Lazy-S incision over the fibular head, mandatory early CPN identification, and strictly subperiosteal deep dissection.
- The common peroneal nerve winds around the fibular neck 1 to 2 cm distal to the fibular head — identify and protect it BEFORE any deep dissection.
- There is no true internervous plane in the superficial layers; the critical plane is the perineural plane around the CPN, after which all dissection is strictly subperiosteal on bone.
- A lazy-S incision is centred over the fibular head with the knee flexed 30 to 40 degrees to relax the nerve and aid exposure.
- The biceps femoris tendon and lateral collateral ligament insert on the fibular head — tag and protect them, and securely reattach if they are released.
- The anterior tibial artery pierces the interosseous membrane 2 to 3 cm distal to the head — staying subperiosteal on the neck protects its origin.
- Document ankle dorsiflexion and eversion before and after surgery; most protected CPN neuropraxias recover within 3 to 6 months.
When & Why
What it exposes. This approach gives direct access to the fibular head, the fibular neck, the common peroneal nerve (CPN) as it winds around the neck, the posterolateral corner (PLC) attachments on the head, and the proximal tibiofibular joint. It is designed around one overriding principle — mandatory early identification and protection of the CPN before any deep bone work. Primary indications. - Common peroneal nerve decompression and neurolysis at the fibular neck (the most common use).
- Fibular head excision for tumour, symptomatic nonunion, or arthritis.
- Posterolateral corner reconstruction — fibular-head tunnel placement and graft passage.
- Proximal tibiofibular joint arthrotomy, stabilisation, or arthrodesis.
- Tumour biopsy or resection involving the proximal fibula with nerve preservation.
- Open reduction and internal fixation of selected proximal fibula fractures, and revision surgery around the fibular head. Why this approach is chosen. The proximal fibula is the site where the CPN is most susceptible to compression and injury. Direct exposure allows safe nerve decompression, secure reattachment of posterolateral corner structures, and access to the fibular head for oncologic or reconstructive procedures, with extensile access proximally along the biceps tendon and distally along the fibular shaft. Contraindications. Active infection over the proposed incision; severe soft-tissue compromise requiring delayed surgery; medical instability precluding positioning; and isolated medial or anterior compartment pathology better addressed through another approach. Alternative approaches. An anterolateral approach to the knee for intra-articular pathology without CPN involvement; a posterolateral approach to the tibia for tibial plateau fractures requiring buttress plating; and a lateral approach to the fibular shaft for mid-shaft fibula fractures or nonunion. Position & landmarks. Supine on a radiolucent table with the knee flexed 30 to 40 degrees over a bolster (this relaxes the CPN and is essential), the hip slightly externally rotated to bring the fibular head forward, and a high thigh tourniquet inflated after draping. Palpate and mark the fibular head (the most prominent lateral landmark), the lateral joint line, the biceps femoris tendon proximally, and the fibular shaft distally; the CPN can often be rolled under a finger as it crosses the fibular neck. The lazy-S incision is centred over the fibular head: the proximal limb curves posteriorly along the biceps tendon and the distal limb runs along the posterior border of the fibular shaft, totalling 6 to 8 cm and extendable in either direction. Document dorsiflexion and eversion before draping.
The Exposure
The exposure is built around the nerve. First understand the regional anatomy, then find and protect the CPN, and only then perform strictly subperiosteal dissection on the fibular neck and head.
