Supine | Lateral Plateau ORIF | Common Peroneal Nerve and Anterior Tibial Vessels at Risk
- Supine positioning with a bump under the ipsilateral hip is standard for anterolateral access to the lateral plateau.
- The common peroneal nerve wraps posterolaterally around the fibular neck and must be identified and protected throughout.
- Subperiosteal elevation of the anterior compartment (tibialis anterior) off the lateral metaphysis is the key deep step.
- A submeniscal arthrotomy allows direct visualisation of the articular surface to confirm reduction.
- The anterior tibial vessels enter the anterior compartment 5-7 cm distal to the joint line and are at risk during distal elevation.
When & Why
What it exposes. The anterolateral approach gives direct access to the lateral tibial plateau and the anterolateral proximal tibial metaphysis. It is the workhorse exposure for the majority of lateral column tibial plateau fractures (Schatzker I, II and III), allowing placement of a buttress plate on the anterolateral surface and a submeniscal arthrotomy for direct visualisation of the articular surface. Why this approach (and not another). Lateral split and split-depression fragments displace with valgus and axial load, and a buttress plate on the anterolateral cortex counters exactly those forces. Submeniscal arthrotomy confirms anatomic reduction (goal less than 2 mm step-off). This approach cannot address posterolateral or medial column fragments, which need their own approaches. Indications. - Schatzker Type I (pure lateral split), Type II (lateral split-depression, the commonest indication) and Type III (pure lateral depression)
- Lateral buttress plating for valgus instability
- Elevation of depressed articular segments with bone grafting
- Revision surgery for malreduced lateral plateau fractures Contraindications. - Isolated medial or posteromedial fractures (use an anteromedial or posteromedial approach)
- Severe soft-tissue compromise over the lateral knee (delayed surgery or an alternative approach)
- Medical unfitness for supine positioning with knee flexion
- Active infection Alternative approaches and the three-column concept. The proximal tibia is planned by the three-column concept (lateral, medial and posterior columns): the anterolateral approach addresses the lateral column, while the medial column needs an anteromedial approach and the posterior column (posteromedial or posterolateral fragments) needs posteromedial or posterolateral approaches. An extended lateral approach with fibular neck osteotomy is reserved for complex bicondylar fractures requiring combined access. Position & landmarks. Supine on a radiolucent table with a small bump under the ipsilateral hip to internally rotate the limb, and the knee flexed 30-40 degrees over a radiolucent triangle to relax the posterior capsule. The C-arm comes from the contralateral side. Palpate and mark Gerdy's tubercle (the anterolateral ITB insertion), the fibular head (the key landmark for the common peroneal nerve), the lateral joint line, the tibial crest, and the patella and patellar tendon (the medial boundary of the incision).
The Exposure
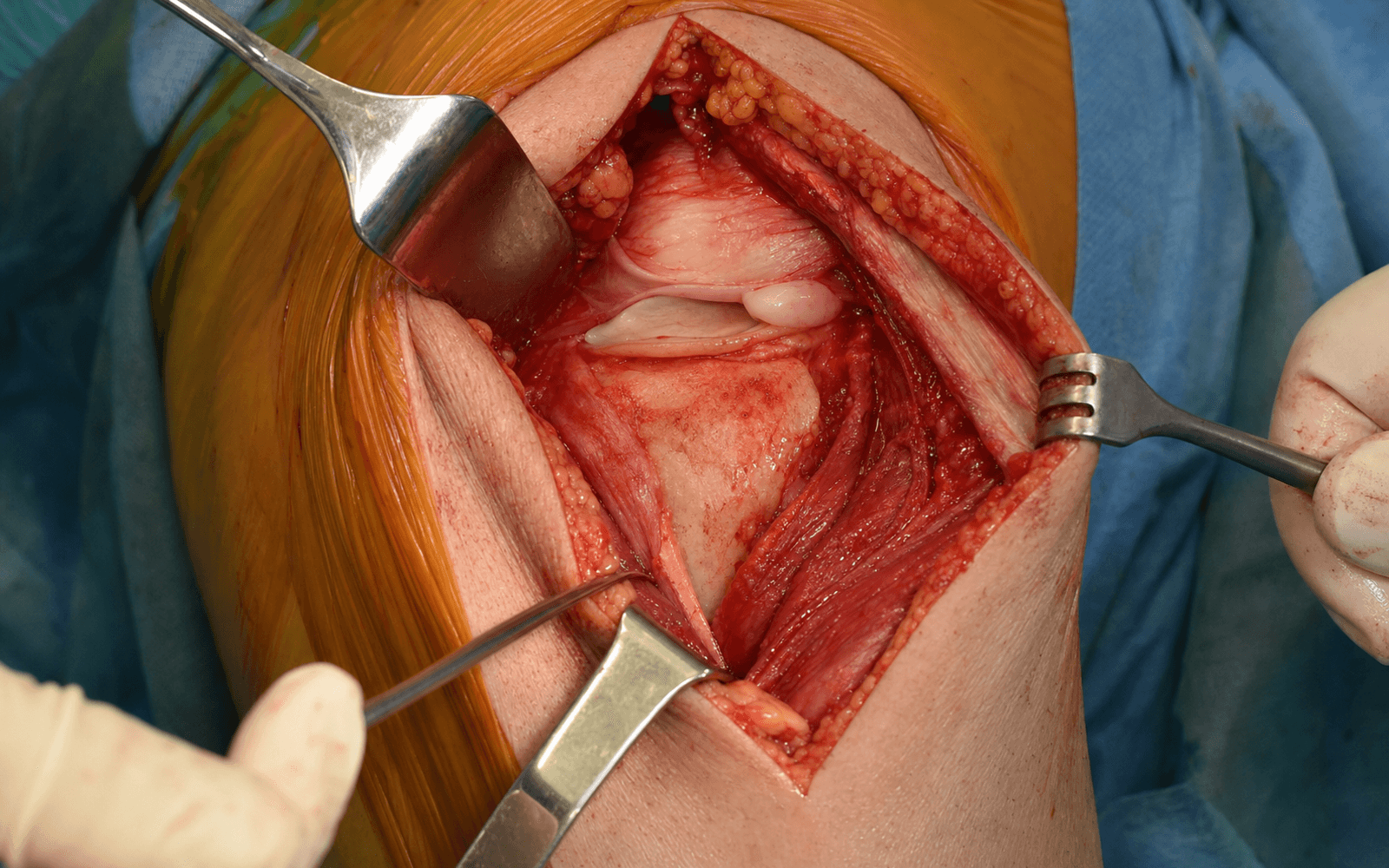
Work down through the layers over Gerdy's tubercle: incise the iliotibial band, elevate the anterior compartment subperiosteally off the lateral metaphysis (stopping short of the anterior tibial vessels), then open a submeniscal arthrotomy to see the joint.
Exposure sequence
- Supine on a radiolucent table; small bump under the ipsilateral hip for slight internal rotation.
- Flex the knee 30-40 degrees over a radiolucent triangle or bump to relax the posterior capsule and open the lateral plateau.
- High thigh tourniquet optional but commonly used; prepare and drape the entire limb free.
- Mark Gerdy's tubercle, the fibular head, the lateral joint line and the tibial crest.
- Make a hockey-stick incision starting 2-3 cm proximal to the joint line, curving anteriorly over Gerdy's tubercle and extending 8-12 cm distally along the anterior compartment (a straight lateral incision 1 cm posterior to the tibial crest is an alternative).
- Keep the incision anterior to the fibular head and stop the distal extent proximal to the anterior tibial artery entry point (5-7 cm).
- Incise skin and subcutaneous tissue and identify the iliotibial band inserting at Gerdy's tubercle.
- Incise the ITB in line with its fibres, or partially release its insertion at Gerdy's tubercle for exposure.
- Expose the anterior compartment fascia.
- Palpate (or visualise) the common peroneal nerve posterolaterally as it wraps the fibular neck 1-2 cm distal to the fibular head.
- Place a vessel loop around it for gentle protection; never place metal retractors directly on the nerve.
- Document ankle dorsiflexion (CPN function) before deep dissection proceeds.
- Incise the anterior compartment fascia longitudinally to expose tibialis anterior.
- Begin subperiosteal elevation of the anterior compartment musculature off the lateral metaphysis with a periosteal elevator, working lateral-to-medial and staying close to bone to protect the anterior tibial vessels.
- Continue elevating tibialis anterior, extensor hallucis longus and extensor digitorum longus off the lateral and anterior metaphysis.
