Posterior viewing portal, anterior rotator-interval portal and an anteroinferior (5 o'clock) working portal to reattach the avulsed anteroinferior labrum
- Recurrent anterior shoulder instability with a Bankart lesion (anteroinferior labral detachment from 2 to 6 o'clock) confirmed on MRI — minimum 2 dislocations, or 1 dislocation with persistent instability symptoms.
- First-time traumatic dislocation in a high-risk patient: young athlete under 25 years, contact or overhead sport, ISIS score less than 6, an on-track Hill-Sachs lesion, and glenoid bone loss less than 20 percent.
- Critical decision threshold: glenoid bone loss greater than 20 to 25 percent, inverted-pear morphology, or an off-track Hill-Sachs lesion is an absolute contraindication to isolated repair and requires a bone-augmentation procedure (Latarjet or distal tibial allograft).
- Technical essential: anchors MUST sit on the glenoid articular face, 2 to 3 mm from the cartilage edge (not on the glenoid neck) to restore the anatomic labral bumper — 'on the dance floor, not in the hallway'.
When & Why
Indication. Symptomatic recurrent traumatic anterior glenohumeral instability with a Bankart lesion (anteroinferior labral detachment, typically 2 to 6 o'clock) confirmed on MRI arthrogram, following a fair trial of non-operative management (physiotherapy for at least 3 to 6 months for a first-time dislocation). Operate when there have been at least 2 dislocations, or 1 dislocation with persistent subluxation or apprehension, provided there is no critical bone loss. Select the patient on bone loss and engagement, not on the labrum alone. The single most important pre-operative decision is whether the soft tissue can be expected to hold. Three findings rule out an isolated arthroscopic Bankart and demand a bone-block procedure (Latarjet, distal tibial allograft): glenoid bone loss greater than 20 to 25 percent, an inverted-pear glenoid, or an off-track (engaging) Hill-Sachs lesion. ### ISIS score — the primary risk stratification The Instability Severity Index Score (Balg and Boileau) predicts failure of arthroscopic Bankart from six pre-operative factors.
- Points
- 2
- Rationale
- Higher recurrence (60 to 90 percent) in adolescents — activity level and tissue quality
- Points
- 2
- Rationale
- Increased shoulder loading and re-injury risk
- Points
- 2
- Rationale
- Football, rugby, wrestling, volleyball — highest re-dislocation rates
- Points
- 1
- Rationale
- Generalised ligamentous laxity predicts capsular failure
- Points
- 2
- Rationale
- A lesion large enough to see on plain film means substantial bone loss
- Points
- 2
- Rationale
- Any visible glenoid loss on AP indicates greater than 10 to 15 percent loss — quantify with CT
Interpretation (total 0 to 10): - 0 to 2 points — less than 10 percent recurrence; arthroscopic Bankart is appropriate.
- 3 to 5 points — about 30 percent recurrence; reasonable with counselling.
- 6 points or more — about 70 percent recurrence; favour a primary Latarjet, particularly in young contact athletes. ### Glenoid bone loss — measure it, then apply the threshold Measurement techniques: - CT en-face view with a best-fit circle (gold standard): overlay a circle on the intact superior glenoid; percent loss equals defect width divided by the circle diameter, times 100.
- Arthroscopic bare-spot method: the native glenoid width equals twice the distance from the bare spot (anatomic centre) to the intact posterior rim; compare with the anterior (damaged) side.
- Pico method (arthroscopic): percent loss equals defect width divided by (defect plus intact anterior rim), times 100.
- Recurrence after Bankart
- About 3%
- Recommendation
- Isolated Bankart is safe (low recurrence)
- Recurrence after Bankart
- About 15%
- Recommendation
- Individualise on ISIS score and activity; Bankart possible with counselling
- Recurrence after Bankart
- 50 to 70%
- Recommendation
- Absolute indication for bone augmentation (Latarjet / distal tibial allograft)
- Recurrence after Bankart
- Very high
- Recommendation
- Larger reconstruction (iliac-crest autograft / structural allograft)
- Hill-Sachs track equals the distance from the medial rotator-cuff footprint to the medial margin of the Hill-Sachs defect.
- On-track: the Hill-Sachs track is less than the glenoid track — the lesion stays medial to the glenoid throughout functional range, and isolated Bankart is safe.
- Off-track: the Hill-Sachs track is greater than the glenoid track — the lesion engages the anterior rim in abduction and external rotation and requires remplissage (if glenoid loss is under 20 percent) or Latarjet. Confirm dynamically at arthroscopy: rotate the arm into abduction-external rotation and watch whether the defect rides up onto the glenoid rim. ### Indications, relative indications and contraindications
Recurrent traumatic anterior instability (2 or more dislocations, or 1 dislocation plus multiple subluxations) with a Bankart lesion on MRI; glenoid bone loss less than 20 percent and an on-track Hill-Sachs; failed conservative management; first-time dislocation in a high-risk young athlete unwilling to accept a 60 to 80 percent recurrence with non-operative care.
Persistent apprehension despite normal imaging; an ALPSA lesion with capsular redundancy; a combined Bankart and SLAP lesion (address both).
Glenoid bone loss greater than 20 to 25 percent; an off-track Hill-Sachs lesion; absent or severely attenuated labral tissue; active infection; significant glenohumeral arthritis; voluntary or psychiatric instability.
