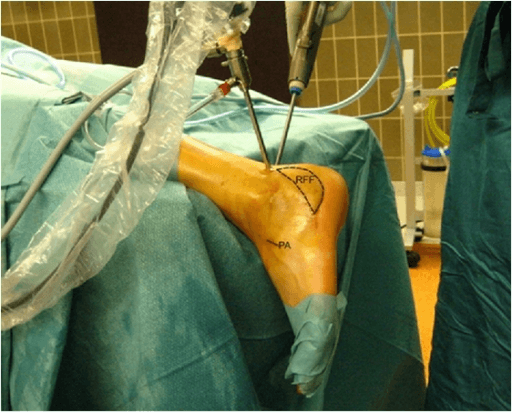
Isolated subtalar joint fusion through a lateral sinus tarsi approach · the heel-alignment operation
- Heel position is the single most critical technical decision: 0–5° valgus with neutral dorsiflexion and plantarflexion prevents lateral or medial border overload, peroneal and posterior tibial tendon overload, and abnormal loading of the ipsilateral knee
- Post-traumatic subtalar osteoarthritis following a displaced intra-articular calcaneal fracture is the most common indication; arthrodesis is the standard of care for end-stage disease after at least 3–6 months of failed conservative management
- Non-union occurs in roughly 5–16% of primary isolated fusions and is markedly higher in smokers and where avascular bone is present — in Easley's series union fell from 92% in non-smokers to 73% in smokers, and every non-union occurred where greater than 2 mm of avascular bone was present
- The talonavicular and calcaneocuboid joints must be carefully protected during cartilage preparation; progressive adjacent joint arthrosis is a major long-term concern and may ultimately require conversion to triple arthrodesis
- Isolated subtalar fusion preserves useful transverse tarsal motion (reduced by about 40%, not abolished) and is preferred over triple arthrodesis whenever the talonavicular and calcaneocuboid joints are spared
When & Why
Indication. Symptomatic, end-stage subtalar osteoarthritis — lateral hindfoot pain, stiffness and functional limitation that has failed at least 3–6 months of conservative care (orthotics or insoles, activity modification, NSAIDs, and at least one image-guided corticosteroid injection into the subtalar joint) — with the talonavicular and calcaneocuboid joints preserved on weight-bearing radiographs and CT. When those adjacent joints are also arthritic, a triple arthrodesis is preferred instead. The operation is chosen for five broad indication groups. In every case the decision to fuse only the subtalar joint (rather than extend to a triple fusion) rests on confirming the talonavicular and calcaneocuboid joints are clinically and radiographically preserved.
The most common indication worldwide. Displaced intra-articular calcaneal fractures destroy posterior facet cartilage in a substantial proportion of patients; Sanders Type III and IV fractures carry the highest risk. May be combined with lateral wall exostectomy or calcaneal osteotomy at malunion correction.
Less common; older patients with insidious hindfoot pain. Confirm on weight-bearing radiographs (Harris-Heath axial and lateral views) and CT, with preserved adjacent joints.
Resection is preferred in the young before secondary OA, but arthrodesis is appropriate when the coalition involves more than 50% of the posterior facet, when severe secondary OA follows failed resection, or when an adult presents with established OA.
Stage IIB/C with fixed subtalar valgus and secondary arthrosis, combined with medial column procedures when the talonavicular joint is preserved. Stage III or IV disease is a triple arthrodesis instead.
Rheumatoid arthritis or seronegative spondyloarthropathy isolated to the subtalar joint and refractory to systemic management. Optimise wound healing and co-ordinate immunosuppressant dose reduction with the rheumatologist peri-operatively.
Secondary subtalar arthrosis from talar AVN. Fusion gives pain relief and stability; the extent of AVN and tibiotalar involvement decides between isolated fusion, total ankle replacement, or tibiotalocalcaneal fusion.
