Peroneal-protecting exposure of the fibular shaft — identify the superficial peroneal nerve in the distal third, then stay subperiosteal to keep the peroneal vessels safe.
- The internervous plane lies between the peroneal compartment (superficial peroneal nerve) and the posterior compartment (tibial nerve) — retract the peronei anteriorly and work on bone.
- The superficial peroneal nerve pierces the crural fascia in the distal third, about 8 to 12 cm proximal to the lateral malleolus, and lies superficial in the distal 5 cm — identify and protect it before any fascial incision.
- Strict subperiosteal dissection on the fibular shaft keeps the peroneal artery and veins safely posterior in the deep compartment.
- The approach is extensile proximally toward the fibular head (common peroneal nerve caution) and distally to the lateral malleolus for ankle fractures.
- For strut graft harvest, take the middle third and leave at least 6 to 8 cm of distal fibula to preserve ankle stability.
When & Why
What it exposes. The lateral approach gives direct, extensile access to the entire fibular shaft — from the fibular neck proximally to the lateral malleolus distally — and is the standard exposure for fibular ORIF, syndesmotic stabilisation, and middle-third strut graft harvest. It works a true internervous plane and, executed subperiosteally, keeps the peroneal vessels posterior and protected. Primary indications.
- Fibular shaft fractures requiring ORIF (isolated or combined with tibial injury).
- Weber B and C ankle fractures needing fibular plating and syndesmotic stabilisation.
- Fibular bone graft or strut harvest for reconstruction (middle third preferred).
- Corrective fibular osteotomy for malunion, ankle deformity, or limb-length issues.
- Peroneal nerve exploration or decompression at the fibular neck.
- Proximal fibular pathology (tumours, nonunions) requiring exposure. Why this approach is chosen. The lateral route provides direct access to the whole fibular shaft while protecting the superficial peroneal nerve when properly executed. It allows plate placement on the lateral or posterolateral surface, is extensile in both directions, and subperiosteal technique keeps the peroneal vessels posterior and safe. Contraindications. Active infection over the proposed incision; severe soft-tissue compromise requiring staged or alternative surgery; isolated medial pathology better addressed through a medial approach; and unplanned common peroneal nerve exploration proximally without adequate preparation. Alternative approaches. A posterolateral approach to the tibia-fibula for combined posterior exposure; an anterolateral approach when anterior-compartment access is also needed; and a medial tibial approach when only tibial shaft work is required. Position and landmarks. Supine with a bump under the ipsilateral hip to internally rotate the leg, or lateral decubitus with the affected side up when combined posterior access is anticipated. The knee is slightly flexed to relax gastrocnemius-soleus, the foot is free-draped for intra-operative ankle motion, and a high thigh tourniquet is used when a bloodless field is needed. Palpable landmarks are the fibular head, the subcutaneous fibular shaft, and the lateral malleolus; the superficial peroneal nerve is often visible subcutaneously in thin patients in the distal third, and the sural nerve runs posterior to the lateral malleolus with the short saphenous vein. Plan a longitudinal incision along the posterior border of the fibula, 4 to 8 cm for mid-shaft work and longer for extensile needs, centred over the pathology.
Limit tourniquet time to less than 120 minutes where possible to reduce nerve ischaemia, and document superficial peroneal nerve sensory and motor function both before and after surgery. Release the tourniquet before closure to confirm haemostasis.