Position: beach chair or lateral decubitus? Both give equivalent outcomes in randomised studies — the choice is surgeon preference and the access needed.
- Beach chair
- Familiar, anatomic
- Lateral decubitus
- Unfamiliar (body rotated 90 degrees)
- Beach chair
- Moderate
- Lateral decubitus
- Superior — gravity aids the view
- Beach chair
- Easy
- Lateral decubitus
- Difficult
- Beach chair
- Lower
- Lateral decubitus
- Higher — keep traction under 15 lb
- Beach chair
- Less (gravity pulls head back)
- Lateral decubitus
- Better
- Beach chair
- Risk of hypotension — keep MAP over 70 mmHg
- Lateral decubitus
- Less risk
Consent. Counsel specifically for recurrence (higher in contact athletes and the ISIS-high group), loss of 10 to 15 degrees of external rotation as a normal consequence of capsular tightening, stiffness or frozen shoulder, axillary/musculocutaneous nerve injury, infection (including late Cutibacterium acnes), and the possibility of conversion to Latarjet if critical bone loss is found intra-operatively (about 10 to 15 percent of planned arthroscopic cases).
The Operation
The goal is to restore the anteroinferior labral bumper and tension the inferior glenohumeral ligament (IGHL) by anatomically reattaching the avulsed capsulolabral complex to the glenoid face with suture anchors, through three portals — a posterior viewing portal, an anterior rotator-interval portal, and an anteroinferior (5 o'clock) working portal. The exposure is the portal placement itself: it is laid out as the first steps below, because every later move depends on it.
Operative sequence
- Beach chair at 45 to 60 degrees head-up (torso tilted en bloc), head secured in a horseshoe or Mayfield rest, or lateral decubitus with an axillary roll and 10 to 15 lb longitudinal plus 5 to 10 lb lateral traction through the forearm (abduction 30 to 45 degrees, forward flexion 20 to 30 degrees).
- Arm in a pneumatic or mechanical holder (Spider, McConnell, TRIMANO) giving 45 to 90 degrees abduction, 0 to 90 degrees forward flexion and full rotation.
- Mark the bony landmarks: anterolateral and posterolateral acromion corners, clavicle, AC joint, and the coracoid tip.
- Test before draping that you can reach the inferior glenoid (90 degrees abduction, 60 degrees external rotation) without the humeral head blocking the working portal.
- Keep C-arm access available in case a bony Bankart is discovered and needs screw fixation.
- Palpate the posterolateral acromion corner; mark the soft spot 2 cm inferior and 1 cm medial to it (the infraspinatus–teres-minor interval).
- Infiltrate local anaesthetic (10 mL 0.5 percent bupivacaine with 1:200,000 epinephrine); inflate the joint with 50 to 60 mL saline through an 18-gauge spinal needle aimed at the coracoid (easy flow confirms intra-articular position).
- 1 to 1.5 cm vertical skin incision; enter with a blunt obturator aimed anteromedially toward the coracoid tip; insert the 30-degree, 4 mm arthroscope. This portal views throughout.
- Rotator-interval portal: from the posterior view, identify the triangle between subscapularis (inferior), supraspinatus (superior) and the biceps tendon (medial). Use an outside-in 18-gauge spinal needle aimed at the centre of the interval just anterior to biceps; external entry is about at the anterior acromion edge, 2 to 3 cm inferior to the anterolateral corner. Make an 8 mm incision, dilate, insert an 8 mm cannula.
- Anteroinferior 5 o'clock portal — the critical working portal, and the one most commonly malpositioned by trainees. Under direct vision, pass a spinal needle just anterior to the subscapularis border at the level of the inferior glenoid (5:30 right shoulder, 6:30 left). The trajectory MUST reach the glenoid face at 5:30 and allow perpendicular drilling — confirm by touching the needle to the rim before incising. Skin entry is typically 2 to 3 cm inferior and 1 cm lateral to the interval portal, but anatomy determines position, not landmarks.
- This is the primary working portal for the shaver, burr, anchor insertion and suture management.
- Pump at 40 to 60 mmHg. Systematic examination from the posterior view: biceps anchor (SLAP?), superior labrum 10 to 2 o'clock, rotator-cuff articular surface, anterior labrum 2 to 6 o'clock (extent of the Bankart), inferior and posterior labrum, glenoid cartilage, humeral head (Hill-Sachs size and depth).
- Glenoid bone loss: use the bare-spot method — measure posterior rim distance (native radius) and anterior rim distance; percent loss equals (posterior minus anterior) divided by posterior, times 100. If loss is greater than 20 to 25 percent, or the glenoid is inverted-pear, STOP the soft-tissue repair and plan a Latarjet.
- Hill-Sachs: measure width and depth; perform the dynamic engagement test in abduction-external rotation. Off-track (engaging) lesions need remplissage or Latarjet.
- Check the drive-through sign (capsular laxity) and probe the inferior capsule to exclude a HAGL lesion (humeral avulsion of the IGHL).
- Insert a curved periosteal elevator (Fukuda/liberator) through the anteroinferior portal. Mobilise the capsulolabral complex as a single unit off the glenoid neck, starting at 3 o'clock and working inferiorly to 6 o'clock, staying on bone.
- In chronic cases the labrum is scarred medially (ALPSA pattern, 50 to 60 percent of recurrent instability) — it must be freed back to an anatomic position.
