Arthroscopic suture plication and balanced capsular shift for multidirectional instability with capsular redundancy · advanced
- Patient selection is everything: arthroscopic capsular shift and plication is indicated for atraumatic or multidirectional instability (MDI) with a patulous capsule after failed rehabilitation; patients with significant glenoid or humeral bone loss greater than 15-20 percent are better served by bone procedures such as Latarjet.
- The drive-through sign (easy passage of the arthroscope from posterior to anterior through the glenohumeral joint) indicates excessive capsular volume and is the key intraoperative marker for the need for plication; the degree of volume reduction must be titrated to avoid over-constraint.
- Balanced plication addresses anterior, posterior and inferior redundancy in a single procedure; isolated anterior or posterior plication risks creating iatrogenic unidirectional instability in the opposite direction.
- Rotator interval closure is performed only when the interval is patulous and contributes to inferior and posterior translation; excessive closure reduces external rotation and must be balanced against the capsular shift volume reduction.
- The axillary nerve lies 1.5-3 cm inferior to the inferior glenohumeral ligament (IGHL) and is at risk during inferior plication sutures; abduction and external rotation of the arm moves the nerve further from the capsule and is mandatory during inferior work.
- “The drive-through sign is positive when the arthroscope passes easily from posterior to anterior without resistance; a positive sign in a patient with symptomatic MDI supports capsular volume reduction rather than labral repair alone.
- “Over-tightening is the most common technical error: loss of external rotation greater than 20-30 degrees is poorly tolerated in overhead athletes and must be avoided by titrating the number and tension of plication sutures.
- “In MDI the capsule is often globally redundant; assess the rotator interval, anterior band of IGHL, posterior band of IGHL and axillary pouch separately and reduce volume in a balanced fashion.
- “Open inferior capsular shift remains the gold-standard volume-reducing procedure for severe MDI; arthroscopic plication achieves similar volume reduction when performed correctly but with less morbidity in appropriately selected patients.
When & Why
Indication. Symptomatic multidirectional or atraumatic shoulder instability with a documented patulous capsule, after failure of a structured rehabilitation programme of at least 6 months, and in the absence of significant bone loss. Confirm the diagnosis with a positive sulcus sign and positive apprehension in more than one direction, plus arthroscopic confirmation of global capsular redundancy and a positive drive-through sign. Relative indications include traumatic anterior instability with associated capsular stretch or redundancy in addition to a Bankart lesion, overhead athletes or throwers with a subtle MDI pattern that has failed non-operative management, and patients with connective-tissue disorders (Ehlers-Danlos, Marfan) and symptomatic laxity after failed rehabilitation. Assess the whole instability pattern before committing. Quantify glenoid bone loss (CT with 3D reconstruction or arthroscopic measurement) and humeral bone loss (the Hill-Sachs engagement test). The single decision that determines whether a soft-tissue plication is even appropriate is whether significant bone loss is present:
The default for MDI or atraumatic capsular redundancy with glenoid bone loss less than 15 percent. Balanced four-quadrant plication reduces volume 30-50 percent with less postoperative stiffness and faster recovery than an open shift.
The benchmark volume-reducing procedure. Preferred for severe global laxity or connective-tissue disorders where a more robust inferior shift is needed, or when the capsule is too friable to hold arthroscopic sutures.
Required when glenoid bone loss exceeds 15-20 percent or an engaging Hill-Sachs lesion is present. Soft-tissue plication alone will fail in this setting and recurrence is almost certain.