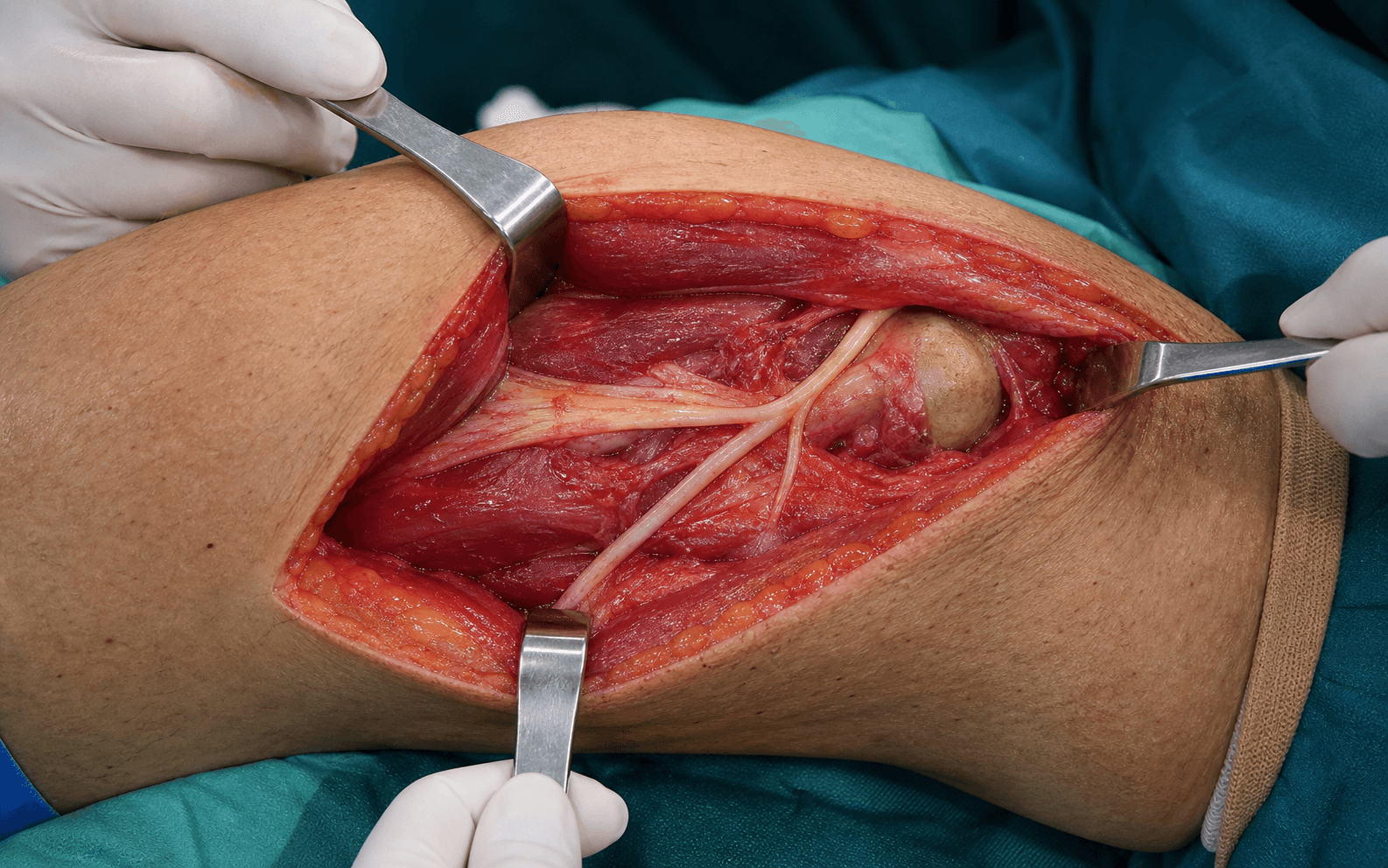
Regional anatomy that dictates the technique. - The CPN (L4-S2) courses along the posterior border of the biceps femoris, then winds laterally around the fibular neck 1 to 2 cm distal to the fibular head, and divides into the deep and superficial peroneal nerves within the peroneal compartment. Before reaching the neck it lies superficial to the lateral head of gastrocnemius and deep to the biceps.
- The anterior tibial artery arises from the popliteal artery at the lower border of popliteus and passes forward through the interosseous membrane about 2 to 3 cm distal to the fibular head — the structure most at risk from anterior or blind dissection.
- The biceps femoris tendon and the lateral collateral ligament both insert on the fibular head; the peroneus longus originates from the proximal fibula and lateral tibial condyle, and the soleus has a proximal origin from the fibular head and posterior tibia.
Exposure sequence
- Supine with the knee flexed 30 to 40 degrees over a bolster and the hip slightly externally rotated; high thigh tourniquet.