- Mobilisation is complete when you can see subscapularis muscle fibres through the thinned capsule, when the labrum reaches the rim without tension, and when a pocket has been created between the complex and the neck.
- STOP at 6 o'clock inferiorly — the axillary nerve lies along the inferior capsule.
- Through the anteroinferior portal, use a 4.0 mm round burr or rasp to decorticate the anterior glenoid neck from 3 to 6 o'clock down to a bleeding cancellous bed — a 5 to 8 mm wide strip giving punctate bleeding (essential for labral-to-bone healing).
- Clear a clean 2 to 3 mm strip of labral remnants from the glenoid face where the anchors will sit.
- Remove only soft tissue and superficial cortex; do not excavate cancellous bone or create an iatrogenic defect. Bleeding is controlled with pump pressure (briefly 70 to 80 mmHg for burring, then back to 50 mmHg).
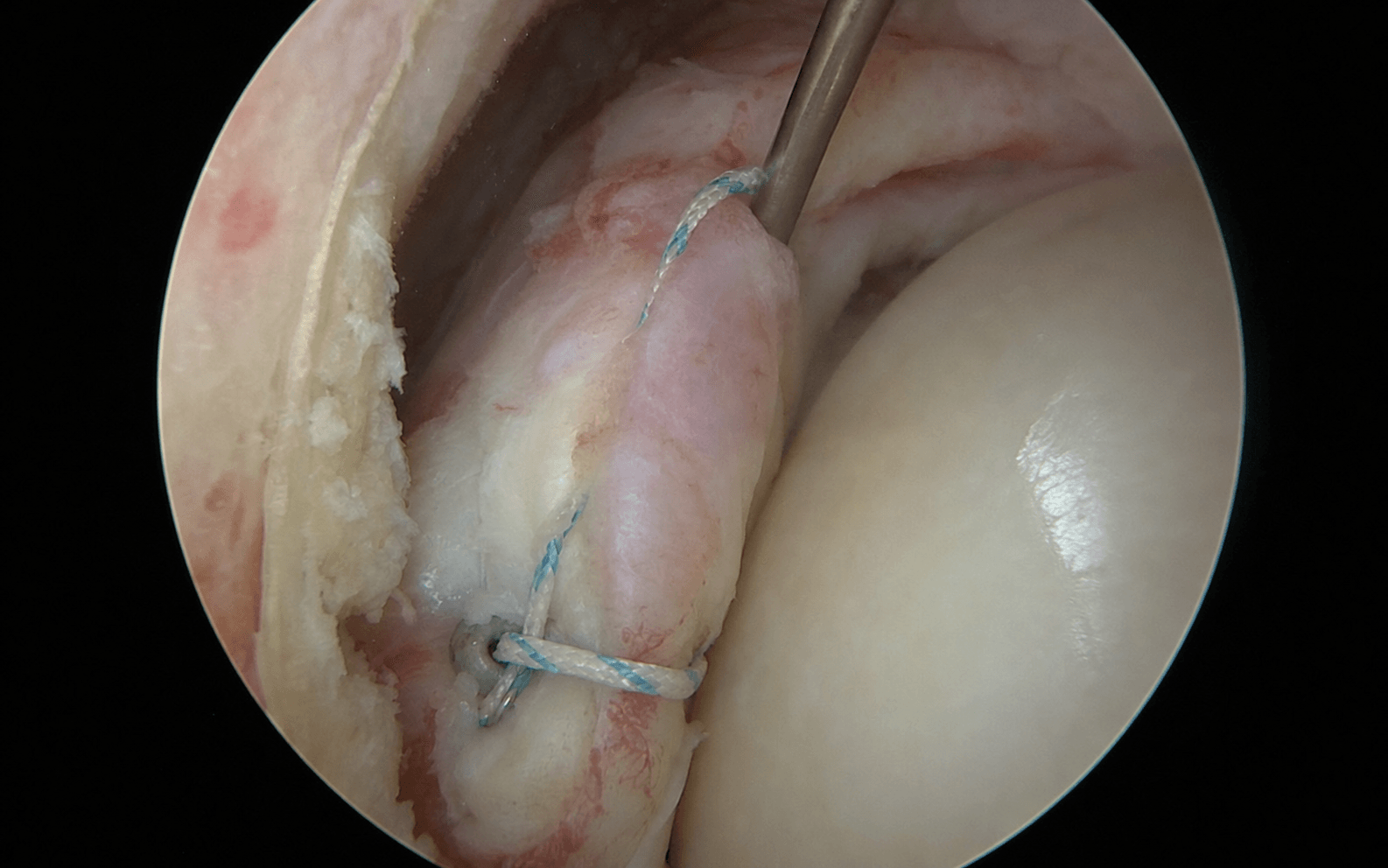
- Use 3.0 or 3.5 mm bioabsorbable or PEEK suture anchors (knotted or knotless). Start with the most inferior anchor at 5:30 (right) or 6:30 (left), then work superiorly: 4:30, 3:30, and 2:30 if needed — 3 to 4 anchors for a typical 3 to 6 o'clock lesion.
- Each anchor sits on the glenoid face 2 to 3 mm from the cartilage edge (NOT on the neck), drilled perpendicular to the glenoid surface and angled toward the glenoid centre (the deadman angle, about 45 degrees), to a depth of 15 to 20 mm until cortical purchase.
- Maintain 5 to 8 mm spacing between anchors on the surface; avoid converging drill holes that would fracture the bone bridges.