Contraindications. Active infection (absolute); subtalar pain not attributable to subtalar OA with preserved cartilage; significant talonavicular or calcaneocuboid OA (triple arthrodesis instead); peripheral arterial disease with critical ischaemia (relative — vascular opinion first); and severe osteoporosis (relative — plan augmented fixation). Consent specifically for sural nerve injury or a painful lateral-foot neuroma (the most common neurological complication, 5–15%), wound dehiscence or infection (higher in post-traumatic cases with prior scars and in inflammatory arthritis), non-union (5–16%, higher in smokers and diabetics), heel malposition requiring revision, and the realistic long-term risk of symptomatic adjacent joint arthrosis that may need conversion to triple arthrodesis. Setup. Lateral decubitus with the operative foot uppermost (excellent sinus tarsi access and easy fluoroscopy), or prone with both feet hanging over the table edge. Thigh or calf tourniquet for a bloodless field during cartilage preparation. C-arm available for lateral and Harris-Heath axial hindfoot views throughout.
The Operation
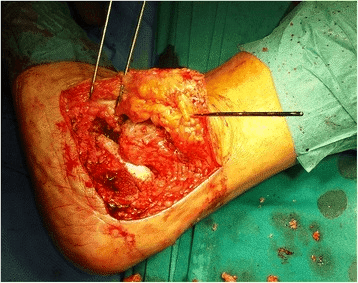
The goal is to expose the subtalar joint through the lateral sinus tarsi approach, remove all articular cartilage from the posterior and anterior-middle facets down to bleeding cancellous bone while protecting the sural nerve, the peroneal tendons and the medial neurovascular bundle, position the heel in 0–5° valgus, and compress the prepared surfaces with one or two large cannulated screws. The exposure is laid out in full below (and in depth on the sinus tarsi approach to the subtalar joint page).

Operative sequence
- Lateral decubitus, operative foot uppermost; thigh or calf tourniquet; C-arm set for lateral and Harris-Heath axial views.
- Palpate the tip of the lateral malleolus and the base of the fourth metatarsal — these bracket the sinus tarsi.
- A 4–5 cm longitudinal incision centred over the sinus tarsi, running from the tip of the lateral malleolus toward the base of the fourth metatarsal.
- Mark the sural nerve course on the skin before incision — it crosses the posterosuperior aspect of the wound and is most easily injured in the first 2 cm of dissection.
- Identify and vessel-loop the sural nerve early. It is formed from the medial sural cutaneous (tibial) and lateral sural cutaneous (common peroneal) nerves, lies about 1–2 cm posterior to the lateral malleolus, and crosses the peroneal tendons and lateral calcaneal wall toward the fifth metatarsal base.
- Identify the peroneal tendon sheath (peroneus brevis and longus in the groove behind the lateral malleolus) and retract it inferiorly. Do not enter the sheath unless tendon pathology needs inspection — peroneal tendon disease is common in calcaneal fracture sequelae and should be assessed at surgery.
- Incise the extensor retinaculum and open the sinus tarsi.
- Excise the fat pad, the cervical ligament (most lateral, connecting the sinus tarsi roof to the calcaneus) and the interosseous talocalcaneal ligament (ITCL) — the strongest intra-articular ligament, running obliquely in the canalis tarsi, which must be divided to open the joint. Cauterise the small artery of the sinus tarsi (a branch of the perforating peroneal).
- This fully exposes the posterior facet (the largest facet; convex calcaneal surface articulating with the concave talar facet, oriented obliquely postero-lateral to antero-medial, and the primary joint fused) and the anterior-middle facet complex (the middle facet sits on the sustentaculum tali medially).
- Place a small Hohmann retractor around the talar neck superiorly and the calcaneal body inferiorly to distract the joint. Confirm the visible anatomy matches the pre-operative CT.
- Remove all remaining articular cartilage from both the talar and calcaneal surfaces of the posterior facet using curved curettes (working in all directions), narrow osteotomes to lift the subchondral plate, and a high-speed burr for eburnated bone.
- The goal is bleeding cancellous bone on both surfaces. Preserve subchondral bone depth — removing excessive bone shortens the heel.
- The talar surface is harder to reach; use longer curved curettes and confirm completeness by palpation and direct vision. Incomplete cartilage removal is a recognised cause of non-union.
- Use narrow curettes through the sinus tarsi to access the anterior and middle facets; remove accessible cartilage and decorticate the surfaces.