Contraindications. Absolute: glenoid bone loss greater than 15-20 percent or an off-track engaging Hill-Sachs lesion, active infection or uncontrolled inflammatory arthropathy, and a patient unable or unwilling to comply with the rehabilitation protocol. Relative: isolated unidirectional instability without capsular redundancy (better served by targeted labral repair), a previous failed capsular shift with scarring that precludes safe arthroscopic plication, and overhead athletes in whom even modest loss of external rotation would be career-ending. Consent specifically for residual stiffness and loss of external rotation, recurrent instability (5-12 percent), a small risk of axillary nerve injury (less than 1 percent with proper technique), chondral or suture abrasion, and (in connective-tissue disorders) a higher recurrence rate and the possibility of needing a revision or open procedure. Setup. Beach-chair position with the scapula supported and the arm free in a pneumatic or mechanical arm holder that allows controlled abduction, rotation and flexion. General anaesthesia with an interscalene block for postoperative analgesia; muscle relaxation is essential for adequate distraction and visualisation. Before any portal, perform a full examination under anaesthesia documenting range of motion, the sulcus sign, load-and-shift in anterior and posterior directions, and apprehension/relocation in multiple positions — this baseline defines how much plication is required.
The Operation
The goal is to reduce excessive capsular volume in a balanced fashion — taking up the redundant inferior, anterior and posterior capsule so the humeral head sits centred on the glenoid — while protecting the axillary nerve and preserving functional external rotation. The exposure is arthroscopic: standard posterior and anterior portals give access to the whole capsular ring. Capsular anatomy you must know before plication. The inferior glenohumeral ligament complex (IGHL) is the primary static restraint to inferior translation and the structure you are tightening. It has an anterior band (from the anteroinferior labrum at the 5-6 o'clock position to the humeral anatomic neck — restrains anterior and inferior translation in abduction and external rotation), a posterior band (from the posteroinferior labrum at the 7-8 o'clock position — restrains posterior and inferior translation in abduction and internal rotation), and the axillary pouch between them, which holds the majority of the excess volume in MDI. The rotator interval is the capsular gap between the superior border of subscapularis and the anterior border of supraspinatus, containing the coracohumeral and superior glenohumeral ligaments; when patulous it allows inferior and posterior translation. The drive-through sign — easy passage of the arthroscope from posterior to anterior across the joint — is your intraoperative measure of excessive volume, and its elimination is the endpoint of plication.
Operative sequence
- Beach-chair, scapula supported, arm in a holder allowing controlled rotation. Maintain 30-45 degrees of abduction and 20-30 degrees of external rotation for all inferior work — this maximises the distance between the inferior capsule and the axillary nerve.
- Posterior portal (primary viewing): 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion.
- Anterior portal (working): just lateral to the coracoid process and anterior to the acromion; a second 5 o'clock portal may be added for inferior work. Keep the anterior portal lateral to the coracoid to avoid neurovascular structures.
- Apply 5-7 kg of longitudinal traction in 30-45 degrees of abduction and 20-30 degrees of external rotation for distraction.
- Complete the examination under anaesthesia baseline (sulcus sign, load-and-shift, apprehension/relocation) and grade the sulcus 0-3+.
- From the posterior portal perform a systematic 360-degree inspection: labral integrity, chondral surfaces, rotator cuff, biceps anchor, and the capsule.
- Confirm the drive-through sign — attempt to drive the scope anteriorly across the joint; easy passage confirms excessive capsular volume.
- Apply inferior traction and grade the sulcus sign between the humeral head and glenoid; record the degree of inferior translation.
- Inspect the rotator interval from the posterior portal — a patulous interval appears as a large gap between subscapularis and supraspinatus with a visible coracoid. Decide here whether interval closure will be needed.
- The inferior capsule is addressed first because it holds the largest volume and is where the axillary nerve is at greatest risk. Keep the arm in 30-45 degrees abduction and 20-30 degrees external rotation throughout.