- Pass the suture device (BirdBeak/Spectrum penetrating, or Scorpion/Viper shuttle) through labrum AND capsule together as one unit, starting at the inferior anchor.
- Capture tissue 10 to 15 mm from the glenoid rim — this distance creates the capsular shift (reducing capsular volume from a pathologic 30 to 40 mL back to 15 to 20 mL and tensioning the IGHL). Capturing only 3 to 5 mm from the rim gives no shift.
- For the inferior anchor, ensure you capture the IGHL (palpate the thickened band) — it provides 60 to 70 percent of anterior restraint in abduction-external rotation and must be incorporated.
- Pass two limbs per anchor in a mattress or crossing pattern to distribute load.
- Retrieve and label each anchor's sutures; tie from inferior to superior (tying superior first loosens the inferior repair when you tension below).
- Knotted: sliding knot (SMC, Weston or Roeder) backed by 3 reversing half-hitches on alternating posts; tension to sit the labrum proud on the rim.
- Knotless: load the sutures into the anchor and advance it; tension is fixed by depth and cannot be adjusted after insertion.
- After each anchor, check external rotation at the side — maintain at least 30 to 40 degrees; accept a 10 to 15 degree loss as normal capsular tightening, but if ER falls under 20 degrees the repair is too tight and should be re-tied with less tension.
- Probe the repair: the labrum should be immobile, proud on the rim throughout, with no gaps or detachments; arthroscopic load-and-shift should show less than 5 mm translation.
- View from both portals to confirm no tissue bridges and no prominent knots.
- Remplissage (off-track Hill-Sachs with glenoid loss under 20 percent): create a posterolateral portal, mobilise the posterior capsule off the defect, place 1 to 2 anchors into the defect floor, and pass sutures through infraspinatus and posterior capsule to tenodese the tendon into the defect. Re-test in abduction-external rotation — the lesion should no longer engage.
- Decompress the joint (turn off the pump, drain fluid); remove cannulas.
- Irrigate each portal tract; close deep dermis with 3-0 absorbable monofilament and skin with 4-0 subcuticular Monocryl, Steri-Strips or glue.
- Bulky sterile dressing; arm in a sling in NEUTRAL rotation (not external). An abduction pillow is optional. No drains.
- Sling full-time for 4 to 6 weeks (removed only for shower, elbow/wrist/hand exercise and supervised therapy). No external rotation past neutral for the first 6 weeks.
- Pendulum (Codman) exercises from day 1; elbow/wrist/hand active ROM immediately; passive forward flexion and internal rotation from week 2 to 4.
- Analgesia: scheduled paracetamol 1 g six-hourly, plus or minus NSAIDs; a limited opioid supply for breakthrough pain; ice for the first 48 to 72 hours.
- Axillary nerve: runs along the inferior capsule at about the 6 o'clock position, an average of 5.4 cm (range 4 to 7 cm) from the lateral acromion edge. Keep the 5 o'clock portal within 5 to 7 cm of the acromion, use the outside-in needle first, and STOP all inferior mobilisation and anchor placement at 6 o'clock. Maintain pump pressure 40 to 60 mmHg so the capsule does not collapse onto the nerve. Injury rate 0.3 to 1 percent — the commonest nerve injury in shoulder arthroscopy.
- Musculocutaneous nerve: pierces the conjoint tendon 3 to 8 cm (mean 5.4 cm) distal to the coracoid. An anterior portal placed too medial (toward the coracoid) penetrates the conjoint tendon and risks it. Keep the portal in the rotator interval, lateral to the conjoint tendon.
- Suprascapular nerve: lies at the spinoglenoid notch 20 to 25 mm medial to the glenoid rim. A posterior portal placed too medial, or excessive medial mobilisation in posterior-labral work, endangers it.
- Superficial structures: the cephalic vein and deltopectoral interval lie over the anterior portal — sharp dissection through skin only, then blunt to the capsule; the anterior and posterior circumflex humeral vessels run with the axillary nerve along the inferior capsule.
Inadequate mobilisation — leaving the labrum scarred medially as an unreduced ALPSA — is the commonest technical cause of arthroscopic failure, accounting for 30 to 40 percent of revisions. Mobilise until you can see subscapularis muscle fibres through the thinned capsule and the labrum reaches the rim without tension. If dense scar prevents adequate mobilisation arthroscopically, convert to open rather than accept a medialsed repair.
Anchors on the glenoid FACE (2 to 3 mm from the cartilage edge) restore the anatomic labral bumper; anchors on the glenoid NECK create a medialsed ALPSA-type repair that provides no mechanical block and fails. Neck placement is the second commonest technical error. Start inferior (5:30), work superior, and confirm position from multiple viewing angles before loading sutures — once the anchor is in bone it cannot be moved.