- The middle facet on the sustentaculum tali lies medially — avoid excessive medial instrumentation to protect the medial neurovascular bundle (posterior tibial artery and tibial nerve) in the tarsal tunnel.
- Confirm instrument depth on fluoroscopy. Instruments passing beyond the anterior-medial margin of the sinus tarsi risk entering the talonavicular joint — fluoroscopic confirmation is mandatory.
- Bone graft is used for significant bone loss from calcaneal fracture collapse, talar AVN with cystic change, revision for non-union, or surgeon preference to augment fusion biology.
- Options: autograft (iliac crest is the gold standard for non-union; local lateral-wall calcaneal cancellous bone avoids donor morbidity), allograft cancellous chips for void fill, or a bone substitute (calcium phosphate, demineralised bone matrix).
- Pack the graft into the prepared joint space only after confirming alignment.
- Target: heel 0–5° valgus relative to the tibial axis, with neutral dorsiflexion and plantarflexion (foot plantigrade) and the forefoot not supinated.
- Confirm clinically — hold the foot in position, simulate weight-bearing (the heel should sit directly under the leg), and compare with the contralateral foot where possible.
- Confirm fluoroscopically — lateral view for tibiotalar and subtalar alignment and a plantigrade foot; Harris-Heath axial view to confirm 0–5° calcaneal valgus.
- Hold the position with one or two 2.0 mm Kirschner guide wires from the plantar heel into the central talar body, parallel and directed from posterior-inferior to central talar body, and re-confirm alignment on fluoroscopy before definitive fixation.
- Standard construct: two large cannulated cancellous screws (6.5–7.3 mm) inserted percutaneously through the plantar heel, directed from the posterior-inferior calcaneus through the posterior facet fusion site into the talar body subchondral bone. Two screws give rotational control; a single 7.3 mm screw can suffice in good-quality bone with well-apposed surfaces (Mann 1998 achieved union in all 48 feet with one or two screws).
- Alternative: a crossed configuration (one screw posterior calcaneus to talar body, one talar neck to calcaneus) for added rotational stability.
- Overdrill the calcaneus to allow glide (compression principle), tap the harder talar body, and compress the surfaces before final tightening. Do not advance threads across the ankle (tibiotalar) joint. Confirm final position on lateral and axial fluoroscopy — no screw in the ankle joint.
- Irrigate copiously, release the tourniquet, and achieve haemostasis with bipolar cautery.
- Ensure the sural nerve is not trapped in the closure. Close the extensor retinaculum with absorbable suture, then a tension-free layered skin closure.
- Apply a soft padded dressing and a below-knee posterior plaster backslab with the foot plantigrade and neutral.
Before any bone work, identify and vessel-loop the sural nerve at the posterosuperior corner of the sinus tarsi incision — it is the most commonly injured structure and a painful lateral-foot neuroma is the most frequent neurological complication. During cartilage preparation, stay lateral to the posterior facet and sustentaculum tali: the posterior tibial artery and tibial nerve run through the tarsal tunnel medial to the sustentaculum, and excessive medial curettage or a medially misdirected K-wire or screw causes catastrophic medial neurovascular injury. Never place retractors or guide wires under the sustentaculum.
Varus malposition creates a rigid supinated hindfoot with lateral border overload, fifth metatarsal and cuboid stress fractures, and peroneal tendon pathology. Valgus beyond 5° overloads the medial midfoot and spring ligament, accelerates talonavicular arthrosis, and drives the knee into valgus. Confirm alignment clinically and fluoroscopically (lateral and Harris-Heath axial) both before and after provisional K-wire insertion — never trust a single view.
Plain radiographs substantially overestimate the percentage of joint fused (Coughlin 2006 found radiographs suggested 86% fusion at six months where CT showed only 64%). When non-union is suspected on persistent pain, obtain a CT rather than relying on serial films.