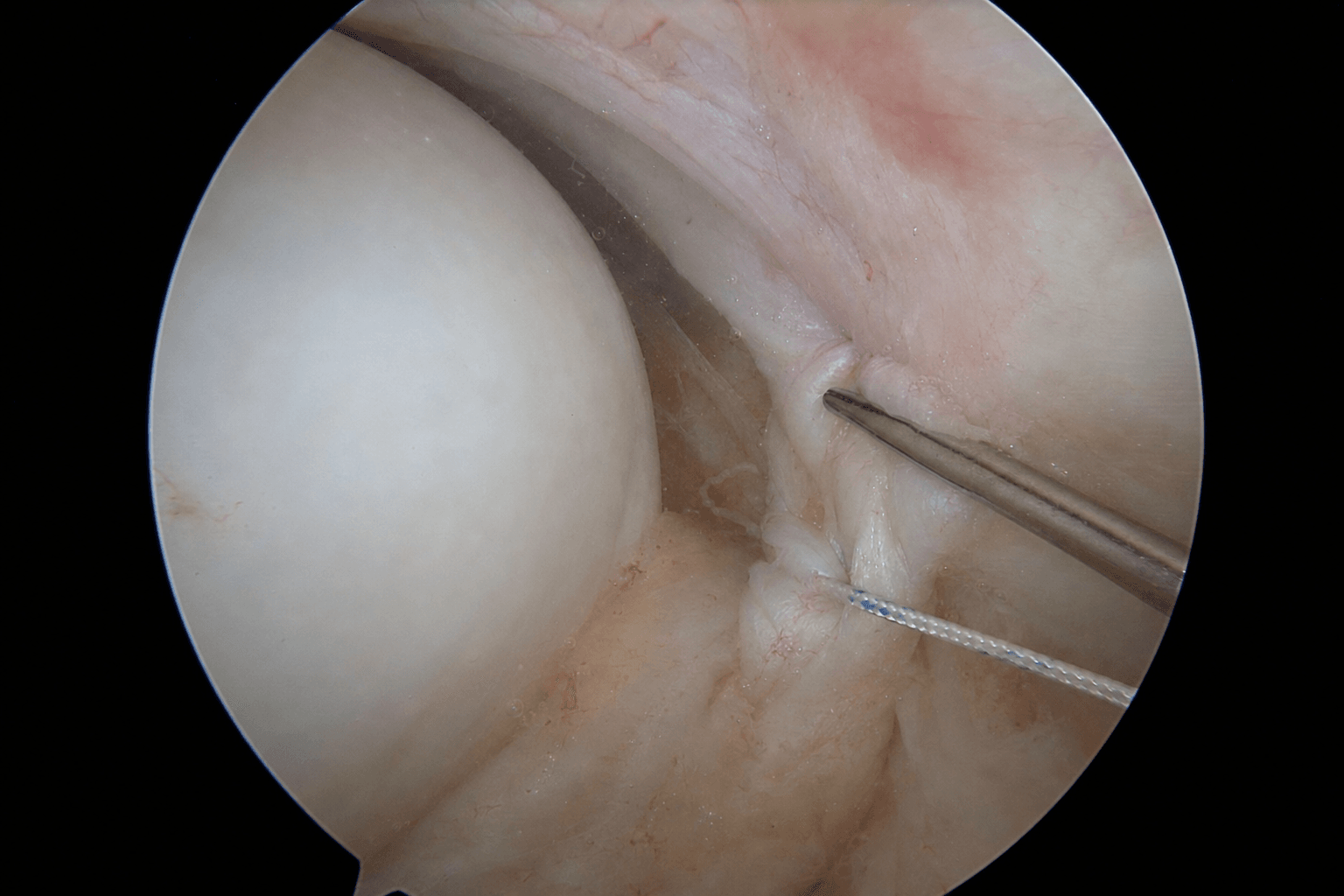
- Using a curved suture passer or shuttle relay from the anterior portal, pass non-absorbable suture (No. 2 FiberWire or equivalent) through the inferior capsule about 1 cm lateral to the labrum at the 6 o'clock position.
- Create a tuck or pleat (5-8 mm) that takes up the redundant capsule and advance the suture to the labrum or a small glenoid-rim anchor. Tie with the humeral head centred on the glenoid.