Accept a 10 to 15 degree loss of ER as normal capsular tightening, but ER loss greater than 20 degrees is pathologic and predicts frozen shoulder. If ER falls under 20 degrees at the side after an anchor, release and re-tie with less tension or a smaller capsular shift, and release the rotator interval if it has been inadvertently closed.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation & motion | Therapy focus | |-------|--------|--------------------------|---------------| | 1 — Protection | 0 to 6 weeks | Sling full-time, neutral rotation; no ER past neutral; pendulums from day 1; passive elevation/IR from week 2 to 4 | Protect biological healing; prevent frozen shoulder | | 2 — Early motion | 6 to 12 weeks | Wean sling; active-assisted then active ROM; progress ER (20 to 30 degrees at week 6, 40 to 50 at week 8, full by week 12) | Restore passive ROM; scapular stabilisation | | 3 — Strengthening | 12 to 16 weeks | Progressive cuff/periscapular/deltoid strengthening; sport-specific non-contact drills; proprioception | Strength to 80 to 90 percent of the other side | | 4 — Return to sport | 16 to 24 weeks | Plyometrics; non-contact practice at 4 months, contact practice at 5 months, full competition at 6 months minimum | Full painless ROM, strength at least 90 percent, negative apprehension, sport-specific testing passed | Most patients return to any sport (about 85 percent overall, 65 percent to pre-injury level, contact athletes 73 percent), at an average of 6 months.
- Recognition
- Recurrent dislocation/subluxation, positive apprehension, re-detached labrum or capsular laxity on MRI, new bone loss on CT
- Prevention
- Correct selection (bone loss under 20%, on-track Hill-Sachs, ISIS under 6 counselled); complete mobilisation; anchors on face; capsular shift; no ER past neutral for 6 weeks; contact sport delayed to 6 months
- Management
- CT for bone loss: over 20% convert to Latarjet; under 15% with good tissue, revision arthroscopic (70 to 85% success); 15 to 20% add remplissage if engaging; poor tissue or multiple failures, Latarjet or bone graft
- Recognition
- ER loss greater than 20 degrees versus the other side; difficulty overhead or hand-behind-head; distinguish guarding (resolves by 3 months) from capsular contracture (beyond 6 months)
- Prevention
- Avoid over-tightening (check ER after each anchor, keep 30 to 40 degrees at side); no routine interval closure in isolated anterior instability; start passive ROM at 4 to 6 weeks
- Management
- Physiotherapy and capsular stretching; NSAIDs 6 to 8 weeks; if no gain by 6 months, manipulation under anaesthesia plus or minus arthroscopic capsular release (risks re-detaching the repair)
- Recognition
- Mechanical symptoms, painful arc, prominent anchor on the humeral head; CT/MRI lucency or backing out
- Prevention
- Perpendicular deadman trajectory; assess bone (use 3.5 mm in soft bone); 5 to 8 mm spacing; feel cortical purchase; 4 to 6 week immobilisation
- Management
- Prominent anchor: arthroscopic removal plus or minus replacement; pullout with instability: revision arthroscopic if bone adequate, else Latarjet; asymptomatic migration: observe
- Recognition
- Cannot abduct (deltoid paralysis), lateral shoulder numbness; deltoid atrophy at 2 to 3 weeks; EMG at 3 to 4 weeks
- Prevention
- 5 o'clock portal within 5 to 7 cm of acromion; outside-in needle first; stop inferior work at 6 o'clock; pump 40 to 60 mmHg; test deltoid in recovery
- Management
- Document immediately; most neuropraxia recovers in 3 to 6 months; sling to prevent subluxation; EMG at 3 to 4 weeks; explore if no recovery by 3 to 4 months (neurolysis, graft, or nerve transfer)
- Recognition
- Weak elbow flexion and supination, lateral forearm numbness
- Prevention
- Anterior portal through the rotator interval, NOT the conjoint tendon; outside-in needle; portal lateral to conjoint tendon, anterior to biceps
- Management
- Usually neuropraxia recovering over 3 to 6 months; EMG; explore at 4 to 6 months if severe (Oberlin transfer)
- Recognition
- Deep posterior/periscapular pain, positive O'Brien and Speed tests, new superior labral detachment on MRI
- Prevention
- Limit superior mobilisation to the zone of pathology; use a smooth elevator; drill the superior anchor carefully; document any pre-existing SLAP
- Management
- Intra-operative: repair the SLAP. Post-operative: physiotherapy 3 to 6 months, then revision; in patients over 40, favour biceps tenodesis over SLAP repair
- Recognition
- Scuffing or flaps seen intra-operatively; later mechanical symptoms, crepitus
- Prevention
- Careful instrument handling; keep the elevator on the neck not the cartilage; anchors 2 to 3 mm from the edge; bury knots; test ROM
- Management
- Grade 1 to 2 document only; grade 3 chondroplasty to stable edges; grade 4 size-dependent (microfracture or staging)
- Recognition
- Portal erythema/drainage at 3 to 7 days, or deep: pain out of proportion, effusion, raised markers; C. acnes presents late and needs 14-day anaerobic culture
- Prevention
- Cefazolin 2 g IV within 60 minutes; chlorhexidine-alcohol prep; plus or minus benzoyl-peroxide wash; minimise time and trauma; meticulous haemostasis
- Management
- Superficial: oral cephalexin or dicloxacillin. Deep: urgent arthroscopic washout, remove loose anchors, 3 to 5 cultures held 14 days, IV antibiotics tailored for 2 to 6 weeks; repeat washout if not improving
- Pre-operative planning: CT to quantify bone loss (over 15 percent rules out revision arthroscopy) and MRI to assess tissue quality; examine for hyperlaxity.
- Technical modifications: more aggressive mobilisation through scar, fresh anchor sites lateral to the old holes, 4 to 5 anchors, capsular plication, and remplissage if an engaging Hill-Sachs was not addressed.
- Outcomes: 70 to 85 percent success (60 to 70 percent in contact athletes). After 2 failed repairs, do NOT attempt further arthroscopy — Latarjet is mandatory.