Critical structures to protect. Five danger zones account for almost all the morbidity of this operation:
Crosses the lateral hindfoot about 1–2 cm posterior to the lateral malleolus, running superficially over the peroneal tendons toward the fifth metatarsal base; most vulnerable at the posterosuperior corner of the incision. Identify and vessel-loop it early; use skin hooks for superficial retraction. Injury causes lateral-foot numbness or a painful neuroma (the most common neurological complication, 5–15%).
The posterior tibial artery and tibial nerve run medial to the sustentaculum tali through the tarsal tunnel. Stay lateral to the posterior facet during bone preparation and never place retractors or K-wires under the sustentaculum. Violation causes catastrophic medial neurovascular injury and compartment syndrome.
Target is 0–5° valgus relative to the tibial axis. Varus creates a rigid supinated hindfoot (lateral border overload, stress fractures, peroneal pathology); excessive valgus overloads the medial midfoot, accelerates talonavicular arthrosis, and drives the knee into valgus. Intra-operative fluoroscopy and clinical heel-alignment checks are mandatory before screw insertion.
Immediately anterior to the subtalar joint; the talonavicular joint is particularly vulnerable to inadvertent curettage when preparing the anterior-middle facets. Use direct vision, avoid aggressive instrumentation beyond the anterior margin of the posterior facet, and confirm joint boundaries on fluoroscopy. Chondral damage accelerates adjacent joint arthrosis and may convert an isolated fusion into a triple fusion.
The sinus tarsi incision passes over the peroneal tendons at the lateral calcaneal wall. Identify the peroneal sheath and retract it inferiorly, and close in layers without tension. Wound dehiscence (3–8%, higher in post-traumatic and inflammatory cases) exposes hardware and risks deep infection; peroneal disruption causes lateral instability and needs separate repair.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0–2 weeks | Below-knee plaster backslab; strict non-weight-bearing; foot elevated above the heart for the first 48–72 hours | Finger and toe active range of motion only; wound check and suture or staple removal at 10–14 days | | 2 | 2–6 weeks | Convert to a fibreglass cast or removable walker boot; remain non-weight-bearing | Ankle dorsiflexion and plantarflexion to prevent tibiotalar stiffness; multimodal analgesia (avoid NSAIDs for six weeks — they impair bone healing) | | 3 | 6–12 weeks | Radiographic review at six weeks; if satisfactory callus, protected weight-bearing in the boot, progressing to full weight-bearing as tolerated | Calf strengthening once full weight-bearing is established; gait re-education for reduced hindfoot motion | | 4 | 3–6 months | Wean from the boot into supportive footwear | Graded return to function; CT at six months if union is in doubt | Most patients return to sedentary work at 6–8 weeks, light duties at 10–12 weeks, and manual labour or prolonged standing at 4–6 months; running and sport resume at 6–12 months depending on union and strength. AOFAS hindfoot scores typically improve from the mid-20s to around 70 (Easley 2000) or 75 (Flemister 2000 for calcaneal-fracture sequelae), with 93% satisfaction (Mann 1998). Patients should be counselled pre-operatively that walking on uneven ground remains difficult: transverse tarsal motion is reduced by about 40%, dorsiflexion by 30%, and plantarflexion by only 9% (Mann 1998) — useful motion is retained, not abolished. Complications
- Recognition
- Persistent hindfoot pain beyond 4–6 months; CT (gold standard) shows no bridging trabeculae; screw lucency or back-out on serial films
- Prevention
- Complete cartilage removal to bleeding bone; two-screw fixation; smoking cessation; HbA1c below 7.5%; avoid NSAIDs for six weeks
- Management
- CT-confirmed non-union: revision with re-preparation of surfaces, iliac crest autograft, improved fixation; address modifiable risk factors first
