpectoral risk is a stretch or retraction injury to the musculocutaneous nerve from aggressive MEDIAL retraction with a deep Langenbeck or Hohmann. Keep self-retaining retractors lateral and on bone, limit retractor time, and identify the bicipital groove before drilling.
Fix the tendon with the elbow at 90 degrees, the forearm in neutral rotation, and no active pull on the tendon — let it sit at physiological resting length. Too tight and the patient develops an elbow flexion contracture; too loose and the muscle belly retracts distally, producing the very Popeye deformity the tenodesis was meant to prevent.
The subpectoral site fixes the tendon distal to the pathological groove at the myotendinous junction, giving the most reliable contour and removing the tendon from the zone of groove pathology; the cost is a second axillary incision. The suprapectoral site needs no extra incision but leaves the tendon near the pathological groove (a higher residual Popeye risk) and brings the axillary nerve to within about 10mm if bicortical drilling is attempted — keep it unicortical.
When tenotomy is the chosen operation, the procedure is entirely arthroscopic and far shorter. From the posterior viewing portal with an anterior working portal, transect the LHB as close to its supraglenoid origin as possible with arthroscopic scissors or radiofrequency, then allow it to retract distally into the groove (it usually comes to rest below the groove, sometimes in the subpectoral region). Inspect the superior labrum to confirm no flap remains that could cause mechanical symptoms. There is no fixation and no second incision — a sling for comfort only.
Aftercare & Complications
Rehabilitation — tenodesis. Protect the tenodesis for 6 weeks: no resisted elbow flexion and no supination against resistance in that window, or the fixation will fail. | Phase | Timing | Restriction | Therapy | |-------|--------|-------------|---------| | 1 | 0-6 weeks | Sling; gravity-assisted elbow flexion only; no resisted elbow flexion or supination against resistance | Pendulums, wrist and hand exercises from day 1; passive or active-assisted shoulder ROM within pain tolerance | | 2 | 6-12 weeks | Wean the sling | Active elbow flexion against gravity, gentle isometric biceps work, progressive shoulder ROM | | 3 | 12-16 weeks | None | Progressive resistive biceps and supination strengthening, sport-specific loading; target full flexion/supination strength by 16 weeks | | 4 | 16-24 weeks | None | Return to manual work and non-contact sport; heavy manual or contact sport at 4-6 months; overhead throwing typically 6 months | Rehabilitation — tenotomy. Far simpler: a sling for comfort for 2-4 weeks, no elbow restriction, early active ROM, with physiotherapy directed at the underlying shoulder pathology treated simultaneously. Full activities at 6-12 weeks unless restricted by a concomitant procedure. Critical point. Do not allow early resisted elbow flexion or forceful supination against resistance in the first 6 weeks after tenodesis — this loads the tenodesis site and risks fixation failure. Driving. Tenotomy — return to automatic driving when comfortable, typically 2-4 weeks. Tenodesis — 4-6 weeks (after sling removal); a manual vehicle at 8-10 weeks. Outcome expectations. Anterior shoulder pain from LHB pathology resolves progressively over 3-6 months; some residual achiness around the tenodesis site is common for 6-12 months and is not a sign of failure. Pooled RCT data show elbow flexion and supination strength return to near-symmetric with either procedure (Zhou 2021) — reassure patients that measurable strength loss is small and usually adapts. Complications
- Incidence
- Commonly about 20-40% after tenotomy (roughly 3x tenodesis; meta-analysis OR 0.29); 9% vs 27% in Koh 2010
- Prevention
- Patient selection — tenotomy only for patients who accept this; subpectoral tenodesis if cosmesis matters
- Management
- Reassurance; exercises do not correct it. For truly disabling cramping or pain, revision subpectoral tenodesis
- Incidence
- Reported by a minority; not significantly different from tenodesis in pooled RCT data
- Prevention
- Preoperative counselling; favour tenodesis in higher-demand patients
- Management
- Usually resolves by 6-12 months as the muscle adapts; eccentric strengthening; revision rarely required
- Incidence
- No significant difference between tenotomy and tenodesis in pooled RCT data (Zhou 2021); any deficit is small and inconsistent
- Prevention
- Either procedure preserves clinically useful strength
- Management
- Physiotherapy strengthening; revision rarely needed for isolated weakness
- Incidence
- Uncommon, in the order of 1%; axillary nerve closest with proximal suprapectoral bicortical drilling (about 10mm)
- Prevention
- Stay lateral during retraction; avoid deep medial retractors; avoid bicortical drilling proximally
- Management
- EMG or NCS at 4-6 weeks; most neuropraxias recover by 3-6 months; explore if no recovery