- Mark the fibular head, biceps tendon and fibular shaft, and confirm the CPN by palpation across the neck.
- Incise a lazy-S centred on the fibular head — the proximal limb along the biceps tendon, the distal limb along the posterior border of the fibular shaft (6 to 8 cm).
- Incise skin and subcutaneous tissue along the marked line; identify and preserve any branches of the lateral sural cutaneous nerve encountered to avoid lateral-calf numbness.
- Expose the fascia over the peroneal compartment and the biceps femoris tendon insertion onto the fibular head.
- Palpate the CPN as it crosses the fibular neck; make a small window in the fascia and carefully identify the nerve proximal to the compression site first.
- Pass a vessel loop or silicone tape around it for gentle retraction.
- No metal or self-retaining retractors on the nerve; keep the knee flexed and release retraction periodically (about every 20 minutes).
- Incise the fascia over the peroneal compartment distal to the nerve and mobilise the CPN gently proximally and distally.
- For decompression, release all compressive bands at the fibular neck and carry the release distally into the peroneal tunnel so decompression is complete.
- With the nerve protected, use a periosteal elevator to elevate directly off the fibular neck and head, staying strictly subperiosteal — this protects the anterior tibial vessels at the interosseous membrane.
- At the fibular head, tag the biceps femoris tendon and LCL; partially release them only if full head exposure is required, for later secure reattachment. Avoid blind posterior dissection.
- Perform the intended work — nerve decompression, fibular head excision, PLC tunnel drilling, or proximal tibiofibular joint arthrotomy.
- Reattach the biceps and LCL to the fibular head or remaining neck with heavy non-absorbable suture through bone tunnels or anchors; close the peroneal fascia loosely to avoid compartment syndrome.
- Confirm the CPN is free of tension and not compressed by tissue or hardware, and document ankle dorsiflexion and great-toe extension before waking the patient.
The common peroneal nerve winds around the fibular neck only 1 to 2 cm distal to the head and is the structure most often injured in this approach; a palsy causes foot drop with loss of ankle dorsiflexion and toe extension. Prevention is the whole technique: palpate and mark the nerve before incision, identify it proximal to the pathology under direct vision, sling it with a vessel loop, keep the knee flexed to relax it, never place metal or self-retaining retractors on it, and release retraction every 20 minutes. Document dorsiflexion and eversion pre- and post-operatively.
This approach does not exploit a true internervous plane between two muscles. Instead the critical plane is the perineural plane around the common peroneal nerve; once the nerve is identified and slung, all further dissection is subperiosteal on bone. This minimises risk to the anterior tibial artery origin and the peroneal artery branches, and the biceps femoris tendon may be partially released for exposure but must be securely reattached.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Lateral sural cutaneous nerve
- Protection strategy
- Identify and preserve if encountered; usually not functionally significant if divided
- Structure at risk
- Common peroneal nerve (1-2 cm distal to head)
- Protection strategy
- Identify first proximal to the site; vessel loop; knee flexed; no metal or self-retaining retractors; release every 20 min
- Structure at risk
- Biceps femoris tendon and LCL
- Protection strategy
- Tag and protect; if released, reattach with heavy non-absorbable suture through bone tunnels or anchors to prevent varus laxity
- Structure at risk
- Anterior tibial artery origin through interosseous membrane
- Protection strategy
- Strictly subperiosteal dissection along the fibular neck; no blind anterior or posterior dissection
- Structure at risk
- Peroneal artery branches
- Protection strategy
- Usually avoided by the subperiosteal plane; ligate small branches only, repair major injury
Extensile options. Extend proximally along the posterior border of the biceps femoris tendon to reach the posterolateral capsule and popliteal fossa for more extensive PLC reconstruction. Extend distally along the posterior border of the fibular shaft to access the proximal fibular diaphysis for longer plate fixation or more distal nerve exploration. Closure. Reattach the biceps femoris and LCL to the fibular head with heavy non-absorbable suture if detached; close the peroneal compartment fascia loosely to avoid compartment syndrome; approximate subcutaneous tissue and close skin with staples or interrupted sutures. Apply a knee brace in slight flexion. CPN injury management. If the nerve is transected intra-operatively, perform primary repair or a nerve graft for a gap; for post-operative foot drop, manage with an ankle-foot orthosis, physiotherapy, and serial nerve-conduction studies. Most neuropraxias recover within 3 to 6 months and axonotmesis within 6 to 12 months; explore if there is no recovery by 3 months with positive EMG changes.
