Minimally invasive alternative for Sanders II-III calcaneal fractures — indirect reduction, fluoroscopy-guided fixation, low wound complications
- Sinus tarsi approach is a minimally invasive ALTERNATIVE to the lateral extensile approach: a small 3-4cm oblique incision over the sinus tarsi (anterolateral opening between talus and calcaneus), NO full-thickness flap elevation, relying on INDIRECT reduction techniques with fluoroscopy guidance.
- PRIMARY advantage — substantially lower wound complications: pooled relative risk of wound-related complications is 2.82 (95% CI 2.00-3.98) HIGHER for the lateral extensile approach versus sinus tarsi (Attenasio meta-analysis, 21 studies, 2086 patients); single-centre series report sinus tarsi wound complications of the order of 5-13% versus roughly 13-25% for extensile lateral. Ideal for high wound-risk patients (active smokers, diabetics, PAD) where soft tissue morbidity is the major concern.
- Patient selection is CRITICAL — the approach has LIMITED exposure: only the anterolateral posterior facet is visible through the sinus tarsi window, with NO access to the posteromedial facet or tuberosity fragments. It requires INDIRECT reduction (percutaneous manipulation, fluoroscopy) rather than direct visualization.
- Appropriate fracture patterns: Sanders II-III (2-3 part fractures) with MINIMAL posterior facet comminution (large fragments amenable to percutaneous reduction), PRIMARY fracture lines in the CORONAL plane (allows lateral manipulation), and an intact or minimally displaced sustentaculum tali (the medial reduction reference).
- INAPPROPRIATE patterns (use lateral extensile): Sanders IV (severe comminution, 4+ fragments — cannot reduce indirectly), central depression with small comminuted fragments (require direct visualization), significant tuberosity varus/valgus (no access through sinus tarsi), and medial wall comminution or sustentaculum fracture.
- Indirect reduction techniques required: percutaneous Essex-Lopresti maneuver (Schanz pin in the tuberosity to lever and restore height/Böhler angle), percutaneous bone tamps (elevate depressed posterior facet fragments through the sinus tarsi), and fluoroscopy guidance for reduction assessment (lateral, axial and Broden views).
When & Why
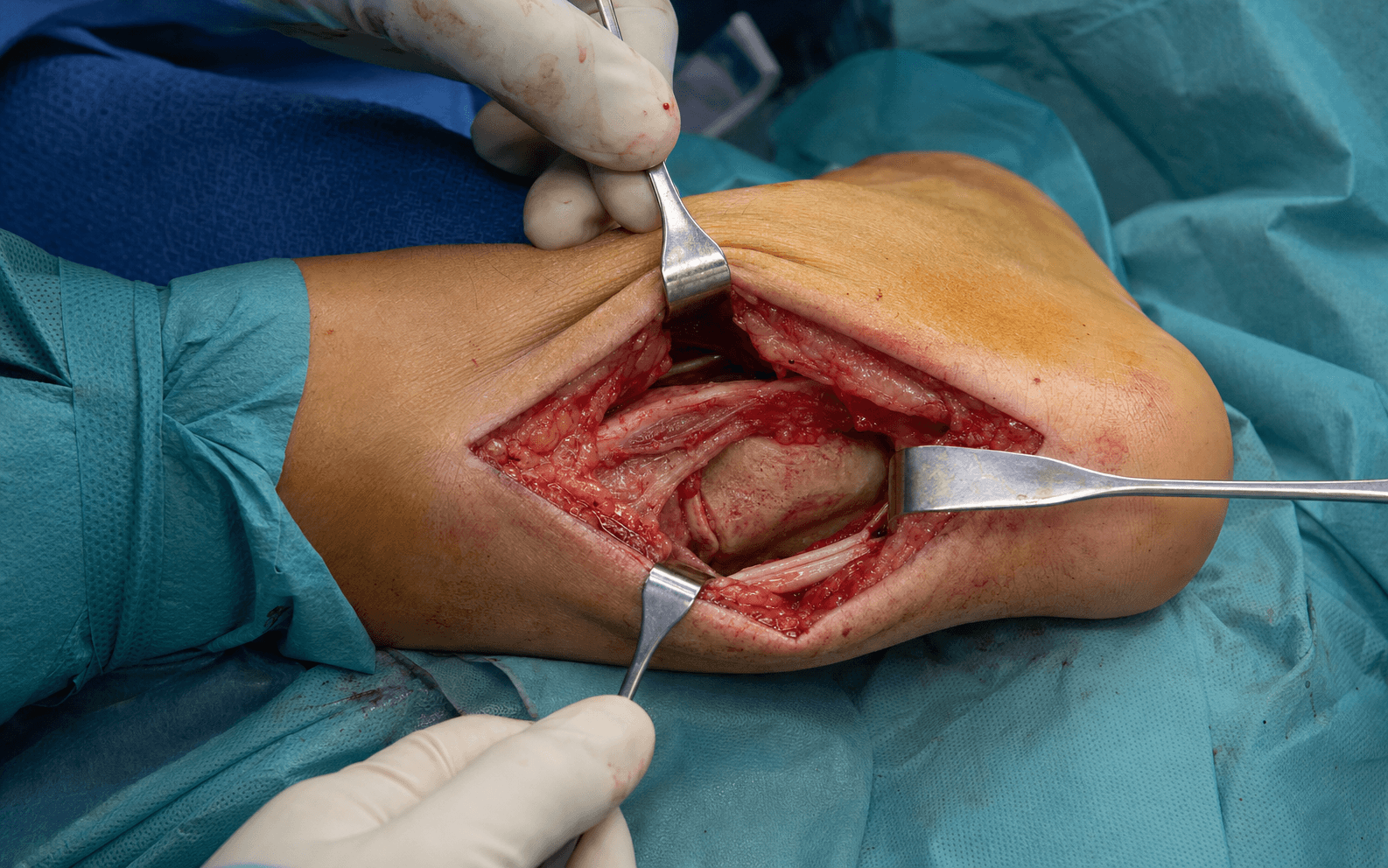