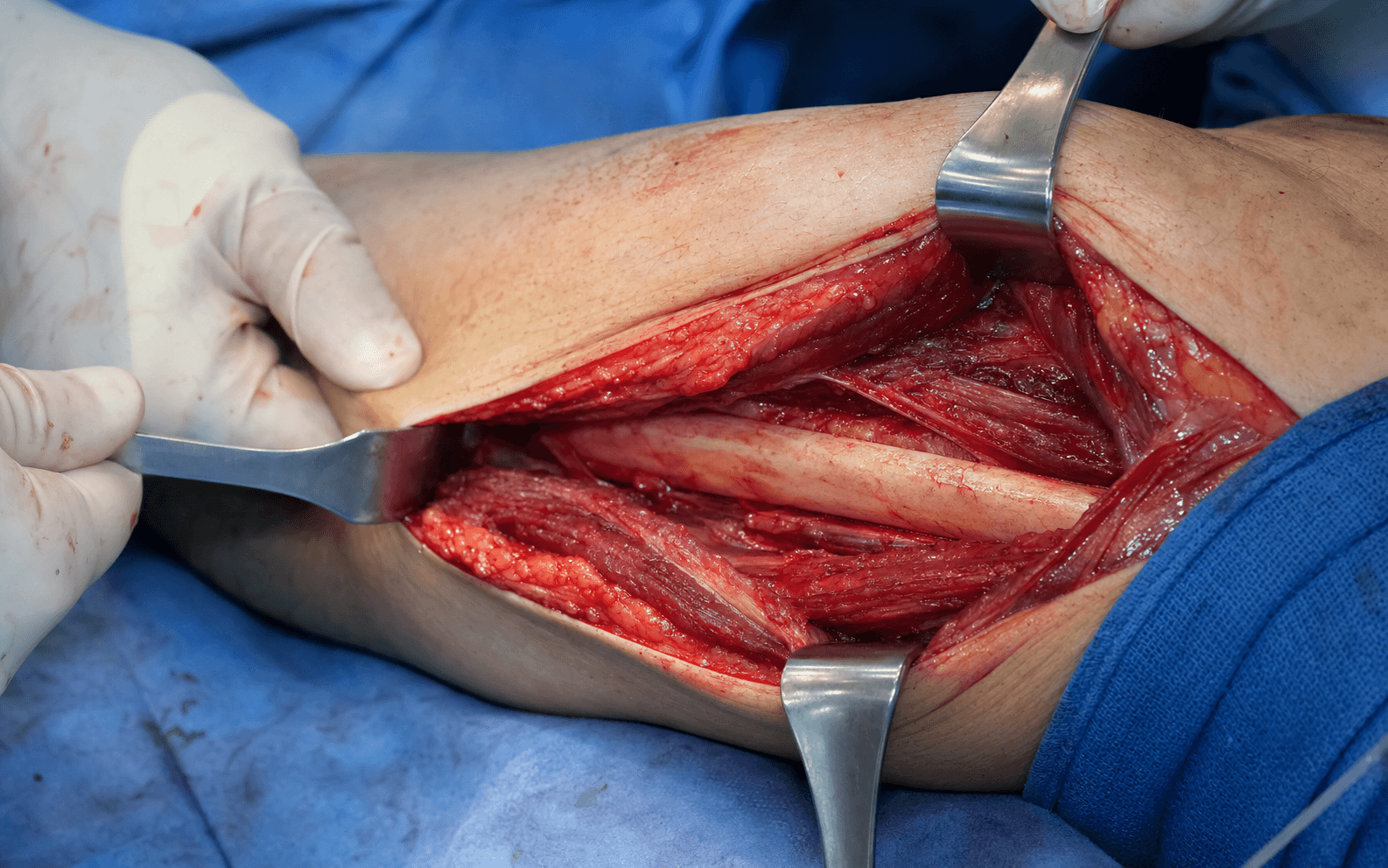
The Exposure
Work down through the layers along the posterior fibular border: find and protect the superficial peroneal nerve in the distal third, open the lateral-compartment fascia, develop the internervous plane, and dissect strictly subperiosteally to keep the peroneal vessels posterior.
Anatomy that governs the exposure. The fibular shaft is triangular in cross-section with anterior, posterior, and lateral (subcutaneous) borders; the middle third is the usual strut-graft donor site, and the distal fibula forms the lateral malleolus of the ankle mortise. The deep dissection passes between two compartments supplied by different nerves, which is the basis of the internervous plane.