- Recognition
- Varus: lateral border pain, stress fractures, rigid supination; excessive valgus: medial midfoot pain, knee valgus
- Prevention
- Clinical plus fluoroscopic alignment check before fixation; provisional K-wires; check the forefoot is not supinated; compare with the contralateral foot
- Management
- Mild: lateral-posting orthotic; functionally significant varus: revision osteotomy through the fusion mass and re-fixation (no re-fusion needed if already united)
- Recognition
- Immediate transection; early lateral-foot and fifth-toe numbness or dysaesthesia; late painful neuroma with a positive Tinel at the scar
- Prevention
- Identify and vessel-loop the nerve early; skin hooks for superficial retraction; vigilance at the proximal-superior corner; avoid electrocautery near it
- Management
- Neuropraxia: observe (resolves 6–12 weeks); painful neuroma: desensitisation, gabapentin; persistent at 12 months: excision and burial in EDB; intra-operative transection: primary 8-0 nylon repair
- Recognition
- Progressive midfoot and dorsolateral pain after an initially successful fusion; weight-bearing CT or MRI confirms TN or CC OA; diagnostic injection
- Prevention
- Avoid cartilage damage to TN and CC during preparation; correct heel alignment (valgus malposition accelerates TN arthrosis); counsel patients on long-term risk
- Management
- Conservative first (orthotics, injection); symptomatic progression: triple arthrodesis, extending the original fusion
- Recognition
- Superficial: edge separation, serous drainage; deep: fever, raised CRP or ESR, purulent drainage, hardware involvement; CT or MRI for depth
- Prevention
- Tension-free layered closure; avoid previous scars; smoking cessation and diabetic optimisation; prophylactic antibiotics
- Management
- Superficial: wound care, negative-pressure dressing, secondary healing; deep without hardware loosening: IV antibiotics and debridement, retain hardware if fusing; deep with loosening and non-union: hardware removal, debridement, staged revision
Non-union workup. Obtain a CT at six months if examination suggests failed union (persistent pain on subtalar stress or palpation). Add a metabolic and infection screen (vitamin D, calcium, HbA1c, ESR, CRP) and a bone scan if the CT is equivocal. Revision re-prepares the surfaces through the same approach with iliac crest autograft and improved fixation (add a second screw or change configuration) after correcting modifiable risk factors. Malposition revision. For a solidly fused but malpositioned heel, correct through an osteotomy of the fusion mass with a Gigli or oscillating saw, re-position to 0–5° valgus under fluoroscopy, supplement with bone graft, and revise fixation. Results are generally satisfactory when performed before secondary adjacent joint changes develop — no re-fusion is required because the joint is already united.
Viva & Exam Focus
SAFESAFE — four steps to solid union
VALGUSVALGUS — consequences of heel malposition
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old builder sustained a displaced intra-articular calcaneal fracture three years ago, treated non-operatively. He now has severe lateral hindfoot pain, cannot work, and is stiff. Weight-bearing CT confirms subtalar OA with preserved talonavicular and calcaneocuboid joints. What is your surgical plan, and what is the most critical technical decision?”
“What are the consequences of malposition at subtalar arthrodesis, and how do you prevent them? A patient returns 18 months post-operatively with lateral border foot pain and difficulty on uneven terrain; the subtalar fusion is solid on CT. What is your assessment?”
“You are asked to consent a 55-year-old woman with rheumatoid arthritis for isolated subtalar arthrodesis. Her subtalar OA is severe; the talonavicular and calcaneocuboid joints have mild OA changes on CT. What additional considerations apply, and how do they affect your consent and surgical planning?”