What it exposes. The sinus tarsi approach gives a small, direct window onto the anterolateral posterior facet of the calcaneus and the lateral wall, through the cone-shaped sinus tarsi (the anterolateral opening between the talus and calcaneus). It is a minimally invasive alternative to the lateral extensile (L-shaped) approach for displaced intra-articular calcaneal fractures, paired with percutaneous indirect reduction and fluoroscopy-guided fixation. Why it exists — wound safety. Wound breakdown (infection, dehiscence, full-thickness flap necrosis) is one of the largest barriers to successful extensile-lateral ORIF: even an anatomic reduction fails if the wound exposes the hardware. In a large extensile-lateral series the overall wound-complication rate was 17.8%, with smoking (OR 5.79), diabetes (OR 6.23) and higher Sanders grade (OR 5.44) the strongest independent predictors (Ding 2013). The sinus tarsi approach minimises the soft-tissue envelope — a 3-4 cm incision, no full-thickness flap, no extensive periosteal stripping, and a shorter operation — which is exactly why it is most valuable in high wound-risk patients. The trade-off — limited exposure. The approach does NOT give complete exposure. Only the anterolateral 30-40 percent of the posterior facet is seen directly; the posteromedial facet, the sustentaculum region and the tuberosity are assessed by fluoroscopy only. Reduction is therefore indirect — percutaneous Essex-Lopresti maneuver, plantar bone tamps and extensive fluoroscopy — so patient selection is critical. Ideal indications. Sanders II-III fractures with limited comminution (2-3 large fragments), primary fracture lines in the coronal plane (amenable to lateral manipulation), an intact sustentaculum tali (the medial reduction reference), and a displaced fracture (articular step-off greater than 2 mm or Böhler angle less than 20 degrees). It is especially attractive in high wound-risk patients — smokers, diabetics, the elderly with thin skin, the obese, and the previously scarred lateral hindfoot — and for one side of a bilateral injury. Contraindications (use lateral extensile). Sanders IV (severe comminution, 4+ fragments — cannot be reduced indirectly), central depression with small comminuted fragments, significant tuberosity varus/valgus (no access through the sinus tarsi), and medial-wall comminution or sustentaculum fracture (loss of the reduction reference). Relative contraindications are severe peripheral vascular disease (ABI less than 0.7) and fracture age greater than 3 weeks (early callus defeats indirect reduction).