- Stop elevation about 5 cm distal to the joint line — the anterior tibial artery enters the anterior compartment through the interosseous membrane at 5-7 cm and will be injured if you go further.
- Use Bennett or Hohmann retractors to maintain exposure.
- If articular visualisation is needed, incise the coronary (meniscotibial) ligament just below the lateral meniscus.
- Elevate the meniscus with a retractor to expose the articular surface for reduction assessment — do not detach the meniscus from its capsular attachment.
- Repair the coronary ligament (submeniscal arthrotomy) with absorbable sutures.
- Repair any ITB release; close the anterior compartment fascia loosely to avoid compartment syndrome.
- Close subcutaneous tissue and skin in layers; apply a hinged knee brace or immobiliser.
- Document CPN function (ankle dorsiflexion) before leaving theatre.
The common peroneal nerve is the most critical structure at risk. It wraps around the fibular neck 1-2 cm distal to the fibular head, and injury causes foot drop. Identify it early by palpation, protect it with a vessel loop or tape sling, never place metal retractors directly on it, and document ankle dorsiflexion before and after the case. CPN palsy complicates 3-5 percent of anterolateral approaches; most are traction or compression neurapraxia with recovery within 6-12 months when the nerve is identified and protected.
The anterior tibial artery (with the deep peroneal nerve) pierces the interosseous membrane and enters the anterior compartment 5-7 cm distal to the lateral joint line. Continuing subperiosteal elevation beyond about 5 cm risks lacerating it and causing anterior compartment ischaemia. If more distal exposure is genuinely required, identify, mobilise and protect the vessels first.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Lateral sural cutaneous nerve branches; recurrent genicular vessels
- Protection strategy
- Careful haemostasis; ligate recurrent genicular vessels as needed
- Structure at risk
- Common peroneal nerve at the fibular neck (1-2 cm distal to the head) — MOST CRITICAL
- Protection strategy
- Identify by palpation before deep retraction; vessel loop; no metal retractors on the nerve
- Structure at risk
- Anterior tibial artery and deep peroneal nerve (enter the compartment 5-7 cm distal to the joint)
- Protection strategy
- Stop subperiosteal elevation at about 5 cm; identify and protect the vessels if more distal access is needed
- Structure at risk
- Lateral inferior genicular artery; lateral meniscus; coronary ligament
- Protection strategy
- Submeniscal arthrotomy that preserves the meniscal attachment; repair the coronary ligament at closure
Internervous plane. The theoretical internervous plane is between the anterior compartment (tibialis anterior, deep peroneal nerve) and the lateral compartment (peroneus longus, superficial peroneal nerve). In practice, no true intermuscular plane is developed — instead the entire anterior compartment is elevated subperiosteally as a unit off the lateral metaphysis, staying anterior to the fibular head and the lateral collateral ligament. The recurrent genicular vessels are usually ligated, and the ITB insertion at Gerdy's tubercle may be partially released for exposure. Muscular layers crossed
- Muscle
- Iliotibial band
- Nerve supply
- Superior gluteal (tensor fascia lata)
- Action
- Knee stabilisation
- Muscle
- Tibialis anterior
- Nerve supply
- Deep peroneal
- Action
- Ankle dorsiflexion
- Muscle
- Extensor hallucis longus
- Nerve supply
- Deep peroneal
- Action
- Great-toe extension
- Muscle
- Extensor digitorum longus
- Nerve supply
- Deep peroneal
- Action
- Toe extension
- Muscle
- Peroneus longus
- Nerve supply
- Superficial peroneal
- Action
- Eversion, plantarflexion
Extensile options. Extend proximally along the lateral border of the patella into a lateral parapatellar arthrotomy for intra-articular access (or with a tibial tubercle osteotomy). Extend distally along the anterior compartment fascia for more distal metaphyseal or diaphyseal work, stopping short of the anterior tibial artery unless the vessels are identified and protected. For bicondylar fractures, combine with an anteromedial approach (same supine position) or a posteromedial or posterolateral approach (staged, repositioning to prone or lateral decubitus). A fibular neck osteotomy is reserved for the rare case needing posterolateral access through a single extended lateral incision. Closure. Layered: repair the coronary ligament with absorbable suture (2-0 or 3-0 Vicryl), repair any ITB release or retinaculum, close the anterior compartment fascia loosely (some surgeons leave it open proximally), close subcutaneous tissue in layers to eliminate dead space, and close skin with staples, nylon or absorbable subcuticular suture. Document CPN function before leaving theatre; check compartment pressures if there is concern (especially after prolonged surgery or tourniquet use). A drain is rarely required but, if used, is removed within 24-48 hours. Complications - Intraoperative: common peroneal nerve injury (3-5 percent), anterior tibial artery injury, inadequate reduction (greater than 2 mm step-off), intra-articular hardware placement.