- Incidence
- Low (a single failure in the Mazzocca 2008 series of 41)
- Prevention
- Correct socket size, an adequate whipstitch, appropriate tensioning, and a sling for 4-6 weeks
- Management
- Popeye appearance; revision tenodesis if symptomatic, conservative if asymptomatic or low-demand
- Incidence
- Less than 0.5% — a stress riser from the socket
- Prevention
- Do not over-ream; 7-8mm maximum diameter; avoid bicortical perforation
- Management
- Undisplaced crack — cerclage wire and a sling for 6 weeks; displaced — ORIF with a plate bypassing the socket
- Incidence
- 1-2%
- Prevention
- Perioperative cefazolin, minimise dead space, aseptic technique
- Management
- Superficial — oral antibiotics; deep — washout, retain fixation if stable
Viva & Exam Focus
TENOTOMYTENOTOMY — when tenotomy is the right choice
TENODESISTENODESIS — when tenodesis is the right choice
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old overhead worker — a carpenter specialising in roof frame construction — presents with 8 months of right anterior shoulder pain localised to the bicipital groove. MRI shows moderate LHB tenosynovitis and a partial-thickness intrasubstance tear of the LHB with no rotator cuff tear. He is right-hand dominant and heavily relies on forceful supination for his work. He asks your advice: should he have a tenotomy or tenodesis? Walk me through your decision-making.”
“Three weeks following an arthroscopic biceps tenotomy (combined with subacromial decompression), your patient returns to clinic. He reports he is generally pleased with the reduction in anterior shoulder pain, but is distressed by a noticeable lump in his mid-upper arm and has noticed his right biceps looks different from his left. On examination there is a visible muscle belly deformity in the mid-upper arm consistent with a Popeye deformity. He says this was not discussed with him before the operation. How do you manage this situation?”
“A 40-year-old right-handed recreational rock climber is reviewed in your clinic with right shoulder pain following a forceful pulling injury during a difficult climb. MRI arthrogram confirms a Type II SLAP lesion with detachment of the superior labrum and LHB anchor from the supraglenoid tubercle. He is otherwise fit and well with no other shoulder pathology. His shoulder is not painful at rest but he cannot climb at grade 7 (his previous level). Should you repair the SLAP or perform a tenodesis, and why?”
Tenotomy — right patient
- Older, low-demand, sedentary, non-manual occupation
- Patient explicitly accepts a higher Popeye deformity risk (roughly 3x tenodesis)
- Massive irreparable rotator cuff tear with concomitant LHB pathology — tenotomy during cuff debridement
- Quickest procedure (shorter operative time confirmed in meta-analysis), minimises anaesthetic time in a frail patient
- Koh 2010 (PMID 20551285): equivalent pain relief and elbow flexion strength to tenodesis; only more Popeye
Tenodesis — right patient
- Younger, active, values arm symmetry and contour
- Cosmesis important — Popeye deformity unacceptable to the patient
- SLAP II over age 35-40 — tenodesis preferred over SLAP repair (Boileau 2009, PMID 19229046)
- Subpectoral preferred: reliable cosmesis, least cyclic displacement (Mazzocca 2005, PMID 16325079; clinical Mazzocca 2008, PMID 18697951)
- Interference screw, cortical button or suture anchor — similar failure load, know each
SLAP II — repair vs tenodesis decision
- Under 35, competitive overhead throwing athlete — SLAP repair (preserve native anatomy, superior labrum important for throwing mechanics)
- Over 35-40 — tenodesis preferred: SLAP repair failure about 37% with age over 36 RR 3.45 (Provencher 2013), tenodesis 87% return to sport (Boileau 2009)
- Concomitant rotator cuff tear — favour tenodesis (a cuff tear worsens SLAP repair outcomes)
- Stiffness from SLAP repair is significant in overhead athletes — tenodesis avoids capsular tightening
- SLAP classification: I (fray, debride), II (anchor detachment — operative decision), III (bucket-handle, debride), IV (extends into LHB — consider tenodesis)
Key anatomy
- Axillary nerve closest with proximal or suprapectoral posterior-cortex drilling (about 10mm); musculocutaneous nerve a mean 37mm and radial nerve 48mm from the subpectoral site (Sethi 2014)
- Pectoralis major inferior border — landmark for subpectoral incision placement (1-2cm below this)
- LHB origin: supraglenoid tubercle and superior labrum — the anchor is detached in Type II SLAP
- Bicipital groove: between the greater and lesser tuberosities, roof is the transverse humeral ligament, associated with the subscapularis superior fibres medially
Complications
- Popeye deformity: roughly 3x more common after tenotomy (about 27% vs 9% in Koh 2010) — preoperative counselling mandatory
- Elbow flexion / supination strength: no significant difference between tenotomy and tenodesis in pooled RCT data (Zhou 2021)