- Muscles
- Peroneus longus and brevis
- Nerve supply
- Superficial peroneal nerve
- Muscles
- Tibialis posterior, flexor digitorum longus, flexor hallucis longus
- Nerve supply
- Tibial nerve
Internervous plane. The deep plane runs between the peroneal muscles (superficial peroneal nerve) anteriorly-laterally and the posterior-compartment muscles (tibial nerve) posteriorly. The peronei are retracted anteriorly as a unit and the posterior compartment falls back, exposing the fibular shaft without crossing nerve territories. Superficially there is no classical internervous plane — the incision crosses subcutaneous tissue and the lateral-compartment fascia, so the superficial peroneal nerve must be identified where it pierces the fascia before any deep retraction.
Exposure sequence
- A longitudinal incision along the posterior border of the fibula, centred over the area of interest: 6 to 8 cm for mid-shaft exposure, extended distally to the lateral malleolus for ankle fractures, or toward the fibular head for proximal pathology.
- This line keeps the peroneal muscles anterior and the peroneal vessels posterior.
- In the distal third, before any fascial incision, identify the superficial peroneal nerve as it emerges through the crural fascia about 8 to 12 cm proximal to the lateral malleolus.
- Trace it proximally and distally, protect it with a vessel loop, and avoid self-retaining retractors that compress it.
- Incise the fascia of the lateral compartment along the posterior fibular border — peroneus brevis lies directly on the fibula posteriorly.
- Develop the plane between the peroneal muscles anteriorly and the posterior-compartment muscles posteriorly.
- Retract the peroneal muscles (longus and brevis) anteriorly as a unit to expose the fibular shaft.
- This is the internervous interval between the peroneal compartment (superficial peroneal nerve) and the posterior compartment (tibial nerve).
- Elevate strictly subperiosteally with a periosteal elevator, staying on the fibula at all times.
- This keeps the peroneal artery and veins posterior and protected within the deep posterior compartment — never stray off bone posteriorly.
- Continue subperiosteal dissection proximally and distally as needed; the whole shaft from head to malleolus can be exposed.
- For graft harvest, expose the middle third with the peroneal vessels protected posteriorly; for plating, apply the plate to the lateral or posterolateral surface.
The superficial peroneal nerve pierces the crural fascia at a variable but predictable point in the distal third of the leg, typically 8 to 12 cm proximal to the tip of the lateral malleolus, and lies superficial to the fascia in the distal 5 cm where it is most vulnerable. Always identify and protect it before any fascial incision or deep retraction.
The single most important step in the distal third is identifying the superficial peroneal nerve before incising the fascia. Injury causes sensory loss on the dorsum of the foot and a painful neuroma. Once found, protect it with a vessel loop throughout the case and avoid fascial-edge compression from retractors.
Dangers & Extensions
Structures at risk, by layer.
- Structure at risk
- Sural nerve branches (posterior to the lateral malleolus)
- Protection
- Identify and retract posteriorly if encountered
- Structure at risk
- Superficial peroneal nerve at its emergence point (distal third)
- Protection
- Identify before fascial incision; loop and protect with a vessel loop
- Structure at risk
- Peroneus longus and brevis
- Protection
- Retract anteriorly as a unit — muscle retraction only
- Structure at risk
- Peroneal artery and veins (immediately deep to the fibula)
- Protection
- Stay strictly subperiosteal on bone — never stray posteriorly
- Structure at risk
- Common peroneal nerve around the fibular neck
- Protection
- Identify early around the neck if extending proximally
If the SPN is injured. A transected nerve should undergo primary microsurgical repair where possible; a neurapraxia is observed, with an AFO if foot drop is present and EMG at three weeks; permanent sensory loss is managed with neuroma care, desensitisation, and revision surgery if symptomatic. Extensile options. Extend proximally toward the fibular head for peroneal nerve exploration or proximal pathology — identify the common peroneal nerve early as it winds around the neck. Extend distally to the tip of the lateral malleolus for Weber B/C ankle fractures and syndesmotic stabilisation, protecting the peroneal tendons and sural nerve. For combined tibial and fibular pathology, the lateral fibular approach can be combined with anterolateral or posterolateral tibial approaches through separate or connected incisions. Closure. Copious irrigation and meticulous haemostasis, particularly around the peroneal vessels. Release the tourniquet before closure to confirm haemostasis. Place a drain only if significant bleeding or dead space is expected, exiting it away from the superficial peroneal nerve course. Close the fascial layer loosely with absorbable suture to avoid compartment syndrome, approximate subcutaneous tissue, and close skin with staples or interrupted sutures. Confirm fibular reduction, plate position, and the ankle mortise on AP, lateral, and mortise views, and document SPN function immediately after surgery.