- Early postoperative: wound dehiscence or infection (2-5 percent, higher with soft-tissue compromise), compartment syndrome (rare but possible after anterior compartment elevation), deep vein thrombosis, loss of reduction if fixation is inadequate.
- Late: post-traumatic osteoarthritis (20-40 percent long-term), knee stiffness (early ROM is essential), nonunion or malunion (less than 5 percent with proper technique), hardware prominence requiring removal.
- Failure management: early loss of reduction is managed with revision ORIF and bone grafting; infection with debridement, antibiotics and possible staged revision; established post-traumatic OA with arthroplasty in older patients or osteotomy in younger patients.
Procedures Through This Approach
- Tibial plateau ORIF — open reduction and internal fixation of lateral plateau fractures (Schatzker I-III) is the principal operation through this exposure.
- Lateral buttress plating for split and split-depression patterns, and elevation of depressed articular segments with bone grafting of the metaphyseal void.
- Submeniscal arthrotomy with direct articular inspection, plus lateral meniscal repair or partial meniscectomy if indicated. Fixation options. A contoured 3.5 mm buttress plate (T-plate, L-plate or anatomic proximal tibia plate) is applied to the anterolateral surface just distal to the joint line, with non-locking screws placed first to achieve the buttress effect and locking screws added for osteoporotic bone or comminution. Independent lag screws fix the split component, and bone graft or a bone graft substitute fills the metaphyseal void. Screws are directed medially and posteriorly. Reduction technique. Reduce the lateral split component with pointed or large pelvic reduction clamps; elevate depressed fragments with a bone tamp or elevator through a metaphyseal window or via the fracture line; support the elevated fragment with graft; and confirm reduction through the arthrotomy and on fluoroscopy (AP, lateral and oblique views). The goal is less than 2 mm articular step-off and restoration of tibial plateau width. Postoperative protocol and outcomes. A hinged knee brace locked in extension is applied; the patient is non-weight-bearing or toe-touch for the first weeks, with gentle ROM (0-90 degrees) once the wound is stable, progressing toward 0-120 degrees by 6 weeks, and progressive weight-bearing to full by 10-12 weeks. Radiographs are taken at 2, 6 and 12 weeks, then at 6 and 12 months (CT if reduction or hardware position is in question). Good-to-excellent results occur in 70-85 percent of patients with anatomic reduction (less than 2 mm step-off), which is the strongest predictor of long-term outcome; articular step-off greater than 2 mm and condylar widening greater than 5 mm predict poorer results. Post-traumatic OA leads to arthroplasty in about 5-8 percent within 10 years; the reoperation rate is 10-15 percent (hardware removal, revision, arthroplasty).
Viva & Exam Focus
ANTEROLATANTEROLAT — the anterolateral plateau exposure
DANGERDANGER — structures at risk, layer by layer
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old construction worker falls from height and sustains a tibial plateau fracture. CT shows a Schatzker II lateral split-depression pattern with 4 mm articular depression and 6 mm condylar widening. How would you approach this?”
“During an anterolateral approach for a lateral plateau fracture, you are about to elevate the anterior compartment when you feel a cord-like structure posterolaterally near the fibular neck. What is your next step?”
“You are performing an anterolateral approach and have elevated the anterior compartment 8 cm distal to the joint line. The scrub nurse asks why you stopped. What is your reasoning?”
