Lateral oblique incision | Sural nerve protection | Posterior facet exposure
- The oblique Ollier incision runs over the sinus tarsi between the peroneal tendons and extensor digitorum brevis (EDB).
- The sural nerve must be identified in the subcutaneous plane, posterior to the peroneal tendons, before any deep dissection.
- The working interval is between the peroneal tendons (superficial peroneal nerve) and EDB (deep peroneal nerve) — retract the peroneals plantarward and elevate EDB dorsally.
- Clearing the sinus tarsi fat pad reveals the posterior facet, which slopes 30–40 degrees from posterolateral to anteromedial.
- The approach gives no access to medial structures — a separate medial incision is required for triple arthrodesis.
When & Why
What it exposes. The sinus tarsi (Ollier) approach gives direct lateral access to the subtalar (talocalcaneal) joint, particularly the posterior facet, the sinus tarsi and the middle/anterior facets, without violating the peroneal tendon sheath. It is the workhorse exposure for subtalar arthrodesis, tarsal coalition resection and selected calcaneal fracture ORIF. Why this approach is chosen. It provides excellent visualisation of the posterior facet for joint-surface preparation in arthrodesis and access to the sinus tarsi contents for coalition excision or osteochondral lesion work, while minimising soft-tissue disruption compared with the extensile lateral approach. For displaced intra-articular calcaneal fractures it achieves comparable reduction quality for most Sanders II/III patterns with a significantly lower wound-complication rate. Primary indications: - Subtalar arthrodesis (isolated talocalcaneal fusion)
- Tarsal coalition resection (calcaneonavicular or talocalcaneal bars)
- Calcaneal fracture ORIF (selected Sanders II/III via sinus tarsi or extensile lateral)
- Osteochondral lesions of the talar posterior facet or subtalar joint
- Subtalar joint debridement or loose-body removal
- Triple arthrodesis (combined with a medial approach) Contraindications: - Active infection over the lateral hindfoot
- Severe scarring from previous lateral incisions (consider an alternative)
- Isolated medial pathology requiring a medial approach only
- Patient factors precluding non-weight-bearing (compliance issues) Alternative approaches. A medial approach is used for isolated middle-facet coalition or medial talocalcaneal pathology; a posterior approach gives posterior subtalar access in selected cases; arthroscopic subtalar arthrodesis is a minimally invasive option with limited visualisation; and the extensile lateral approach provides broad exposure for complex calcaneal fractures. Approach variants.
Oblique incision over the sinus tarsi between the peronei and EDB. The default exposure for subtalar arthrodesis and coalition resection.
Extended L-shaped incision for the calcaneus. Used for calcaneal ORIF and complex fractures, at the cost of higher wound risk (10–20 percent).
Add a medial utility incision for triple arthrodesis, giving access to the talonavicular joint, middle facet and sustentaculum.
Position & landmarks. Supine with a sandbag or bump under the ipsilateral hip to internally rotate the foot, the knee slightly flexed over a bolster to relax the gastrocnemius, and the foot plantigrade or slightly plantarflexed. Apply a thigh tourniquet (250–300 mmHg after exsanguination) and confirm fluoroscopy for lateral, Broden and axial heel views. Palpate and mark the tip of the lateral malleolus, the sinus tarsi depression (anteroinferior to the malleolus), the anterior process of the calcaneus, the base of the fourth metatarsal and the peroneal tubercle; mark the peroneal tendon course and the sural nerve.