- Incidence
- 5 to 10 percent (usually transient)
- Prevention and management
- Identify and protect the nerve; observe and desensitise
- Incidence
- Less than 2 percent
- Prevention and management
- Avoid fascial-edge compression; revision surgery if symptomatic
- Incidence
- 1 to 3 percent
- Prevention and management
- Soft-tissue care and prophylactic antibiotics; irrigation and debridement if needed
- Incidence
- 2 to 5 percent
- Prevention and management
- Stable fixation and bone graft if needed; revision ORIF or bone stimulation
- Incidence
- Rare with correct technique
- Prevention and management
- Preserve the distal 6 to 8 cm of fibula; reconstruct if symptomatic
Transient superficial peroneal sensory disturbance occurs in 5 to 10 percent of lateral fibular approaches and usually resolves within six months; permanent sensory loss or neuroma pain occurs in less than 2 percent. Meticulous identification of the nerve at its fascial emergence point is the key preventive measure.
Procedures Through This Approach
- Fibular plating (ankle and shaft fractures) — apply a 3.5 mm or 2.7 mm plate to the lateral or posterolateral surface; for Weber B and C fractures achieve anatomic reduction of the lateral malleolus and assess syndesmotic stability with the hook test or external rotation stress, using lag screws with neutralisation or buttress plating as indicated.
- Fibular strut graft harvest — expose the middle third, cut the required length with an oscillating saw under direct vision while protecting the peroneal vessels posteriorly, and preserve at least 6 to 8 cm of distal fibula for ankle stability; fill or plate the defect if a large graft is taken.
- Corrective fibular osteotomy — mark the planned level, perform the osteotomy with a saw or osteotomes under direct vision, correct rotation, length, or angulation, stabilise with plate and screws, and assess the ankle mortise fluoroscopically.
- Peroneal nerve exploration at the fibular neck — via the proximal extension, identifying and protecting the common peroneal nerve as it winds around the neck.
- Proximal fibular pathology (tumours, nonunions) through the extended proximal exposure.
Viva & Exam Focus
FIBULA SAFELateral fibula approach — step sequence
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old sustains a direct blow to the lateral leg with an isolated fibular shaft fracture at the junction of the middle and distal thirds. How would you approach fixation?”
“You are planning to harvest a 10 cm fibular strut graft for mandibular reconstruction. Describe your approach and the key technical points to minimise morbidity.”
“A 42-year-old with a Weber C ankle fracture requires fibular plating, and the fracture extends into the distal third. How do you protect the SPN during the approach?”