Patient position
- Supine with a bump under the ipsilateral hip
- Knee flexed 30-40 degrees over a radiolucent triangle
- Slight internal rotation of the limb
- Radiolucent table essential for fluoroscopy
- Tourniquet optional but commonly used
CPN protection
- Wraps around the fibular neck 1-2 cm distal to the head
- Identify early, before any deep retraction
- Vessel loop or tape sling for protection
- No metal retractors directly on the nerve
- Document ankle dorsiflexion pre- and post-operatively
Internervous plane and dissection
- Subperiosteal elevation of the anterior compartment (tibialis anterior)
- No true intermuscular plane is developed
- Stay anterior to the fibular head and LCL
- Stop distal elevation at about 5 cm to protect the anterior tibial artery
- Submeniscal arthrotomy for articular visualisation
Danger structures
- CPN at the fibular neck — foot drop if injured
- Anterior tibial artery 5-7 cm distal to the joint line
- Deep peroneal nerve with the anterior tibial vessels
- Lateral meniscus — repair if arthrotomy performed
- Recurrent genicular vessels — may require ligation
Buttress plate principle
- Lateral fragment displaces with valgus and axial load
- Buttress plate on the anterolateral surface prevents displacement
- 3.5 mm T-plate, L-plate or anatomic lateral plate
- Screws directed medially and posteriorly
- Goal is less than 2 mm articular step-off
Closure and aftercare
- Repair the coronary ligament (submeniscal arthrotomy) with absorbable suture
- Close the anterior compartment fascia loosely
- Hinged knee brace locked in extension initially
- Non-weight-bearing or toe-touch for 6-8 weeks
- Early ROM once the wound is stable
References
Guidelines, registries & global practice. - Epidemiology: lateral tibial plateau fractures account for about 55-65 percent of all tibial plateau fractures worldwide; high-energy mechanisms predominate in younger patients and low-energy falls in the elderly osteoporotic population. The anterolateral approach is the most commonly performed surgical approach for tibial plateau fractures globally.
- AO Foundation / OTA: CT-based three-column analysis for all tibial plateau fractures; anterolateral approach indicated for lateral column involvement with step-off greater than 2 mm or condylar widening greater than 5 mm.
- BOAST (British Orthopaedic Association): soft-tissue assessment (wrinkle test) before definitive fixation; staged management with an external fixator if the soft tissues are compromised.
- AAOS Appropriate Use Criteria: operative fixation for displaced lateral plateau fractures in active patients; non-operative management acceptable for non-displaced fractures or low-demand patients.
- EFORT / European consensus: anatomic reduction (less than 2 mm step-off) and stable fixation to prevent post-traumatic arthritis; buttress plating for split-depression patterns.
- Registry evidence: the NJR (UK), AJRR (US) and AOANJRR (Australia) each show that malreduction increases later arthroplasty risk, with post-traumatic OA after tibial plateau fracture leading to arthroplasty in about 5-8 percent of patients within 10 years; anatomic reduction at index surgery reduces that risk.
Impact of CT scan on treatment plan and fracture classification of tibial plateau fractures
- CT changed classification in 26 percent of cases and altered surgical plan in 23 percent compared to plain radiographs alone
Three-column fixation for complex tibial plateau fractures
- Three-column fixation improves stability and outcomes in complex tibial plateau fractures involving multiple columns
Posterolateral vs. anterolateral approach for posterolateral tibial plateau fractures: A multicenter cohort with four-year outcomes
- Anterolateral approach for lateral tibial plateau fractures provides good long-term outcomes in multicenter cohort with four-year follow-up
Functional outcomes of severe bicondylar tibial plateau fractures treated with dual incisions and medial and lateral plates
- Dual plating through anterolateral and posteromedial approaches achieves good functional outcomes in complex tibial plateau fractures
CT Improves Classification and Surgical Planning for Tibial Plateau Fractures
- CT changed classification in 26 percent of cases and altered surgical plan in 23 percent compared to plain radiographs alone
Anatomic Reduction Critical for Long-Term Outcome in Tibial Plateau Fractures
- Residual articular step-off greater than 2 mm associated with significantly worse long-term functional outcomes and higher rates of post-traumatic arthritis
Three-Column Classification Guides Approach Selection in Complex Tibial Plateau Fractures
- Three-column concept improved understanding of fracture morphology and reduced rate of missed posterior column involvement compared to Schatzker classification alone
Buttress Plating Superior to Non-Buttress Constructs for Split-Depression Patterns
- Lateral buttress plating with submeniscal arthrotomy achieved anatomic reduction in 87 percent of lateral split-depression fractures with low complication rate
Common Peroneal Nerve Injury in Lateral Tibial Plateau Surgery
- CPN injury rate of 3-5 percent during anterolateral approach; most injuries are neurapraxia with recovery within 6-12 months when nerve is identified and protected