The sinus tarsi approach succeeds only with appropriate patient selection. It provides limited exposure and relies on indirect, fluoroscopy-dependent reduction. Attempting it for a Sanders IV or severely comminuted pattern leads to persistent articular step-off greater than 2 mm and poor outcomes — subtalar arthritis, pain, and secondary fusion. If the pattern needs fragment-by-fragment reduction under direct vision, use the lateral extensile approach despite the wound risk; most comparative evidence (Yeo 2015, Lv 2020, Attenasio 2024) was restricted to Sanders II-III.
- Sinus tarsi
- 3-4 cm oblique, minimally invasive
- Lateral extensile
- 12-15 cm L-shaped, extensile
- Sinus tarsi
- No full-thickness flap (dissect through EDB)
- Lateral extensile
- Full-thickness flap (skin, subcutaneous, periosteum)
- Sinus tarsi
- Limited — anterolateral 30-40% direct, rest by fluoroscopy
- Lateral extensile
- Complete — entire facet under direct vision
- Sinus tarsi
- Indirect (Essex-Lopresti, plantar tamp, fluoroscopy)
- Lateral extensile
- Direct (each fragment under vision)
- Sinus tarsi
- Lower (~5-13%; pooled RR 2.82 favouring STA — Attenasio 2024; Davey 2020 9.4%)
- Lateral extensile
- Higher (17.8% in a large series; smoking OR 5.79, diabetes OR 6.23 — Ding 2013)
- Sinus tarsi
- Shorter (Attenasio 2024)
- Lateral extensile
- Longer
- Sinus tarsi
- Extensive — critical for reduction and hardware
- Lateral extensile
- Moderate — confirmatory
- Sinus tarsi
- Steep (indirect reduction, fluoroscopy expertise)
- Lateral extensile
- Moderate-high but familiar
- Sinus tarsi
- Sanders II-III, limited comminution, 2-3 large fragments
- Lateral extensile
- Sanders II-IV, all patterns, complex comminution
- Sinus tarsi
- Comparable (Yeo 2015 AOFAS 90)
- Lateral extensile
- Comparable (Yeo 2015 AOFAS 86; no difference — Lv 2020)
- Sinus tarsi
- Common long-term, driven by the initial injury (no difference — Lv 2020, Attenasio 2024)
- Lateral extensile
- Common long-term, driven by the initial injury
Position. Lateral decubitus, injured side up, ankle neutral — the same position as the extensile approach. Bean-bag or lateral positioners for stability; bolsters support the leg so the anterolateral foot is accessible. Tourniquet optional — many prefer it down given the shorter, minimally invasive procedure and the reduced ischaemia-time concern.
The Exposure
Work from skin to posterior facet through the sinus tarsi window, then reduce the fracture indirectly with the Essex-Lopresti maneuver and a plantar bone tamp, confirming everything by fluoroscopy before fixation.
Exposure sequence
- Lateral decubitus, injured side up, ankle neutral.
- Palpate the sinus tarsi — the depression just anterior to the lateral malleolus, lateral to the extensor digitorum brevis (EDB) belly.
- Mark a 3-4 cm oblique incision centered over the sinus tarsi, oriented about 45 degrees from anterior-superior to posterior-inferior (paralleling the peroneal tendons); do NOT extend anterior to the calcaneocuboid joint (EDB origin).
- Sharp dissection through skin and subcutaneous tissue.
- Identify the intermediate dorsal cutaneous nerve (a superficial peroneal branch) if it crosses the field — retract it, or accept division (limited dorsal foot numbness only).
- Identify the EDB muscle belly (reddish muscle overlying the sinus tarsi).
- Retract EDB anteriorly and inferiorly with a small Weitlaner or Gelpi self-retaining retractor — gentle traction, to avoid injuring its deep peroneal nerve branch.
- This exposes the sinus tarsi space posteriorly.
- Remove the sinus tarsi fat pad with a rongeur to expose the deeper structures.
- Partially release the talocalcaneal interosseous ligament (and cervical ligament if needed) to improve visibility of the posterior facet — do NOT completely destabilize the subtalar joint.