Indications
- Post-traumatic subtalar OA (calcaneal fracture sequelae) — most common; failed 3–6 months of conservative care
- Primary subtalar OA with preserved talonavicular and calcaneocuboid joints
- Talocalcaneal coalition with posterior facet involvement over 50% or secondary OA
- Stage IIB/C adult acquired flatfoot with fixed subtalar valgus and OA
- Inflammatory arthritis and Hawkins III–IV talar AVN isolated to the subtalar joint
Critical goal — heel alignment
- 0–5° valgus relative to the tibial axis with the foot plantigrade
- Varus: rigid supination, lateral border overload, fifth metatarsal stress fractures, peroneal pathology, knee varus
- Excessive valgus: medial midfoot strain, accelerated talonavicular arthrosis, knee valgus
- Confirm clinically plus fluoroscopically (lateral and Harris-Heath axial) before and after K-wire insertion
Surgical anatomy
- Posterior facet is the largest and the primary facet fused; oriented obliquely postero-lateral to antero-medial
- Anterior and middle facets lie in the sinus tarsi; the middle facet sits on the sustentaculum tali medially
- The interosseous talocalcaneal ligament fills the canalis tarsi and must be excised to expose all facets
- Sural nerve lies 1–2 cm posterior to the lateral malleolus — vessel-loop it early
- Peroneal tendons are retracted inferiorly; the medial neurovascular bundle is protected by staying lateral
Operative steps (SAFE)
- Surfaces — complete cartilage removal to bleeding cancellous bone
- Alignment — 0–5° valgus, clinical and fluoroscopic check before fixation
- Fixation — two cannulated large cancellous screws from posterior calcaneus to talar body
- Extras — sural nerve vessel-looped, peroneal tendons retracted, TN and CC joints not violated
Outcomes and evidence
- Union 84% overall in Easley 2000 (184 fusions); 96% in optimised non-smokers
- Smoking is the dominant risk factor: union 73% in smokers versus 92% in non-smokers; all non-unions had over 2 mm of avascular bone
- AOFAS improved from 24 to 70 (Easley 2000); 96% union and AOFAS 75 for calcaneal sequelae (Flemister 2000)
- CT is the gold standard for union — radiographs overestimate fusion (Coughlin 2006)
- Adjacent transverse-tarsal arthrosis is common long term and a key counselling point
Post-operative protocol
- 0–6 weeks: non-weight-bearing in cast or boot; wound check at 2 weeks
- 6 weeks: radiographic review; begin protected weight-bearing if satisfactory callus
- 8–12 weeks: progress to full weight-bearing in supportive footwear
- CT at 6 months if clinical concern for non-union
- Return to manual work at 4–6 months; annual review for adjacent joint surveillance
Background & Evidence
Epidemiology and indication profile. Isolated subtalar arthrodesis is performed most often for post-traumatic osteoarthritis after a displaced intra-articular calcaneal fracture, which destroys posterior facet cartilage in a substantial proportion of patients — Sanders Type III and IV fractures carry the highest risk of symptomatic subtalar OA. Primary subtalar OA is less common and typically affects older patients; talocalcaneal coalition, adult acquired flatfoot deformity (Stage II posterior tibial tendon dysfunction), inflammatory arthritis, and talar avascular necrosis make up the remainder. The operation is selected only when the talonavicular and calcaneocuboid joints are spared, preserving useful transverse tarsal and ankle motion and avoiding the greater stiffness of a triple arthrodesis. Hindfoot kinematics after fusion. The subtalar joint provides inversion and eversion (about 20–30° total range) with coupled internal and external rotation. Fusion abolishes this motion, but the midtarsal (Chopart) joints partially compensate. Mann (1998) quantified the motion lost after isolated fusion: transverse tarsal motion reduced by 40%, dorsiflexion by 30%, and plantarflexion by only 9% — useful motion is retained, which is why an isolated fusion is preferred over a triple whenever the adjacent joints allow. Post-traumatic calcaneal deformity classification (Zwipp). When subtalar fusion is combined with malunion correction, the Zwipp classification of post-traumatic calcaneal deformity guides the choice between in-situ fusion, distraction bone-block arthrodesis, and corrective osteotomy:
- Deformity
- Loss of height without significant joint depression
- Typical surgical response
- In-situ subtalar arthrodesis
- Deformity
- Loss of height with joint depression and hindfoot alignment change
- Typical surgical response
- Subtalar arthrodesis with correction
- Deformity
- Lateral wall exostosis and subtalar arthrosis
- Typical surgical response
- Lateral wall exostectomy plus in-situ fusion
- Deformity
- Severe loss of talocalcaneal height with anterior ankle impingement
- Typical surgical response
- Subtalar distraction bone-block arthrodesis
- Deformity
- Complex multi-planar deformity
- Typical surgical response
- Corrective calcaneal osteotomy plus arthrodesis
Union rates and the evidence base. Primary isolated fusion achieves union in roughly 84–95% of patients depending on selection. The landmark figures to quote: Easley (2000) reported an overall union rate of 84% (154 of 184 feet), rising to 96% only after excluding smokers, revisions, structural grafts, and fusions adjacent to a prior ankle fusion — examiners reward the real overall figure rather than the best-case subgroup. Smoking is the dominant modifiable risk factor: union fell from 92% in non-smokers to 73% in smokers, and every non-union occurred where more than 2 mm of avascular bone was present. For calcaneal-fracture sequelae specifically, Flemister (2000) reported 96% union across 86 fusions with a mean AOFAS of 75, independent of graft type — supporting local lateral-wall bone graft to avoid iliac-crest donor morbidity. Where a malunion has lost height and produced anterior ankle impingement, a distraction bone-block arthrodesis (Rammelt 2004) restores talocalcaneal height rather than a simple in-situ fusion. CT is the gold standard for assessing union — plain radiographs substantially overestimate the percentage fused (Coughlin 2006).