- Bicipital cramping: reported by a minority post-tenotomy, usually resolves by 6-12 months
- Nerve injury: uncommon; axillary nerve closest with proximal suprapectoral bicortical drilling — avoid bicortical fixation there
- Tenodesis failure: low (a single failure in the Mazzocca 2008 clinical series of 41); varies with technique and bone quality
Exam tips
- Know the key papers: Koh 2010 PMID 20551285 (tenotomy vs tenodesis — only Popeye differs), Boileau 2009 PMID 19229046 (tenodesis vs repair for SLAP), Provencher 2013 PMID 23460326 (SLAP repair 37% failure, age over 36), Mazzocca 2005/2008 PMID 16325079/18697951 (subpectoral interference screw)
- Age threshold 35-40 for SLAP II — above this, tenodesis is preferred over repair
- Popeye deformity is EXPECTED from tenotomy — must warn preoperatively, document in consent
- Nerve anatomy is an exam favourite — axillary nerve about 10mm at the suprapectoral site, musculocutaneous about 37mm and radial about 48mm at the subpectoral site (Sethi 2014)
- Always treat concomitant shoulder pathology — LHB disease is rarely isolated (commonly associated SASD bursitis, rotator cuff, or subscapularis pathology)
Background & Evidence
Epidemiology. LHB pathology is one of the commonest sources of anterior shoulder pain, increasingly recognised as arthroscopic diagnosis has improved. It rarely occurs in isolation — in greater than 90% of cases it coexists with subacromial-subdeltoid (SASD) bursitis, a rotator cuff tear (especially the superior subscapularis fibres, whose tendon border attaches partly to the bicipital groove sheath) or AC joint arthritis. It predominates in patients over 40 and in overhead or manual workers. Pathoanatomy. The LHB originates from the supraglenoid tubercle and the posterosuperior glenoid labrum — its anchor accounts for about 40-50% of the posterosuperior labral attachment. It passes over the humeral head from posterosuperior to anteroinferior, entering the rotator interval between the supraspinatus (superiorly) and the subscapularis (inferiorly). The superior glenohumeral ligament (SGHL) and coracohumeral ligament (CHL) form a pulley that stabilises the tendon at the groove entrance; disruption of this pulley, or a subscapularis tear, allows medial subluxation. The tendon then enters the bicipital groove — between the greater and lesser tuberosities, 5-12mm wide, 4-6mm deep and about 7-8cm long, roofed by the transverse humeral ligament — surrounded by a synovial sheath continuous with the glenohumeral joint. The anterior humeral circumflex vessels run along the inferior groove margin.
- Feature
- Fraying or degeneration of the superior labrum; LHB anchor intact
- Management
- Debridement
- Feature
- Detachment of the superior labrum and LHB anchor from the supraglenoid tubercle (the most common operative type, 50-60%)
- Management
- Repair under 35-40 in a thrower; tenodesis over 35-40
- Feature
- Bucket-handle tear of the superior labrum; LHB anchor intact
- Management
- Resect the unstable fragment if displacing; preserve the anchor
- Feature
- Bucket-handle tear extending into the LHB tendon itself
- Management
- If less than 50% — repair and tubularise; if greater than 50% — tenodesis
Nerve anatomy — why fixation site matters. The musculocutaneous nerve (lateral cord, C5-C7) exits posterior and lateral to pectoralis minor and enters the deep surface of coracobrachialis a variable distance distal to the coracoid. In a cadaveric model (Sethi 2014) the distance from the tenodesis site to the axillary nerve was 10.5mm at the suprapectoral level versus 36.7mm subpectoral; at the subpectoral site the musculocutaneous nerve lay a mean 37.4mm and the radial nerve 48.0mm away. The axillary nerve — not the musculocutaneous — is therefore the structure most at risk, which is why bicortical posterior-cortex fixation at the suprapectoral level is avoided. Key evidence. Koh (2010, 90 patients over 55 with a cuff tear plus an LHB lesion) found tenodesis reduced Popeye deformity (9% vs 27%, P = 0.04) but no other variable differed. Two meta-analyses of randomised trials (Hartland 2022, 860 patients across 11 RCTs; Zhou 2021, 9 RCTs) confirm tenotomy and tenodesis give equivalent function, pain and elbow flexion or supination strength, with tenodesis only reducing Popeye deformity (OR about 0.29) and tenotomy offering a shorter operative time — directly refuting the older teaching of a large fixed supination deficit. For SLAP, Boileau (2009) showed 87% return to sport after tenodesis versus 20% after SLAP repair, and Provencher (2013, 179 SLAP repairs) found a 37% failure rate with age over 36 the only independent predictor (RR 3.45). Biomechanically, Mazzocca (2005) showed the subpectoral interference screw had the least cyclic displacement (1.5mm) with a similar ultimate failure load across four constructs, and the clinical series (Mazzocca 2008, 41 patients) reported significant score gains with a single fixation failure.