- The anterolateral aspect of the posterior facet is now visible; clear fracture haematoma and assess the depressed lateral fragment.
- Make a 5 mm stab incision posteriorly over the tuberosity and insert a 4.0 mm Schanz screw or Steinmann pin into the tuberosity fragment under lateral fluoroscopy.
- Apply traction posteriorly and inferiorly to disimpact the posterior facet and restore calcaneal height/Böhler angle (target 25-40 degrees on the lateral view).
- Make a 5 mm stab on the medial plantar heel (avoiding the weight-bearing area and the lateral plantar nerve).
- Advance a bone tamp or curved periosteal elevator superiorly through the calcaneus under fluoroscopy, engage the underside of the depressed posterior facet fragment, and lever it superiorly.
- AP view: confirm medial-lateral alignment with the sustentaculum.
- Lateral view: confirm Böhler angle restoration (25-40 degrees).
- Broden views (oblique 10-40 degrees cephalad): confirm posterior facet articular congruity (goal: step-off less than 2 mm) — the only way to assess the medial/posterior facet through this approach.
- Palpate the visible articular surface through the sinus tarsi with a probe — it should feel flush; trust tactile feedback over fluoroscopy alone.
- Hold the reduction with 2-3 percutaneous 2.0 mm K-wires into the reduced fragments.
- Definitive fixation: Option A — a small low-profile 3-4 hole calcaneal plate on the anterolateral wall through the sinus tarsi incision (extend slightly to 5-6 cm if needed) with 3.5 mm screws (most common); Option B — percutaneous 4.0-4.5 mm cannulated lag screws for simple 2-part patterns; Option C — combined plate plus percutaneous lag screws.
- Confirm final position on AP, lateral, Broden and axial views — ensure no intra-articular screw penetration and that heel width is normalized.
- Remove the temporary K-wires and allow the EDB to fall back over the sinus tarsi.
- Close the subcutaneous layer with 3-0 absorbable suture and the skin with interrupted or subcuticular sutures; the small incision heals under low tension.
- Apply a bulky compressive dressing and posterior splint; strict elevation, non-weight-bearing 6-8 weeks, advancing to full weight-bearing by 12 weeks, with ankle and subtalar ROM from week 2-3.
If reduction is inadequate (persistent step-off greater than 2 mm on Broden views) after 2-3 attempts, convert to the lateral extensile approach intraoperatively — extend the sinus tarsi incision into the L-shaped extensile incision. Residual articular step-off drives subtalar arthritis, so an anatomic reduction outweighs the incremental wound risk of converting.
The sinus tarsi gives only the anterolateral 30-40 percent of the posterior facet directly. The medial and posterior facet are judged on Broden views (10, 20, 30, 40 degrees cephalad) — accept the extra fluoroscopy time as the necessary trade-off for limited direct visualization, and do not proceed to fixation until fluoroscopy plus probe-palpation confirm a less than 2 mm step-off.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Intermediate dorsal cutaneous nerve (superficial peroneal branch)
- Protection
- Identify and retract if it crosses; division causes only limited dorsal numbness — far less troublesome than a sural nerve injury in the extensile approach
- Structure at risk
- Deep peroneal nerve lateral branch to EDB
- Protection
- Retract EDB gently with a self-retainer; avoid excessive traction (injury risk less than 1%)
- Structure at risk
- Peroneal tendons (brevis and longus) behind the lateral malleolus
- Protection
- Keep the incision anterior to the tendons; the peroneal sheath is not violated
- Structure at risk
- Arterial anastomosis (dorsalis pedis and peroneal branches)
- Protection
- Ligate or cauterize during dissection — collateral circulation is adequate
- Structure at risk
- Medial calcaneal branch of the tibial nerve / lateral plantar nerve
- Protection
- Place the plantar incision on the MEDIAL heel; stay subperiosteal during tamp advancement
Complications - Inadequate reduction (most common intraoperative issue). Persistent step-off greater than 2 mm or Böhler angle not restored to 25-40 degrees. Repeat the percutaneous maneuvers; if still inadequate after 2-3 attempts, convert to lateral extensile rather than accept malreduction.