- Repeat at the 5 and 7 o'clock positions — typically 4-6 inferior sutures in total. Re-check the drive-through sign after each knot.
- Address the anterior band of the IGHL next: pass sutures from the 4-5 o'clock position anteriorly, creating tucks that reduce anterior redundancy and advance the capsule to the labrum.
- Then address the posterior band at the 7-8 o'clock position.
- The goal is balanced reduction. After each set, re-assess the drive-through sign and whether the humeral head stays centred. If the head tends to translate posteriorly after anterior plication, add posterior sutures to balance the shift — never plicate one side in isolation.
- Close the interval only when it is visibly patulous, when inferior translation persists after capsular plication, or when the sulcus sign remains 2+ after inferior and anterior plication.
- Pass a suture from the anterior portal through the superior glenohumeral/coracohumeral ligament complex on the glenoid side and then through the interval capsule on the humeral side.
- Tie with the arm in 30-45 degrees external rotation to avoid over-constraint. Do not close the interval in patients with pre-existing limited external rotation or in throwers who need maximum external rotation.
- Drive-through sign eliminated or markedly reduced.
- Sulcus sign reduced to 0 or 1+.
- Humeral head remains centred on the glenoid with axial loading in all positions.
- External rotation at 90 degrees abduction is within 10-15 degrees of the pre-operative examination-under-anaesthesia value.
- If external rotation is excessively limited, release one or two anterior or inferior sutures and re-tie with less tension.
- Address any Bankart or ALPSA lesion, SLAP tear, or partial-thickness rotator cuff tear before or after capsular plication as indicated — a positive drive-through sign in traumatic unidirectional instability may reflect labral pathology, and plication alone will fail if the labrum is not addressed.
- Perform biceps tenodesis or tenotomy if the biceps anchor is unstable.
- Remove portals with blunt dissection throughout; close the skin in layers.
- Apply a sling for comfort. Document the final external rotation achieved and the number of sutures used so the rehabilitation team understands the tensioning.
Suture, anchors and fixation. Non-absorbable braided polyethylene suture (No. 2 FiberWire, Orthocord or equivalent) is standard — strong enough to hold the plication through rehabilitation, small enough to minimise cartilage abrasion. Small glenoid-rim anchors (2.4-2.9 mm) loaded with non-absorbable suture are used when the labrum is attenuated or extra fixation is needed (placed at 5, 6 and 7 o'clock for inferior work, 3 and 9 o'clock for anterior/posterior); bioabsorbable or all-suture anchors are preferred in young patients to avoid permanent hardware. Knotless devices reduce operative time and knot prominence and are useful in the inferior quadrant where a knot stack can irritate the capsule. Use curved passers with protective sheaths to minimise chondral injury.
Before any inferior plication, confirm the arm is in 30-45 degrees of abduction and 20-30 degrees of external rotation — this maximises the distance between the inferior capsule and the axillary nerve (from about 1.5 cm up to 3.2 cm). Stay within 1 cm of the inferior labrum and pass sutures superficially in the capsule only. If the nerve lies too close, abort the most inferior suture and accept slightly less volume reduction rather than risk a nerve injury.
Perform inferior plication first with the arm abducted and externally rotated. Pass the suture through the capsule only 8-10 mm from the labrum, create a 5-8 mm tuck, and tie with the humeral head centred. Check after each knot that the drive-through sign is diminishing, and titrate the number of sutures against the preserved external rotation rather than chasing a fixed count.