The Exposure
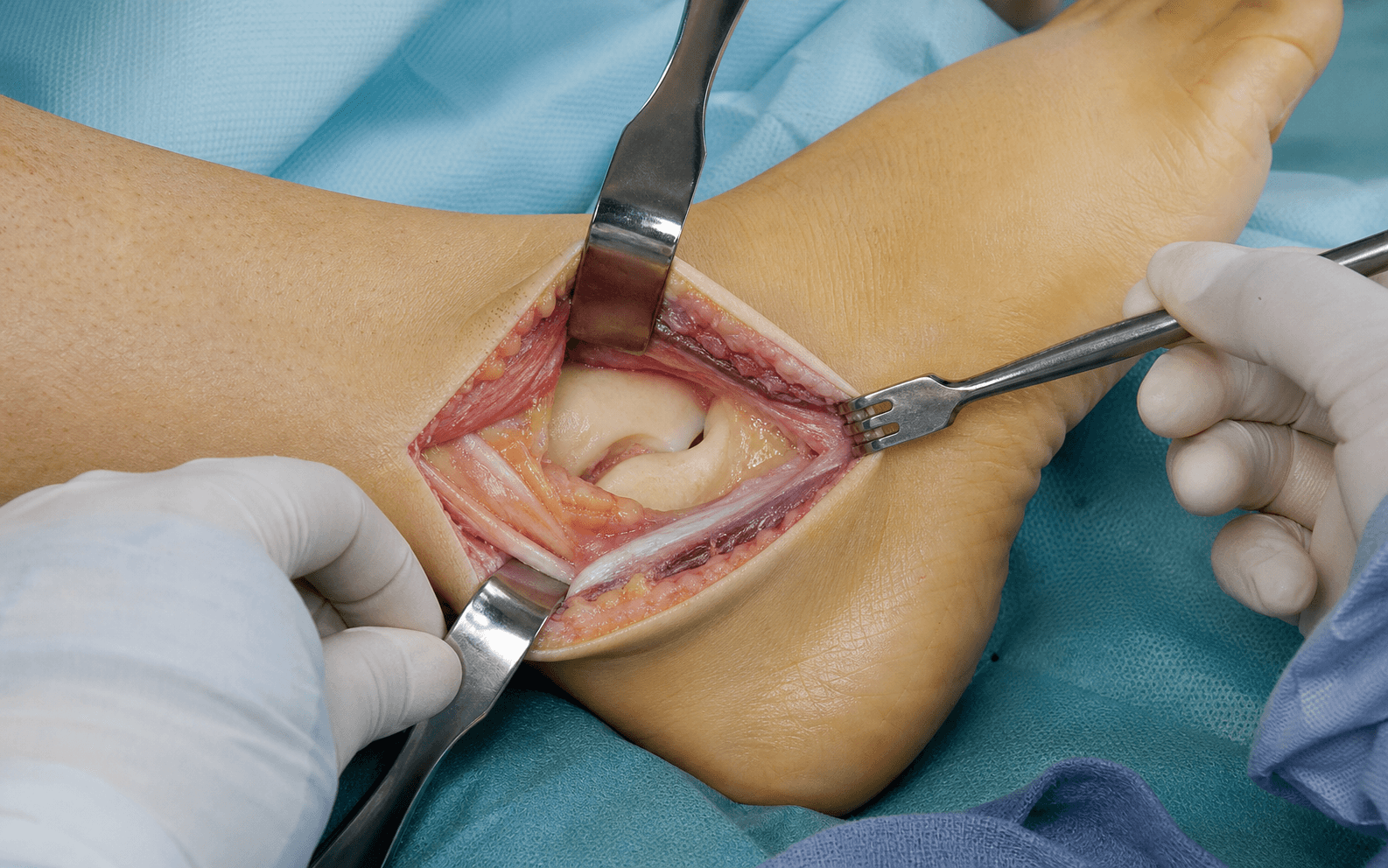
Work down through the layers along the oblique Ollier line — protecting the sural nerve, then developing the interval between the peroneal tendons and EDB to reach the posterior facet of the subtalar joint.
Sinus tarsi exposure sequence
- Supine with a bump under the ipsilateral hip to internally rotate the foot; knee slightly flexed; thigh tourniquet inflated to 250–300 mmHg after exsanguination.
- Mark the tip of the lateral malleolus, the sinus tarsi, the anterior process of the calcaneus and the base of the fourth metatarsal; mark the peroneal tendons and sural nerve.
- Make a 3–5 cm oblique (Ollier) incision from 1 cm distal to the lateral malleolus tip toward the base of the fourth metatarsal, centred over the sinus tarsi.
- Carefully incise skin and subcutaneous tissue; the sural nerve lies in the subcutaneous fat posterior to the peroneal tendons — identify it before any deep work.
- Pass a vessel loop around it for gentle retraction; the lateral calcaneal artery runs with it and may be ligated if bleeding.
- Never place metal retractors directly on the nerve, avoid tight kinking, and document lateral foot sensation before and after.
- Incise the fascia over the peroneal sheath and the EDB origin in line with the skin incision; do not violate the peroneal tendon sheath.
- The working interval lies between the peroneal tendons (superficial peroneal nerve) plantarward and the extensor digitorum brevis (deep peroneal nerve) dorsally — an intermuscular rather than strictly internervous plane.
- Retract the peroneus longus and brevis as a unit, plantarward, with a Langenbeck or Hohmann retractor, preserving the sheath.
- Avoid over-retraction, which causes tendon subluxation, tenosynovitis or superficial peroneal nerve neurapraxia.
- Identify the EDB origin from the sinus tarsi and anterior calcaneal process; elevate it subperiosteally, lateral to medial, with a periosteal elevator.
- Reflect the muscle dorsally and hold it with stay sutures or self-retaining retractors; avoid crushing or bipolar cautery on the belly to preserve its deep peroneal innervation.
- Excise the sinus tarsi fat pad and synovium to expose the posterior facet, which lies immediately posterior and plantar to the sinus tarsi.
- The sinus contains the cervical ligament (talar neck to calcaneal anterior process) and the interosseous talocalcaneal ligament deep in the tarsal canal — divide these deliberately during arthrodesis.