Viva & Exam Focus
PORTALPORTAL — safe shoulder-arthroscopy portals
ANCHORSANCHORS — proper anchor placement in Bankart repair
Exits the quadrangular space with the posterior circumflex humeral artery, runs along the inferior capsule at about the 6 o'clock position (average 12 to 15 mm inferior to the rim), and lies an average of 5.4 cm (range 4 to 7 cm) from the lateral acromion. It is the commonest nerve injured in shoulder arthroscopy (0.3 to 1 percent). Protect it by keeping the 5 o'clock portal within 5 to 7 cm of the acromion, using the outside-in needle first, stopping all inferior work at 6 o'clock, and maintaining pump pressure at 40 to 60 mmHg. Test deltoid abduction in recovery.
A terminal branch of the lateral cord (C5 to C7) that pierces coracobrachialis 3 to 8 cm (mean 5.4 cm) distal to the coracoid tip, then runs between biceps and brachialis to become the lateral antebrachial cutaneous nerve. It is medial to the conjoint tendon at the level of the anterior portal. An anterior portal placed too medial or too inferior penetrates the conjoint tendon and injures it (0.1 to 0.5 percent). Keep the portal in the rotator interval, lateral to the conjoint tendon; if the needle aims toward the coracoid, it is too medial.
From the upper trunk (C5 to C6); supplies supraspinatus at the suprascapular notch and infraspinatus after passing around the scapular spine through the spinoglenoid notch, 20 to 25 mm medial to the glenoid rim. A posterior portal placed too medial, or excessive medial mobilisation in posterior-labral work, endangers it (under 0.5 percent in anterior Bankart; 3 to 5 percent in posterior labral repair). Injury presents as painless supraspinatus or infraspinatus atrophy with external-rotation weakness.
The cephalic vein runs in the deltopectoral interval superficial to the coracoid and conjoint tendon; the anterior and posterior circumflex humeral arteries form a ring around the surgical neck and run with the axillary nerve along the inferior capsule. Use sharp dissection through skin only, then blunt dissection to the capsule; bleeding is usually controlled by pump pressure. Major vascular injury needing open conversion is extremely rare (under 0.1 percent).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old elite rugby player has 3 documented anterior dislocations in 12 months (dominant shoulder), an anteroinferior labral detachment from 3 to 6 o'clock on MRI arthrogram, 15 percent glenoid bone loss by best-fit circle on CT, positive apprehension/relocation tests and a Beighton score of 1/9. Walk me through your decision between arthroscopic Bankart and Latarjet.”
“After mobilisation and anchor placement in a 25-year-old recreational netball player, the superior anchors (3:30, 2:30) have excellent bumper height, but the inferior 5:30 anchor shows the labrum sitting low — slightly medial on the neck rather than proud on the rim. It probes stable. What is the likely technical error, and how do you manage it intra-operatively?”
“You complete a 4-anchor knotted Bankart with capsular shift in a 28-year-old competitive tennis player. The repair looks excellent and probes stable, but external rotation at the side is only 15 degrees (45 degrees on the other side pre-operatively). What is the differential, what happens if you accept it, and what do you do now?”
Indications
- Recurrent traumatic anterior instability (2 or more dislocations, or 1 plus persistent subluxation/apprehension) with a Bankart lesion on MRI
- First-time dislocation in a high-risk patient: age under 25, competitive/contact or overhead athlete, ISIS under 6
- Glenoid bone loss under 20% and an on-track Hill-Sachs (over 20 to 25%, inverted-pear, or off-track = Latarjet, not Bankart)
Key anatomy
- Bankart = anteroinferior labral detachment (2 to 6 o'clock) with IGHL origin disruption
- IGHL is the primary anterior stabiliser — 60 to 70% of restraint in ABER; MUST be incorporated
- Labrum deepens the socket 50% and adds 30% surface area; restoring bumper height is the goal
- Posterior portal 2 cm inferior + 1 cm medial to posterolateral acromion; anteroinferior 5 o'clock portal is critical
- Axillary nerve at 6 o'clock, 5 to 7 cm from the acromion — STOP inferior work at 6 o'clock
Critical steps
- Portals: posterior (viewing), rotator interval (instrumentation), 5 o'clock (working) — spinal needle outside-in for all
- Diagnostic arthroscopy: 21-point exam, bare-spot bone-loss measure, Hill-Sachs engagement test; over 20% STOP
- Mobilise the capsulolabral complex as one unit until subscapularis fibres show through the capsule
- Decorticate the neck to bleeding bone; clean a 2 to 3 mm face strip
- 3 to 4 anchors, inferior (5:30) to superior, on the FACE 2 to 3 mm from cartilage, deadman angle
- Capture tissue 10 to 15 mm from the rim for capsular shift; incorporate the IGHL inferiorly
- Tie inferior to superior; restore the bumper; keep ER 30 to 40 degrees at the side
Danger zones
- Axillary nerve: 6 o'clock, 5 to 7 cm from acromion (0.3 to 1%)
- Musculocutaneous nerve: conjoint tendon 3 to 8 cm from coracoid (0.1 to 0.5%)
- Suprascapular nerve: spinoglenoid notch, 20 to 25 mm medial to the rim