References
Treatment of biceps tendon lesions in the setting of rotator cuff tears: prospective cohort study of tenotomy versus tenodesis
- 90 patients over 55 years with a rotator cuff tear plus LHB lesion, treated consecutively with suture-anchor tenodesis (n=45) or tenotomy (n=45)
- Popeye deformity occurred in 9% (tenodesis) versus 27% (tenotomy), P = 0.04 — the only significant difference between groups
- No significant difference in cramping pain or in elbow flexor power ratio versus the contralateral side (0.92 tenodesis vs 0.94 tenotomy); ASES and Constant scores improved equally
Clinical effectiveness of tenotomy versus tenodesis for long head of biceps pathology: a systematic review and meta-analysis
- 860 patients across 11 randomised controlled trials (426 tenotomy vs 434 tenodesis)
- Comparable patient-reported function (SMD 0.14, P = 0.13) and pain; tenodesis significantly reduced Popeye deformity (OR 0.29, P less than 0.00001)
- Tenotomy had a significantly shorter operative time (mean difference about 15 minutes)
Biceps tenotomy versus tenodesis for lesions of the long head of the biceps tendon: a systematic review and meta-analysis of randomized controlled trials
- Pooled analysis of 9 randomised controlled trials comparing tenotomy and tenodesis
- No significant difference in ASES score, VAS pain, cumulative elbow flexion strength, cumulative elbow supination strength, or cramping pain
- Tenodesis reduced Popeye deformity (RR 0.33); tenotomy had a shorter operative time
Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion
- 25 patients with an isolated type II SLAP lesion: 10 SLAP repairs (mean age 37) versus 15 biceps tenodeses (mean age 52)
- 87% (13/15) returned to their previous level of sport after tenodesis versus only 20% (2/10) after SLAP repair (P = 0.01)
- Four failed SLAP repairs were successfully salvaged by subsequent biceps tenodesis
A prospective analysis of 179 type 2 superior labrum anterior and posterior repairs: outcomes and factors associated with success and failure
- 179 type II SLAP repairs in a young active cohort followed a mean of 40 months
- 37% met failure criteria with a 28% revision rate despite overall improvement in outcome scores
- Age over 36 years was the only independent predictor of failure (relative risk 3.45)
The biomechanical evaluation of four fixation techniques for proximal biceps tenodesis
- Cadaveric comparison of four tenodesis fixation methods (subpectoral bone tunnel, arthroscopic suture anchor, subpectoral interference screw, arthroscopic interference screw)
- The subpectoral interference screw showed the LEAST cyclic displacement (1.5mm)
- No statistically significant difference in ultimate failure load between methods (all roughly 165-252 N); all specimens failed at the tenodesis site
Clinical outcomes after subpectoral biceps tenodesis with an interference screw
- 41 of 50 patients followed (mean age 50, mean 29 months) after subpectoral biceps tenodesis with an interference screw
- Significant improvement in ASES, Constant, Rowe and SANE scores
- Only one fixation failure (tendon pull-out producing a Popeye deformity); patients with a coexistent rotator cuff lesion had significantly lower ASES scores
Safety of open suprapectoral and subpectoral biceps tenodesis: an anatomic assessment of risk for neurologic injury
- 10 cadaveric arms; the guide pin was in direct contact with the axillary nerve in 20% of suprapectoral tenodeses
- Distance from the tenodesis site to the axillary nerve was 10.5mm (suprapectoral) versus 36.7mm (subpectoral)
- At the subpectoral site the musculocutaneous nerve was a mean 37.4mm and the radial nerve 48.0mm from the tenodesis