- Intra-articular hardware (3-5%). Screw penetration into the subtalar joint — prevent with guide wires and Broden-view confirmation before final tightening; recognized post-op, return for removal/revision.
- Wound complications (3-5% — the primary advantage over extensile lateral at 10-25%). Superficial dehiscence 2-3%, superficial infection 1-2%, deep infection rare (less than 1%); manage as for the extensile approach (local care, oral/IV antibiotics, debridement if deep).
- Loss of reduction (5-8%). Usually early, from inadequate fixation, early weight-bearing, or severe osteoporosis; revise if under 3 weeks, otherwise observe and plan subtalar fusion if symptomatic arthritis develops.
- Subtalar arthritis (40-50% long-term — same as extensile lateral). Driven principally by the initial injury (articular impaction, Sanders grade, residual step-off) rather than the exposure; pooled comparisons show no significant radiographic difference between approaches (Lv 2020, Attenasio 2024). Anatomic restoration (step-off less than 2 mm) is the modifiable factor most associated with delaying secondary fusion.
- Hardware irritation (5-10%). Lower than the extensile approach; remove after union (12-18 months) if symptomatic. Extensile options. If the fracture is more complex than pre-op imaging suggested, convert to the lateral extensile approach by extending the sinus tarsi incision into the full L-shaped incision. For severe lateral wall collapse, add a small 2-3 cm lateral incision to push the wall fragments medially (total 5-7 cm, still lower wound risk than 12-15 cm extensile). A laminar spreader in the sinus tarsi (subtalar distraction) widens the window and improves visualization; bone graft may be packed through the sinus tarsi into a large metaphyseal void. Closure. Remove the temporary K-wires, replace the EDB over the sinus tarsi, close the subcutaneous layer loosely with absorbable suture and the skin with interrupted or subcuticular sutures, and apply a bulky dressing with a posterior splint.
Procedures Through This Approach
- ORIF of displaced intra-articular calcaneal fractures (Sanders II-III) — the principal operation done through this exposure.
- Subtalar arthrodesis — for post-traumatic arthritis or as salvage after calcaneal fracture.
- Triple arthrodesis — when subtalar, talonavicular and calcaneocuboid joints are all arthritic.
- Access to the calcaneocuboid joint and anterior process fractures, and as the working portal for subtalar arthroscopy.
Viva & Exam Focus
SINUSSINUS — patient selection for the sinus tarsi approach
PERCUTANEOUSPERCUTANEOUS — indirect reduction sequence
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old active smoker (1 pack/day) with a Sanders type III calcaneal fracture (3-part posterior facet, 2 fracture lines, 4 mm articular step-off, Böhler angle 18 degrees) presents 12 days post-injury. CT shows 3 large posterior facet fragments (no central comminution), fracture lines in the coronal plane, and an intact sustentaculum. He is highly motivated for surgery, understands the smoking risks, but is unable to quit. Soft tissues: wrinkle sign positive, no blisters. You are considering sinus tarsi vs lateral extensile vs nonoperative. What is your recommendation and rationale, and how do you counsel this patient on approach choice given his active smoking status?”
“A 35-year-old non-smoker, non-diabetic, healthy construction worker with a Sanders type II calcaneal fracture (2-part posterior facet, single fracture line, 5 mm step-off, Böhler angle 15 degrees) presents 11 days post-injury. CT shows a simple 2-part pattern, single coronal fracture line, minimal comminution, intact sustentaculum. Soft tissues excellent (wrinkle sign positive, no blisters). He has researched online and specifically requests the 'minimally invasive sinus tarsi approach' because of a 'smaller scar, less complications.' You are experienced with both approaches. Do you agree with his request, or do you recommend lateral extensile? What is your rationale and how do you counsel him?”