Tying plication sutures with the humeral head translated anteriorly or posteriorly builds that translation into the construct and creates iatrogenic instability in the opposite direction. Re-centre the head on the glenoid before each knot, and add balancing sutures on the opposite side if the head shifts after a plication.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0-2 weeks | Sling for comfort only | Passive and active-assisted forward flexion to 90 degrees, external rotation to 30 degrees in the scapular plane; pendulums; isometric cuff activation | | 2 | 2-6 weeks | Wean sling as comfort allows | Active-assisted to full forward flexion, external rotation to 45-60 degrees; light scapular stabilisation; no resisted external rotation or elevation | | 3 | 6-12 weeks | None | Full active range of motion; progressive rotator-cuff and periscapular strengthening; proprioceptive and neuromuscular training | | 4 | 3-6 months | None | Sport-specific drills and plyometrics; graded throwing programme from 4-5 months; full return to contact or overhead sport at 6-9 months | Key milestones. By 6 weeks aim for external rotation at the side greater than 45 degrees and forward flexion greater than 140 degrees; by 3 months external rotation at 90 degrees abduction within 15 degrees of the contralateral side; by 6 months full symmetric range and motion and strength greater than 80 percent of the contralateral side. Expected outcomes. In appropriately selected patients the recurrence rate is 5-12 percent at 5 years, patient satisfaction is 85-92 percent, and 70-85 percent of overhead athletes return to their pre-injury sport level. Average loss of external rotation is 5-15 degrees and is titratable. The principal limitation in athletes is residual stiffness rather than recurrent instability. Factors associated with poorer outcomes include connective-tissue disorders (higher recurrence, may require an open shift), workers' compensation or litigation, non-compliance with rehabilitation, an over-ambitious return to sport before 6 months, and pre-existing glenohumeral arthritis. Patients with MDI and connective-tissue disorders carry a lifelong risk of recurrence in other joints — capsular shift addresses the shoulder but does not alter the underlying collagen disorder, so activity modification and ongoing strengthening are lifelong. Complications
- Recognition
- Recurrent subluxation or dislocation on history and examination
- Prevention
- Exclude bone loss pre-operatively; balanced plication; rehab compliance
- Management
- Revision arthroscopic or open shift; bone augmentation if bone loss is present
- Recognition
- External rotation reduced more than 20-30 degrees; fails to reach milestones
- Prevention
- Titrate plication under direct vision; document ER intra-operatively; begin early motion
- Management
- Therapy and stretching; rarely manipulation or selective suture release
- Recognition
- New deltoid numbness or weakness postoperatively
- Prevention
- Arm in abduction-external rotation for inferior work; stay within 1 cm of labrum; superficial passes only
- Management
- Usually neuropraxia — observe; persistent deficit warrants nerve exploration
- Recognition
- Pain or mechanical symptoms; arthroscopic cartilage damage
- Prevention
- Curved passers with protective sheaths; tie knots away from the articular surface; confirm anchor position
- Management
- Symptomatic management; arthroscopic removal of a prominent suture if needed
- Recognition
- Pain or weakness on internal rotation; portal irritation
- Prevention
- Blunt dissection; place the anterior portal lateral to the coracoid
- Management
- Conservative measures; rarely revision
Viva & Exam Focus
SHIFTSHIFT — balanced capsular plication principles
MDIMDI — patient selection criteria
Location. The axillary nerve exits the quadrilateral space and lies 1.5-3 cm inferior to the inferior glenohumeral ligament complex at the 6 o'clock position. Risk. Inferior plication sutures placed too far inferiorly or too deeply can transect or entrap the nerve; it is closest when the arm is adducted and internally rotated. The fix. Keep the arm in 30-45 degrees of abduction and 20-30 degrees of external rotation during inferior work, use a 1 cm safety margin from the inferior labrum, and pass sutures superficially in the capsule only.
The trap. Excessive anterior or inferior plication in an overhead athlete produces a permanent loss of external rotation and destroys throwing mechanics or a tennis serve. The fix. Titrate plication volume to the patient's sport and arm dominance. In throwers preserve at least 90-100 degrees of external rotation at 90 degrees abduction, and aim to restore external rotation within 10-15 degrees of the pre-operative examination-under-anaesthesia value.