- Cephalic vein and deltopectoral structures: superficial to the anterior portal
- Circumflex humeral vessels: along the inferior capsule with the axillary nerve
Technique pearls
- ISIS: age under 20 (2), competitive sport (2), contact/overhead (2), hyperlaxity (1), Hill-Sachs on AP (2), glenoid loss on AP (2); 6 or more = 70% failure
- Bone loss: under 13.5% safe, 13.5 to 20% gray zone, over 20 to 25% or inverted-pear = Latarjet
- Glenoid track = 0.83 x diameter minus bone loss; off-track Hill-Sachs needs remplissage
- Complete mobilisation is the number-one success factor (30 to 40% of failures if inadequate)
- 'Dance floor not hallway' — anchors on the face, not the neck
- Capsular shift by WHERE you capture tissue (10 to 15 mm from rim)
- Beach chair versus lateral: no outcome difference, surgeon preference
Complications
- Recurrence 5 to 8% overall, 10 to 15% contact, 15 to 25% revision
- Stiffness: 10 to 15 degree ER loss normal, over 20 degrees pathologic
- Anchor failure 2 to 5%
- Axillary nerve 0.3 to 1% (commonest nerve injury)
- Infection 0.3 to 0.5% — Cutibacterium acnes, 14-day culture
Post-op protocol
- Phase 1 (0 to 6 weeks): sling full-time neutral rotation, no ER past neutral, pendulums from day 1
- Phase 2 (6 to 12 weeks): wean sling, active ROM, scapular stabilisation; progress ER
- Phase 3 (12 to 16 weeks): strengthening, non-contact sport-specific drills
- Phase 4 (16 to 24 weeks): plyometrics; contact practice at 5 months, full competition at 6 months minimum
- Neutral-rotation sling for 4 to 6 weeks is standard — ER bracing shows no reproducible benefit
Background & Evidence
Lesion patterns and classification Anterior labral lesions take several forms that change the operative strategy: - Bankart (classic): the anteroinferior labrum is detached from 2 to 6 o'clock with good tissue quality.
- ALPSA (anterior labroligamentous periosteal sleeve avulsion): the labrum is detached but healed medially on the neck — the commonest chronic pattern (50 to 60 percent of recurrent instability) — demanding aggressive mobilisation.
- Perthes: the labrum is lifted off with intact periosteum, reduced in adduction but lifting in abduction (10 to 20 percent).
- GLAD (glenolabral articular disruption): an anterior labral tear with an associated chondral injury.
- Bony Bankart: an anterior glenoid-rim fracture with attached labrum; if the fragment is greater than 25 percent of glenoid width or displaced more than 5 mm, fix it with screws (ORIF), not suture anchors. Snyder's grading of anterior labral lesions: I frayed but attached; II detached (classic Bankart) with good tissue; III detached with a bucket-handle tear; IV detached with tissue loss or attenuation. ### Anatomy and biomechanics - Glenoid labrum: fibrocartilaginous, increasing effective depth by 50 percent and surface area by 30 percent; the anteroinferior labrum (2 to 6 o'clock) is the least vascular and the most often detached.
- IGHL complex — the primary anterior stabiliser (60 to 70 percent of restraint in abduction-external rotation): anterior band (2 to 4 o'clock), axillary pouch (5 to 7 o'clock), posterior band (7 to 9 o'clock).
- MGHL: primary restraint to anterior translation at 45 degrees abduction; absent in 8 to 30 percent; a Buford complex (cord-like MGHL with absent anterosuperior labrum) is a normal variant — do NOT repair it.
- SGHL: primary restraint to inferior translation in adduction; tightened by rotator-interval closure.
- Glenoid: pear-shaped, about 39 mm vertical by 29 mm transverse, 2 to 10 degrees retroverted; the bare spot is the anatomic centre.
- Dynamic stabilisers (about 70 percent of stability): rotator-cuff concavity-compression (effective with bone loss under 20 percent), scapular stabilisers, and the long head of biceps.
- Capsular volume rises from a normal 15 to 20 mL to 30 to 40 mL after multiple dislocations — the rationale for the capsular shift. ### Key evidence (verified) - Balg and Boileau (2007) — ISIS score validation in 131 patients; a score over 6 carried a 70 percent recurrence (p less than 0.001). Now the standard pre-operative risk tool.
- Burkhart and De Beer (2000) — 194 repairs; under 25 percent bone loss gave 4 percent recurrence versus 67 percent with an inverted-pear glenoid or engaging Hill-Sachs; contact athletes without bone defect 6.5 percent versus 89 percent with bone deficiency. Established the bone-loss paradigm.
- Di Giacomo, Itoi, Burkhart (2014) — the glenoid-track concept: on-track lesions recurred in 2.6 percent versus 18.9 percent off-track; dynamic testing 94 percent sensitive and 100 percent specific.
- Shaha et al. (2015) — 3D-CT in 194 patients; functional scores (WOSI) deteriorated once bone loss exceeded about 13.5 percent ('subcritical'), even without re-dislocation; quartile 4 (mean 24.5 percent) failed in 27.8 percent.
- Kavaja et al. (2018) — meta-analysis of 48 studies, 3,188 patients; overall recurrence 8.6 percent at a mean 3.8 years (contact athletes 13.2 percent versus 5.4 percent non-contact); revision rate 7.1 percent.
- Cho et al. (2018) — RCT of 2 versus 3 anchors; 12 percent versus 4 percent recurrence (p = 0.02) for lesions over 3 cm.