Procedures Through This Approach
- Common peroneal nerve decompression — nerve exploration and release at the fibular neck; the principal operation through this exposure.
- Fibular head excision for tumour (e.g. osteochondroma), symptomatic nonunion, or arthritis, with preservation and reattachment of posterolateral corner structures.
- Posterolateral corner reconstruction — fibular-head tunnel drilling (anterior-to-posterior) and graft passage for chronic posterolateral rotatory instability.
- Proximal tibiofibular joint arthrotomy, stabilisation, or arthrodesis.
- Tumour biopsy or resection with appropriate margins, and ORIF of selected proximal fibula fractures.
Viva & Exam Focus
FIBULAFIBULA — the proximal fibula approach, step by step
CPN SAFECPN SAFE — protecting the common peroneal nerve
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man presents with foot drop three months after a knee dislocation. Nerve conduction studies show compression of the common peroneal nerve at the fibular neck. Describe your surgical approach for decompression.”
“A 22-year-old woman has a biopsy-proven osteochondroma of the fibular head causing common peroneal nerve irritation. Describe your approach for excision.”
“A 28-year-old athlete has chronic posterolateral rotatory instability after a knee injury, with MRI confirmation of a PLC injury. Describe the surgical approach for anatomic reconstruction.”
Patient position
- Supine with knee flexed 30-40 degrees over a bolster
- Hip slightly externally rotated to expose the fibular head
- Tourniquet high on the thigh; radiolucent table
- Document dorsiflexion and eversion before and after
CPN protection sequence
- Palpate and mark the nerve before incision
- Identify it proximal to the fibular neck first
- Place a vessel loop or tape sling immediately
- No metal or self-retaining retractors on the nerve
- Release retractors about every 20 minutes
- Keep the knee flexed to reduce nerve tension
Incision and superficial dissection
- Lazy-S incision centred over the fibular head
- Preserve lateral sural cutaneous nerve branches
- Expose the biceps femoris tendon insertion
- Incise the fascia over the peroneal compartment
- Identify the CPN before any deep retraction
Deep dissection and dangers
- Subperiosteal elevation along the fibular neck
- Tag the biceps femoris and LCL for reattachment
- Protect the anterior tibial artery at the interosseous membrane
- Ligate small peroneal artery branches only
- Stay on bone to avoid neurovascular injury
Extension and procedures
- Proximal: along the biceps tendon into the popliteal fossa
- Distal: along the posterior fibular shaft
- CPN decompression at the fibular neck
- Fibular head excision or tumour resection
- PLC reconstruction tunnel placement
- Proximal tibiofibular joint procedures
Closure and aftercare
- Reattach the biceps and LCL with heavy non-absorbable suture
- Close the fascia loosely to avoid compartment syndrome
- Confirm the nerve is free of tension before closure
- Document dorsiflexion under anaesthetic
- Early ankle dorsiflexion exercises; knee brace in slight flexion
References
Anatomic variations related to decompression of the common peroneal nerve at the fibular head
- Anatomic study defining variations in the CPN course at the fibular head that are critical for safe surgical decompression and exposure
The anatomical relationship of the common peroneal nerve to the proximal fibula and its clinical significance when performing fibular-based posterolateral reconstructions
- Cadaveric study quantifying the CPN position relative to proximal fibular landmarks for safe tunnel placement in PLC reconstruction
Peroneal Nerve Palsy: Evaluation and Management
- Comprehensive review of peroneal nerve palsy including anatomy at the fibular head, evaluation, and surgical management principles
Outcomes of treatment of acute grade-III isolated and combined posterolateral knee injuries: a prospective case series and surgical technique
- Prospective study of surgical technique and outcomes for PLC injuries using fibular-head-based reconstructions, with emphasis on nerve protection