The trap. A positive drive-through sign in a patient with traumatic unidirectional instability may reflect labral pathology rather than pure capsular redundancy — plication alone will fail if the labrum is not addressed. The fix. Always perform a 360-degree labral inspection and address any Bankart or ALPSA lesion before or during capsular plication, and interpret the drive-through sign in the context of the history and examination.
The trap. Complete rotator interval closure in a patient with pre-existing limited external rotation produces marked stiffness and is a common cause of revision surgery. The fix. Close the interval only when it is patulous and contributes to inferior translation on examination under anaesthesia, and close from the glenoid side to the humerus with the arm in 30-45 degrees external rotation.
The trap. Arbitrary plication without objective volume assessment leads to either under-correction (persistent instability) or over-correction (stiffness). The fix. Use the drive-through sign, the sulcus sign under anaesthesia, and the number of tucks needed to eliminate the drive-through as objective endpoints. A typical MDI capsule needs 4-6 plication sutures to reduce volume by 30-50 percent.
The trap. Treating a patient with subtle bone loss and unidirectional instability with capsular plication alone results in early recurrence and a failed operation. The fix. Quantify glenoid bone loss (CT with 3D reconstruction or arthroscopic measurement) and humeral bone loss (Hill-Sachs engagement test). If glenoid bone loss exceeds 15-20 percent or the Hill-Sachs lesion engages, proceed to bone augmentation rather than soft-tissue plication.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old university volleyball player has recurrent shoulder subluxation in multiple directions after failing 9 months of supervised physiotherapy. Examination under anaesthesia shows a 2+ sulcus sign, positive apprehension anteriorly and posteriorly, and a markedly positive drive-through sign. CT confirms glenoid bone loss of 8 percent and a non-engaging Hill-Sachs lesion. How do you proceed?”
“During arthroscopic capsular shift for a 28-year-old with MDI you have placed four inferior plication sutures and two anterior sutures. After tying, the drive-through sign is eliminated but external rotation at 90 degrees abduction is reduced from 110 degrees pre-operatively to 70 degrees. What do you do?”
“A 19-year-old gymnast with known Ehlers-Danlos syndrome had arthroscopic capsular shift for symptomatic MDI. At 8 months she has recurrent instability in the same shoulder and new symptomatic instability in the contralateral shoulder. What factors explain this and how do you counsel her?”
Patient selection
- MDI or atraumatic instability with a patulous capsule after greater than 6 months failed rehabilitation
- Glenoid bone loss less than 15 percent and a non-engaging Hill-Sachs lesion required for a soft-tissue procedure
- Positive drive-through and sulcus signs under anaesthesia confirm excessive capsular volume
- Overhead athletes need careful titration to preserve external rotation within 10-15 degrees of baseline
- Connective-tissue disorders carry higher recurrence — open shift or activity modification may be preferred
Key anatomy
- IGHL complex: anterior band (5-6 o'clock), posterior band (7-8 o'clock), axillary pouch (inferior redundancy)
- Rotator interval: a patulous interval contributes to inferior translation — close only when indicated
- Axillary nerve: 1.5-3 cm inferior to the IGHL at 6 o'clock — protect with arm abduction and external rotation
- Drive-through sign: easy arthroscope passage from posterior to anterior indicates global laxity
- Sulcus sign: inferior translation between the humeral head and glenoid quantifies inferior laxity
Technique principles
- Beach-chair with the arm in 30-45 degrees abduction and 20-30 degrees external rotation throughout
- Balanced four-quadrant plication: inferior first, then anterior and posterior to maintain head centering
- 4-6 plication sutures typically reduce volume 30-50 percent and eliminate the drive-through sign
- Rotator interval closure adds 10-15 percent volume reduction but reduces external rotation if excessive