- Peebles et al. (2020) — meta-analysis of 9 studies, 957 patients; knotless 6.2 percent versus knotted 6.8 percent recurrence (equivalent), knotless 18 minutes faster with fewer knot complications (3 versus 8 percent).
- Paterson et al. (2010) — meta-analysis of immobilisation after FIRST-TIME (non-operative) dislocation in patients under 30; no benefit of conventional sling beyond 1 week (41 percent versus 37 percent recurrence, p = 0.52), and ER bracing not significantly better than IR (25 percent versus 40 percent, p = 0.07).
- Olds et al. (2015) — return to sport: 85 percent to any sport, 65 percent to pre-injury level; contact athletes 73 percent; average 6 months. ### Knotted versus knotless anchors Knotted anchors give surgeon-controlled tension and a long track record but take longer (3 to 5 minutes per knot) and carry knot-prominence and slippage risk; knotless anchors (PushLock, Iconix, Footprint) are faster and eliminate knot complications but fix the tension and cost more. Meta-analyses show equivalent recurrence (about 6 to 7 percent both), ROM and satisfaction at a minimum of 2 years. Adjuncts without proven benefit include PRP, bone-marrow aspirate and biologic scaffolds; thermal capsulorrhaphy is abandoned (30 to 50 percent recurrence, capsular necrosis). ### Guidelines, registries and global practice - AAOS (US) and ISAKOS/AANA consensus: arthroscopic Bankart for recurrent traumatic anterior instability with subcritical bone loss and an on-track Hill-Sachs; Latarjet favoured for critical glenoid loss, off-track bipolar lesions and high-demand contact athletes.
- BOA / BESS (UK) shoulder instability pathways emphasise structured bone-loss and glenoid-track assessment, reserving Latarjet for significant bone loss or failed soft-tissue repair.
- EFORT / European practice is broadly concordant, with rising primary-Latarjet use in young contact athletes reflecting the ISIS work.
- Convergent global threshold: critical glenoid bone loss around 20 to 25 percent (with growing recognition of a subcritical zone from about 13.5 percent) and an off-track Hill-Sachs shift the decision away from isolated arthroscopic Bankart.
- Registries: arthroplasty registries (NJR, AJRR, AOANJRR, Swedish, Norwegian) do not separately track instability soft-tissue procedures, but administrative data across countries show a sustained rise in both arthroscopic stabilisation and Latarjet over two decades. First-time dislocation in patients under 20 to 25 carries a 60 to 90 percent non-operative recurrence — the central driver of early surgical stabilisation worldwide.
- Antibiotic prophylaxis (globally consistent): a first-generation cephalosporin such as cefazolin 2 g IV (weight-adjusted) within 60 minutes of incision; for beta-lactam allergy, vancomycin 15 to 20 mg/kg or teicoplanin. Some units add anti-Cutibacterium cover and pre-operative benzoyl-peroxide skin prep, though routine clindamycin addition is debated and not universal. Redose cefazolin for prolonged procedures or major blood loss; a single peri-operative dose is standard.
References
The instability severity index score: a simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation
- Prospective case-control study of 131 consecutive patients undergoing arthroscopic Bankart with suture anchors; 14.5% recurrent instability at mean 31 months
- Six risk factors integrated into a 10-point pre-operative score: age under 20 at surgery, competitive/contact or overhead sport, hyperlaxity, Hill-Sachs on AP radiograph in external rotation, and loss of the sclerotic inferior glenoid contour
- A score over 6 points carried an unacceptable 70% recurrence risk (p less than 0.001)
Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion
- 194 consecutive arthroscopic Bankart repairs (suture-anchor technique), mean follow-up 27 months
- No significant bone defect: 4% recurrence; significant bone defect (inverted-pear glenoid or engaging Hill-Sachs): 67% recurrence
- Contact athletes without bone defect 6.5% recurrence vs 89% with bone deficiency
Evolving concept of bipolar bone loss and the Hill-Sachs lesion: from engaging/non-engaging to on-track/off-track lesion
- Introduced the glenoid-track method (radiographic and arthroscopic) to predict whether a Hill-Sachs lesion will engage the anterior glenoid rim
- If the Hill-Sachs lesion falls outside the glenoid track it is off-track (will engage); if within, on-track (will not engage)
- Integrates humeral-sided plus glenoid-sided (bipolar) bone loss into a single treatment paradigm
Redefining 'critical' bone loss in shoulder instability: functional outcomes worsen with 'subcritical' bone loss
- 73 shoulders after isolated arthroscopic Bankart repair, stratified by glenoid bone-loss quartiles; overall failure 12.3%
- WOSI functional scores deteriorated significantly once bone loss exceeded about 13.5%, even in patients who did not re-dislocate
- Bone loss was significantly higher in repairs that failed (24.7% vs 12.8%, p less than 0.01); quartile 4 (mean 24.5%) failure 27.8%
Position and duration of immobilization after primary anterior shoulder dislocation: a systematic review and meta-analysis
- Systematic review and meta-analysis of 9 Level I to II studies of immobilization after PRIMARY (non-operative) anterior dislocation
- In patients under 30: no benefit of conventional sling immobilization beyond 1 week (recurrence 41% for 1 week or less vs 37% for 3 weeks or more, p = 0.52)
- External-rotation bracing 25% vs internal-rotation sling 40% recurrence (p = 0.07, not statistically significant); age under 30 strongly predicted recurrence