Critical anatomy
- Sinus tarsi: conical space on the anterolateral hindfoot between the talus (superior) and calcaneus (inferior), palpable depression anterior to the lateral malleolus
- Contents: talocalcaneal interosseous ligament, cervical ligament, fat pad, arterial anastomosis (dorsalis pedis and peroneal branches)
- Exposure: anterolateral 30-40% of the posterior facet visible directly; medial/posterior assessed by fluoroscopy only
- EDB overlies the sinus tarsi — retract anteriorly/inferiorly; innervated by the deep peroneal nerve lateral branch
- Intermediate dorsal cutaneous nerve (superficial peroneal) crosses the field — 5-10% injury risk, dorsal foot numbness
Primary indications
- Sanders II-III with LIMITED comminution (2-3 large fragments, simple coronal/sagittal fracture lines)
- HIGH wound-risk patients benefit most — smoking and diabetes are the strongest independent predictors of wound breakdown after extensile-lateral ORIF (OR 5.79 and 6.23, Ding 2013)
- Intact sustentaculum tali (medial reduction reference)
- EXCLUDE Sanders IV (severe comminution, central depression small fragments — need direct visualization)
- Evidence: pooled wound-complication RR 2.82 favouring sinus tarsi (Attenasio 2024) with no significant radiographic or functional difference (Yeo 2015, Lv 2020)
Surgical steps
- Position: lateral decubitus, injured side up, ankle neutral
- Incision: 3-4 cm oblique over the sinus tarsi, 45 degrees anterior-superior to posterior-inferior
- Exposure: retract EDB, remove the fat pad, partial ligament release
- Reduction (INDIRECT): Essex-Lopresti maneuver, then plantar bone tamp under fluoroscopy
- Fluoroscopy EXTENSIVE: AP, lateral, Broden (10-40 degrees cephalad — critical), axial
- Fixation: small plate via the sinus tarsi OR percutaneous cannulated lag screws
- Conversion: LOW threshold to extensile lateral if reduction is inadequate after 2-3 attempts
Complications
- Wound complications substantially lower than extensile lateral — the primary advantage (pooled RR 2.82 favouring STA, Attenasio 2024; Yeo 2015 ELA 13.3% significantly higher, p = 0.022)
- Inadequate reduction — the most common intraoperative issue; convert to extensile lateral if not achievable
- Steep learning curve — indirect, fluoroscopy-dependent; malreduction risk is higher early and falls with experience
- Subtalar arthritis common long-term — driven by initial injury severity, not the approach (Lv 2020, Attenasio 2024)
- Intermediate dorsal cutaneous nerve injury (5-10%) — dorsal foot numbness, not functionally limiting
Evidence
- Attenasio 2024 (Injury, meta-analysis, 21 studies, 2086 patients): wound-complication RR 2.82 (95% CI 2.00-3.98) higher with extensile lateral; longer operative time/stay; NO significant radiographic difference
- Lv 2020 (Arch Orthop Trauma Surg, 15 RCTs): no significant difference in Böhler/Gissane angle, calcaneal dimensions, or overall complications (RR 0.592, 95% CI 0.336-1.045)
- Yeo 2015 (BMC Musculoskelet Disord, 100 Sanders II-III): median AOFAS 90 (STA) vs 86 (ELA), no significant difference; ELA wound complications 13.3% significantly higher (p = 0.022)
- Ding 2013 (FAI, 490 extensile-lateral ORIF): wound complications 17.8%; strongest risk factors smoking (OR 5.79), diabetes (OR 6.23), Sanders grade (OR 5.44)
- Buckley 2002 (JBJS Am, RCT, 424 patients): NO overall operative vs nonoperative difference in 2-year SF-36 (68.7 vs 64.7, p = 0.13); subgroups (non-compensation, women, younger, anatomic reduction less than or equal to 2 mm) did better with surgery
Exam-day power phrases
- "Sinus tarsi offers a substantial wound-safety benefit (pooled wound-complication RR 2.82 favouring STA vs extensile lateral, 95% CI 2.00-3.98 — Attenasio 2024) with equivalent outcomes for APPROPRIATE patterns (Sanders II-III, 2-3 large fragments)"
- "PRIMARY indication: Sanders II-III with LIMITED comminution in HIGH wound-risk patients — smoking and diabetes are the strongest predictors of wound breakdown after extensile-lateral ORIF (OR 5.79 and 6.23 — Ding 2013)"
- "CRITICAL LIMITATION: Sanders IV is generally NOT suitable — it needs extensile exposure for fragment-by-fragment manipulation under direct vision"
- "Sinus tarsi gives LIMITED direct visualization (anterolateral 30-40% of the posterior facet) — it relies on INDIRECT reduction (Essex-Lopresti, plantar tamp, extensive fluoroscopy)"
- "LOW threshold to convert to extensile lateral if reduction is inadequate after 2-3 attempts — residual step-off greater than 2 mm drives subtalar arthritis"
- "Functional and radiographic outcomes are EQUIVALENT for appropriate fractures (Yeo 2015: AOFAS 90 STA vs 86 ELA; Lv 2020) — the sinus tarsi advantage is WOUND SAFETY, not better function"
References
Wound complications: extensile lateral vs sinus tarsi approach (updated meta-analysis)
- 21 comparative studies (4 RCTs, 17 cohort studies), 2086 patients — extensile lateral approach (ELA, n=1129) versus sinus tarsi approach (STA, n=957) for displaced intra-articular calcaneal fractures.