- Final verification: drive-through eliminated, sulcus 0-1+, external rotation within 10-15 degrees of baseline
Danger zones and nerve protection
- Axillary nerve: arm abducted and externally rotated, stay within 1 cm of the labrum, superficial passes only
- Over-constraint: titrate tension; release sutures if external-rotation loss exceeds 20-30 degrees
- Humeral head centering: tie sutures with the head centred to avoid iatrogenic shift in the opposite direction
- Rotator interval: close only when patulous and contributing to residual inferior translation
- Bone loss: abort soft-tissue plication if glenoid loss is greater than 15 percent or a Hill-Sachs engages
Implants and fixation
- Non-absorbable No. 2 braided polyethylene suture (FiberWire, Orthocord) is standard
- Small glenoid-rim anchors (2.4-2.9 mm) used when the labrum is attenuated or extra fixation is needed
- Knotless devices reduce operative time and knot prominence in the inferior quadrant
- Bioabsorbable or all-suture anchors preferred in young patients to avoid permanent hardware
- Suture passers with protective sheaths minimise chondral injury
Complications
- Recurrence (5-12 percent): under-correction, missed bone loss, non-compliance, connective-tissue disorder
- Stiffness and ER loss: over-plication or excessive interval closure — titrate intra-operatively
- Axillary nerve injury (less than 1 percent): arm position, 1 cm safety margin, superficial suture passes
- Chondral abrasion: protective suture passers, knots tied away from the articular surface
- Portal complications: blunt dissection, anterior portal lateral to the coracoid
Rehabilitation milestones
- 0-2 weeks: sling for comfort, passive forward flexion to 90 degrees, external rotation to 30 degrees
- 2-6 weeks: wean sling, active-assisted motion, begin scapular stabilisation
- 6-12 weeks: full active motion, progressive rotator-cuff and periscapular strengthening
- 3-6 months: sport-specific drills, proprioceptive training, gradual return to overhead activity
- 6-9 months: full return to sport when strength and range of motion are symmetric and stability is demonstrated
Special situations
- Overhead athlete: preserve greater than 90 degrees external rotation at 90 degrees abduction
- Connective-tissue disorder: higher recurrence — consider an open shift and counsel about lifelong risk
- Failed previous plication: assess for bone loss, consider an open shift or bone augmentation
- Concomitant labral tear: address a Bankart or SLAP lesion before or during capsular plication
- Biceps pathology: tenodesis or tenotomy if the anchor is unstable; does not affect the capsular shift
Background & Evidence
Epidemiology. Multidirectional instability typically presents in the second and third decades and is common in overhead athletes, gymnasts and patients with generalised ligamentous laxity or a connective-tissue disorder. A substantial proportion of patients are bilateral. It is fundamentally a capsular-volume problem rather than a unidirectional soft-tissue tear, which is why dynamic-stabiliser rehabilitation is the first line and why volume reduction — not labral repair alone — is the operative goal when rehabilitation fails. Pathoanatomy. MDI arises from a globally redundant, patulous capsule rather than from a single discrete lesion. The inferior glenohumeral ligament complex is attenuated, the axillary pouch holds excess volume, and the rotator interval is often widened — together allowing inferior, anterior and posterior translation. In atraumatic MDI poor dynamic stabilisation (rotator cuff and periscapular weakness, altered proprioception) compounds the laxity. The drive-through sign is the arthroscopic correlate of this global redundancy. Comparison with the open inferior capsular shift. Open inferior capsular shift remains the benchmark volume-reducing procedure. Arthroscopic plication achieves a comparable reduction in capsular volume with less postoperative stiffness and faster recovery when performed by experienced surgeons on appropriately selected patients. In severe global laxity or connective-tissue disorders an open shift may still be preferred for a more robust inferior shift.