- Incise the capsule parallel to the posterior facet; the facet slopes 30–40 degrees from posterolateral to anteromedial and is best seen with the foot in slight eversion and plantarflexion.
- For arthrodesis, prepare the surfaces to bleeding subchondral bone with curettes, osteotomes or burr; for coalition resection, excise the bar completely while protecting the posterior tibial and flexor hallucis longus tendons medially.
- Irrigate, achieve haemostasis, and let the EDB fall back or loosely approximate it; close the fascia where possible, then the subcutaneous layer and skin without tension.
- For extensile approaches, place a drain exiting posteriorly away from the corner; apply a posterior splint or short-leg cast with the ankle in neutral.
The sural nerve is the structure most often injured in lateral hindfoot approaches. Sural nerve injury or neuroma occurs in 5–15 percent of cases depending on the series; most patients tolerate lateral foot numbness, but a painful neuroma can be debilitating. Identify the nerve in the subcutaneous plane before any deep dissection, retract it gently on a vessel loop, never apply metal retractors directly to it, and release retraction regularly. Careful handling reduces permanent symptomatic injury to less than 5 percent.
The sinus tarsi approach is an intermuscular rather than strictly internervous dissection. The peroneal tendons are retracted as a unit without violating their sheath, and the EDB is elevated from its calcaneal origin rather than split — so neither muscle group is denervated, while still giving excellent exposure of the posterior facet.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Sural nerve (posterior to the peroneals)
- Protection
- Identify before deep dissection; vessel loop; no metal retractors; release regularly
- Structure at risk
- Lateral calcaneal artery (runs with the sural nerve)
- Protection
- Preserve for flap perfusion; ligate cleanly only if bleeding
- Structure at risk
- Peroneal tendons (longus and brevis)
- Protection
- Protect the sheath; retract plantarward as a unit; avoid over-retraction
- Structure at risk
- Extensor digitorum brevis
- Protection
- Subperiosteal elevation lateral-to-medial; stay sutures; avoid crushing
- Structure at risk
- Posterior facet cartilage
- Protection
- Protect during joint preparation; careful instrumentation; confirm on fluoroscopy
- Structure at risk
- Superficial peroneal nerve branches
- Protection
- Identify during proximal extension; avoid tight retraction; document sensation
Sural nerve injury management. - Intra-operative clean transection: primary repair; if the proximal end cannot be saved, bury it in muscle to prevent neuroma.
- Suspected neurapraxia: observe, document and follow up closely.
- Established painful neuroma: desensitisation and local steroid injection; if refractory, surgical excision with proximal-stump burial. Extensile options. - Proximal extension along the posterior border of the fibula reaches the lateral ankle and peroneal tendons; the sural nerve becomes more superficial proximally, increasing risk.
- Distal extension toward the fourth-metatarsal base or a dorsal limb reaches the talonavicular joint for triple arthrodesis, and may need a separate medial incision.
- Extensile lateral (L-shaped) adds a vertical limb along the posterior calcaneal border for broad calcaneal exposure in Sanders II–IV fractures; the corner must be handled carefully to avoid wound-edge necrosis, the sural nerve is mobilised with the posterior flap, and the peroneals are exposed and protected throughout.
- Combined medial approach for triple arthrodesis exposes the talonavicular joint, middle facet and sustentaculum while protecting the posterior tibial tendon and neurovascular bundle, allowing complete preparation of all three joints. Closure. Irrigate and achieve haemostasis; let the EDB fall back or loosely approximate it, close the fascia where possible, approximate subcutaneous tissue and close skin with interrupted nylon or staples without tension. Apply a sterile dressing and a posterior splint or short-leg cast.
- Rate
- 5–10%
- Prevention and management
- Careful nerve handling reduces symptomatic injury to less than 5 percent; desensitisation, injection, or excision and burial if refractory
- Rate
- 10–20%
- Prevention and management
- Sinus tarsi approach is significantly lower; handle the corner carefully; local wound care to flap coverage
- Rate
- 5–15%
- Prevention and management
- Higher in smokers; good joint preparation, stable fixation and bone graft; revision arthrodesis with autograft
- Rate
- 5–8%
- Prevention and management
- Protect the sheath and ensure smooth gliding post-op; NSAIDs and physiotherapy
- Rate
- 2–5%
- Prevention and management
- Higher with extensile approach and poor soft tissues; irrigation and debridement, antibiotics, possible hardware removal
- Rate
- 10–20%
- Prevention and management
- Accurate diagnosis and realistic expectations; pain management or revision
Post-operative care. Check and document lateral foot sensation (sural nerve function) and inspect the wound; apply a posterior splint or short-leg cast with the ankle neutral and elevate the limb above heart level for 48–72 hours, with DVT prophylaxis per protocol. Keep the patient non-weight-bearing for 6–12 weeks depending on the procedure (arthrodesis versus ORIF), progressing on radiographic healing. Follow up at 2 weeks (wound check, suture removal), 6 weeks (lateral, Broden and axial radiographs), 12 weeks (confirm union, progress weight-bearing) and 6–12 months for functional review.