- Risk of postoperative wound-related complications was significantly HIGHER with ELA than STA: relative risk 2.82 (95% CI 2.00-3.98); reoperation risk also trended higher (RR 1.85, 95% CI 0.69-5.00).
- ELA was associated with longer time to surgery, longer operative times and longer hospital stay.
- NO statistically significant difference in final radiographic outcomes (Böhler angle, angle of Gissane, calcaneal height/length/width) between the two approaches.
- The excess wound-complication risk with ELA, while still present, was trending downward in more recent publications.
Sinus tarsi vs extensile lateral approach for Sanders II-III fractures — comparative cohort
- Retrospective cohort of 100 displaced intra-articular calcaneal fractures (40 sinus tarsi, 60 extensile lateral), Sanders type II and III only.
- Median final AOFAS hindfoot score 90 (sinus tarsi) vs 86 (extensile lateral) — no significant difference.
- Böhler angle, Gissane angle and calcaneal height/length/width were restored comparably in both groups, with no significant clinical or radiographic difference.
- Wound complication rate was 13.3% in the extensile lateral group, significantly higher than the sinus tarsi group (p = 0.022).
- Authors conclude the selective sinus tarsi approach is an effective, reliable option for Sanders II-III fractures with comparable outcomes and fewer wound complications.
Sinus tarsi vs extended lateral approach — systematic review and meta-analysis of RCTs
- 15 randomized controlled trials, 847 patients in the sinus tarsi group and 959 in the extended lateral group.
- No significant difference in change of Böhler angle, Gissane angle, or calcaneal height, width or length between approaches.
- No significant difference in overall complication incidence (risk ratio 0.592, 95% CI 0.336-1.045).
- Authors conclude there is no difference in clinical efficacy between the two approaches for displaced intra-articular calcaneal fractures, while noting the need for larger long-term RCTs.
Short-term outcomes of sinus tarsi ORIF in an unselected cohort — effect of smoking
- 58 intra-articular calcaneal fractures (53 patients) treated via the sinus tarsi approach in a non-exclusively selected cohort; mean follow-up 35.4 months.
- Wound complications occurred in 5 patients (9.4%): 2 superficial (3.7%) and 3 deep (5.6%); 4 of the 5 were smokers.
- Smokers were significantly more likely to develop wound infection than non-smokers (p = 0.04), so wound risk is reduced but not eliminated by the limited approach.
- The authors recommend operative fixation to improve long-term function but emphasise that smoking shifts the risk-benefit balance and warrants counselling/cessation.
Durable outcomes of sinus tarsi ORIF at over 5 years follow-up
- 34 fractures (31 patients) with minimum 5-year follow-up after sinus tarsi ORIF for intra-articular calcaneal fractures (mean follow-up 81.9 months).
- Maryland Foot Score improved significantly from short-term (mean 77.6) to medium-term (mean 86) follow-up (p = 0.008), indicating maintained or improving function over time.
- No significant difference between immediate postoperative and long-term Böhler angle (p = 0.97) — radiographic reduction was durable.
- Wound complications occurred in 12.9% (3 infections, 2 delayed healing); reoperation in 32% (mostly elective removal of metal in 29%; subtalar fusion in 6%).
- Authors conclude clinical and radiographic outcomes after sinus tarsi ORIF are stable beyond 5 years, supporting its continued use.