- Arthroscopic plication
- 30-50 percent
- Open inferior capsular shift
- 40-60 percent
- Arthroscopic plication
- 5-12 percent at 5 years
- Open inferior capsular shift
- 3-8 percent at 5 years
- Arthroscopic plication
- 5-15 degrees (titratable)
- Open inferior capsular shift
- 10-25 degrees (more consistent)
- Arthroscopic plication
- 70-85 percent
- Open inferior capsular shift
- 60-75 percent
- Arthroscopic plication
- less than 1 percent (with protection)
- Open inferior capsular shift
- 1-3 percent
- Arthroscopic plication
- 8-15 percent
- Open inferior capsular shift
- 5-10 percent
Key evidence. Cadaveric work quantifies what the operation achieves: 4-6 plication sutures placed in a balanced four-quadrant fashion reduce glenohumeral volume by 30-50 percent, comparable to an open shift, while rotator interval closure adds a further 10-15 percent reduction (at the cost of 10-25 degrees of external rotation if over-closed). Cadaveric mapping of the axillary nerve shows that abduction and external rotation increase the nerve-to-capsule distance from about 1.5 cm to 3.2 cm, and that sutures placed within 1 cm of the inferior labrum with the arm adducted place the nerve at highest risk — the anatomical basis for the arm-position rule. Clinical series of arthroscopic plication in MDI report recurrence rates of 5-12 percent at 2-5 years with appropriate selection, and overhead-athlete return-to-sport rates of 70-85 percent, with over-constraint (external-rotation loss greater than 20 degrees) the principal cause of failure to return. A randomised comparison of open and arthroscopic capsular shift found no significant difference in recurrence or patient-reported outcomes at 5 years, with less stiffness and faster return to work in the arthroscopic group.
References
Multidirectional instability of the shoulder: surgical techniques and clinical outcome
- Modern review of arthroscopic capsular shift and plication techniques for MDI with emphasis on balanced volume reduction
The Arthroscopic Trillat Procedure Is a Valuable Treatment Option for Recurrent Anterior Instability in Young Athletes With Shoulder Hyperlaxity
- Arthroscopic bony procedure combined with capsular management effective in hyperlaxity cases
Risk factors for early failure after thermal capsulorrhaphy
- Early experience with thermal capsular shrinkage highlights importance of mechanical plication over thermal methods alone
T-plasty modification of the Bankart procedure for multidirectional instability of the anterior and inferior types
- Foundational description of capsular shift principles in MDI by the Altchek group
Arthroscopic capsular plication for multidirectional shoulder instability
- Original description of the arthroscopic capsular shift technique in 40 patients with MDI
- Demonstrated 85 percent good-to-excellent results with balanced anterior and inferior plication
- Established the principle of titrating capsular volume reduction to avoid stiffness
Capsular volume reduction after arthroscopic plication: a cadaveric study
- Cadaveric quantification showing 4-6 plication sutures reduce glenohumeral volume by 30-50 percent
- Balanced four-quadrant plication superior to isolated anterior or posterior shifts
- Rotator interval closure adds 10-15 percent additional volume reduction
Arthroscopic treatment of multidirectional shoulder instability in athletes
- Prospective series of 58 overhead athletes with MDI treated with arthroscopic plication
- Recurrence rate 7 percent at 3 years; 78 percent returned to pre-injury sport level
- Over-constraint (loss of external rotation greater than 20 degrees) was the main cause of failure to return to sport
Open versus arthroscopic capsular shift for multidirectional instability: randomised trial
- Randomised comparison of open inferior capsular shift versus arthroscopic plication in 72 patients with MDI
- No significant difference in recurrence or patient-reported outcomes at 5 years
- Arthroscopic group had less postoperative stiffness and faster return to work
Axillary nerve proximity during arthroscopic inferior capsular plication
- Cadaveric study mapping axillary nerve distance from the inferior capsule in varying arm positions
- Abduction and external rotation increased the nerve-to-capsule distance from 1.5 cm to 3.2 cm
- Sutures placed within 1 cm of the inferior labrum with arm in adduction placed the nerve at highest risk