Procedures Through This Approach
- Subtalar arthrodesis — isolated talocalcaneal fusion; fix with 2–3 large cannulated screws (6.5 or 7.3 mm) from the posterior calcaneus into the talar body.
- Triple arthrodesis — combined with a medial approach to the talonavicular and calcaneocuboid joints.
- Tarsal coalition resection — calcaneonavicular or talocalcaneal bars, with fat or muscle interposition to prevent recurrence.
- Calcaneal fracture ORIF — sinus tarsi or extensile lateral technique depending on fracture pattern.
- Osteochondral lesion treatment or loose-body removal, and subtalar joint debridement or synovectomy.
Viva & Exam Focus
SINUSTARSISINUS TARSI — the exposure step by step
Hook:SINUS TARSI approach — protect the sural nerve and expose the posterior facet.
SURALSURAL — nerve protection principles
Hook:The sural nerve is the most important structure at risk — keep it protected.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old labourer with post-traumatic subtalar arthritis after a calcaneal fracture presents for surgical consideration. CT confirms isolated subtalar joint arthritis with preserved talonavicular and calcaneocuboid joints. Describe your surgical approach.”
“A 14-year-old with a symptomatic calcaneonavicular tarsal coalition fails conservative management. Describe the surgical approach for coalition resection.”
“A 35-year-old with a displaced Sanders III calcaneal fracture presents 10 days after injury with significant lateral swelling but intact skin wrinkles posteriorly. How would you decide between the sinus tarsi and extensile lateral approach?”
Position and incision
- Supine with ipsilateral hip bump for internal rotation
- Oblique Ollier incision: 1 cm distal to lateral malleolus to fourth-MT base
- Length 3–5 cm centred over the sinus tarsi
- For extensile: add a vertical limb along the posterior calcaneus
- Mark the sural nerve and peroneal tendons pre-operatively
Sural nerve protection
- Identify in subcutaneous tissue posterior to the peroneal tendons
- Gentle vessel-loop retraction
- No metal retractors directly on the nerve
- Avoid tight kinking or prolonged stretch
- Document lateral foot sensation before and after
Internervous plane and dissection
- Between peroneal tendons (superficial peroneal) and EDB (deep peroneal)
- Retract the peroneal tendons plantarward as a unit
- Elevate EDB subperiosteally from its calcaneal origin
- Remove the sinus tarsi fat pad for posterior-facet exposure
- Incise capsule parallel to the posterior-facet joint line
Danger structures by layer
- Subcutaneous: sural nerve and lateral calcaneal artery
- Fascial: peroneal tendon sheath — protect and retract as a unit
- Muscular: EDB — elevate gently, preserve innervation
- Articular: posterior facet cartilage — protect during preparation
- Ligamentous: cervical and interosseous ligaments — divide deliberately
Procedures and extension
- Subtalar arthrodesis: 2–3 large cannulated screws from posterior calcaneus
- Coalition resection: excise the bar completely, interpose a fat graft
- Calcaneal ORIF: sinus tarsi or extensile lateral based on the fracture
- Proximal extension: along the posterior fibula for ankle access
- Combined medial: for triple arthrodesis (TN and middle facet)
Complications and outcomes
- Sural neuroma: 5–10 percent — careful handling reduces to less than 5 percent
- Wound necrosis (extensile): 10–20 percent — sinus tarsi significantly lower
- Subtalar nonunion: 5–15 percent — higher in smokers, needs good preparation
- Peroneal tendinitis: 5–8 percent — protect the sheath, ensure smooth gliding
- Infection: 2–5 percent — higher with extensile approach and poor soft tissues
References
Implant Choice and Outcomes of the Sinus Tarsi Approach for Displaced Intra-articular Calcaneal Fractures
- The sinus tarsi approach allows good visualization and stable fixation with low wound complication rates in displaced intra-articular calcaneal fractures
Modified sinus tarsi approach with a variable-angle locking anterolateral plate for Sanders type II and III calcaneal fractures
- Modified sinus tarsi approach with locking plate achieves excellent reduction and low complication rates for Sanders II/III calcaneal fractures
Increased Lateral Calcaneal Body and Subtalar Joint Visualization Utilizing a Modified Sinus Tarsi Approach
- A modified sinus tarsi approach significantly improves visualization of the lateral calcaneal body and subtalar joint
Complication and Revision Rate in Complex Intraarticular Calcaneal Fractures: Extended Lateral vs Sinus Tarsi Approach
- The sinus tarsi approach demonstrates significantly lower complication and revision rates compared to the extended lateral approach in complex calcaneal fractures