References
Isolated subtalar arthrodesis
- 184 consecutive isolated subtalar arthrodeses in adults; overall union rate 84% (154 of 184), not the 96% sometimes quoted
- Union fell from 92% in non-smokers to 73% in smokers; all 30 non-unions occurred in feet with greater than 2 mm of avascular bone
- AOFAS ankle-hindfoot score improved from 24 to 70; 96% union only after excluding smokers, revisions, structural grafts and adjacent ankle fusions
- Most frequent non-fusion complications were prominent hardware (20%) and lateral impingement (10%); symptomatic varus and valgus malalignment each 3%
Subtalar arthrodesis for complications of intra-articular calcaneal fractures
- 86 subtalar arthrodeses for calcaneal malunion, failed ORIF, or primary fusion of comminuted fractures; union in 83 of 86 (96%)
- Fusion rate was independent of graft type (iliac crest, local lateral-wall, or allograft); avoiding iliac crest harvest shortened hospital stay
- Mean AOFAS hindfoot score 75 at minimum 2-year follow-up; four varus malunions and four cases of osteomyelitis
- No correlation between postoperative talar declination angle and outcome; worker's compensation patients did worse
Isolated subtalar arthrodesis
- 48 isolated subtalar fusions; union achieved in all cases with one or two screws and 93% patient satisfaction
- Quantified loss of adjacent motion: transverse tarsal motion reduced 40%, dorsiflexion 30%, plantarflexion only 9%
- Radiographic progression of arthrosis in 36% of ankles and 41% of transverse tarsal joints at mean 59.5 months
- Six unsatisfactory results — three calcaneal stress fractures and three malpositioned fusions
Foot function after subtalar distraction bone-block arthrodesis: a prospective study
- 31 distraction bone-block arthrodeses for malunited calcaneal fractures with loss of height; no non-unions
- AOFAS hindfoot score improved from 23.5 to 73.2 at mean 33 months follow-up
- Talocalcaneal height corrected by 61.8% and talar declination by 38.5%; pedobarography normalised the roll-over pressure pattern
- Degree of heel-height correction correlated with normalised plantar pressure transfer
Comparison of radiographs and CT scans in the prospective evaluation of the fusion of hindfoot arthrodesis
- Prospective comparison of serial radiographs and CT for hindfoot fusion; agreement between the two methods was poor
- Radiographs overestimated posterior-facet fusion (86% at 6 months) compared with CT (64% at the same time point)
- Clinical results (AOFAS, VAS, SF-12) were independent of the radiographic percentage fused
- Concluded progress of fusion cannot be reliably judged on plain radiographs; CT is significantly more reliable
Clinical outcome after primary triple arthrodesis
- 111 patients (132 feet) undergoing primary triple arthrodesis; mean AOFAS 60.7
- 91% of patients stated they would repeat the procedure
- Significant radiographic progression of ankle arthritis over time
- Provides the comparator outcome data for triple versus isolated subtalar fusion
Subtalar arthrodesis with calcaneal osteotomy
- Describes the Type I to V classification of post-traumatic calcaneal deformity
- Guides the choice between in-situ fusion, distraction bone-block arthrodesis, and corrective osteotomy
- Combines arthrodesis with calcaneal osteotomy for complex multi-planar deformity
- Framework for planning simultaneous malunion correction at the time of subtalar fusion