Position
- Supine with a bump under the ipsilateral hip, or lateral decubitus affected side up
- High thigh tourniquet if a bloodless field is needed
- Prep the entire leg to mid-thigh
- Document SPN function pre-operatively
SPN protection
- Pierces the fascia 8 to 12 cm proximal to the lateral malleolus
- Identify it before incising the fascia in the distal third
- Protect with a vessel loop and trace proximally and distally
- Avoid fascial-edge compression and self-retaining retractors on the nerve
Internervous plane
- Peroneal compartment (superficial peroneal nerve) versus posterior compartment (tibial nerve)
- Peroneal muscles retracted anteriorly
- Stay strictly subperiosteal on the fibular bone
- Peroneal vessels kept posterior and protected
Dangers by layer
- Subcutaneous: sural nerve branches posteriorly
- Fascia: SPN at its emergence point (distal third)
- Peroneal compartment: muscle retraction only
- Deep: peroneal vessels protected by the subperiosteal plane
- Proximal: common peroneal nerve around the fibular neck
Indications
- Fibular plating for ankle and leg fractures
- Strut graft harvest (middle third, preserve distal 6 to 8 cm)
- Corrective fibular osteotomy
- Peroneal nerve exploration at the fibular neck
- Proximal fibular pathology
Extensile options
- Proximal: toward the fibular head with common peroneal nerve protection
- Distal: to the lateral malleolus for ankle fractures
- Combined: with anterolateral or posterolateral tibial approaches
- Always identify and protect nerves at each extension
References
The lateral approach to the fibula is used worldwide for fibular fixation, graft harvest, and osteotomy, and the principles are consistent across advanced orthopaedic practice and equivalent examination systems: SPN identification in the distal third and subperiosteal technique to protect the peroneal vessels are universal requirements.
- Position on the fibular approach
- Lateral approach standard for fibular shaft and malleolar fixation; SPN protection mandatory; subperiosteal technique emphasised for vessel safety
- Position on the fibular approach
- Early soft-tissue assessment; document nerve function pre- and post-operatively; staged management for high-energy injuries with swelling
- Position on the fibular approach
- Anatomic fibular reduction restores the ankle mortise; CT for complex patterns; SPN morbidity discussed in consent
Registry and population evidence. Fibular fractures occur in about 10 to 15 percent of all lower-limb fractures, and ankle fractures requiring fibular plating are the most common indication for this approach. Donor-site morbidity after fibular graft harvest is primarily transient SPN sensory disturbance in 5 to 10 percent. In high-resource settings, dedicated small-fragment and mini-fragment locking systems are standard; in resource-limited settings, one-third tubular and 3.5 mm reconstruction plates give equivalent outcomes when technique is sound, with external fixation used more often for temporisation. Consent (globally applicable). Discuss superficial peroneal nerve sensory loss (5 to 10 percent transient, less than 2 percent permanent), peroneal vessel injury (rare with correct technique), infection (1 to 3 percent), nonunion (2 to 5 percent), and ankle instability after graft harvest if the distal fibula is not preserved.
Surgical anatomy of the superficial peroneal nerve in the ankle and foot
- Anatomic study defining the emergence point of the superficial peroneal nerve through the crural fascia
- The nerve pierces the fascia at an average of 8 to 12 cm proximal to the lateral malleolus in the distal third
- In the distal 5 cm the nerve lies superficial to the fascia and is vulnerable to surgical injury
- Recommended identification and protection before fascial incision in lateral approaches
Free vascularised fibular grafting for reconstruction after tumour resection
- Free vascularised fibular grafts provide reliable structural reconstruction after tumour resection
- High union rates achieved with meticulous vascular anastomosis and subperiosteal harvest technique
- Peroneal vessel protection is critical during harvest to maintain graft viability
- Donor-site morbidity is low when the middle third is used and ankle stability is preserved
Free fibula donor-site morbidity: the Mayo experience with 100 consecutive harvests
- Long-term follow-up shows a low rate of ankle instability when the distal fibula is preserved
- Transient SPN sensory loss occurs in a minority of patients
- Donor-site pain and weakness resolve in the majority by one year
- Pre-operative counselling regarding nerve sensory changes is essential
Proportional localisation of the peroneal nerve along the fibula
- Detailed anatomic mapping of the peroneal nerve course along the fibula for surgical planning
- Proportional localisation aids identification during the lateral approach to avoid injury
- Critical for safe exposure in distal and mid fibular shaft procedures
- Confirms the highest-risk zone in the distal third, consistent with prior anatomic studies