Dual-row fixation with a suture-bridge configuration to maximise footprint contact, restore the anatomic insertion and optimise biomechanical strength for medium to large rotator cuff tears
- Dual-row fixation: medial-row anchors at the articular margin secure the tendon edge where the native cuff inserted, while lateral-row knotless anchors placed 10–15 mm lateral create a suture bridge compressing the tendon across the full 15–18 mm anatomic footprint — recreating the native enthesis.
- Biomechanical superiority: footprint contact area 60–80 percent versus 30–50 percent single-row, contact pressure 3–5 times higher, and ultimate failure load 20–40 percent greater — but this translates into a clinical advantage only for LARGE tears greater than 3 cm.
- Evidence-based indications: large tears greater than 3 cm show a 15–20 percent absolute reduction in re-tear rates with double-row (20–30 percent versus 35–45 percent single-row); small-medium tears show equivalent outcomes — technique selection must be tear-size specific.
- Tension-free mobilisation is the most important step: a tendon reduced to the lateral footprint without tension is the foundation of healing. Inadequate mobilisation dooms the repair regardless of how elegant the construct appears.
When & Why
Indication. A double-row / transosseous-equivalent suture-bridge repair is indicated for medium to large full-thickness posterosuperior cuff tears (roughly 2–5 cm) in active patients with adequate tissue quality and reparability, where restoring the anatomic footprint and maximising tendon-bone contact is most likely to translate into durable structural healing. The evidence supports a meaningful reduction in re-tear rates with double-row for large tears greater than 3 cm; for small-medium tears (less than 3 cm) outcomes are equivalent to single-row, which remains the faster, lower-cost default in that subgroup. Assess the whole tear before committing. Confirm that the tissue can actually be repaired double-row by evaluating four things together:
- Size (Cofield: small less than 1 cm, medium 1–3 cm, large 3–5 cm, massive greater than 5 cm) — double-row is most useful for medium-large tears.
- Pattern — crescent (direct repair), U-shaped (margin convergence first), L-shaped (repair the apex first), or massive.
- Retraction (Patte) — Stage 3 retraction to the glenoid is often irreparable.
- Muscle quality (Goutallier on MRI) — Grade 3–4 fatty infiltration predicts poor healing regardless of construct. Contraindications. Massive irreparable tears (Patte Stage 3 retraction with Goutallier Grade 3–4), severe osteoporosis (poor anchor purchase), and tissue that will not reach the lateral footprint even after complete mobilisation — in each, a medialiszed single-row repair, partial repair, superior capsular reconstruction (SCR) or reverse arthroplasty is more appropriate than forcing a double-row under tension. The one decision that matters. Once a double-row strategy is chosen, the construct variant is largely preference:
Medial double-loaded anchors at the articular margin; knotless lateral anchors capture the medial suture tails to create horizontal bridges across the footprint. The most common double-row configuration in current practice.
All-knotless construct using high-strength tape or suture; faster to assemble with less subacromial bulk, and biomechanically comparable.
Three suture pairs per medial anchor (six sutures) give greater lateral footprint coverage and suture density, at the cost of more complex suture management.
Knots tied at both rows — the original technique. Greater subacromial bulk and impingement risk mean it is now less commonly used.
Consent specifically for re-tear (10–20 percent overall, higher for large tears), stiffness (8–15 percent), infection (less than 1 percent), nerve injury (suprascapular or axillary), anchor-related problems, and persistent symptoms despite an intact repair. Setup. Beach-chair position is preferred: head elevated 60–70 degrees, arm in a pneumatic holder with 10–15 lbs of gentle traction, 20–30 degrees of abduction and neutral rotation — allowing dynamic range-of-motion testing of the finished repair. Lateral decubitus with the arm in 45 degrees of abduction, 20 degrees of forward flexion and balanced traction is the alternative.
The Operation
The goal is to expose and clear the subacromial space, mobilise the tendon back to its anatomic footprint without tension, then build a double-row suture-bridge construct — medial fixation at the articular margin and lateral compression across the full 15–18 mm footprint — and confirm it is stable through a dynamic range-of-motion test. The exposure (positioning, portals, bursectomy) is laid out inline as the opening steps, because everything that follows depends on it.
Operative sequence
- Beach chair, 60–70 degrees upright; pneumatic holder with 10–15 lbs traction, arm in 20–30 degrees abduction and neutral rotation.
- Mark the acromion, clavicle, coracoid and scapular spine; inject 30–50 ml of saline with epinephrine (1:300,000) for distension and haemostasis.
- Establish the posterior viewing portal at the soft spot, 2 cm inferior and 1 cm medial to the posterolateral acromion corner.
- Run a systematic glenohumeral exam: biceps (manage if more than 50 percent torn or unstable), subscapularis (comma sign), labrum, cartilage and ligaments — 40–50 percent of cuff tears have concomitant pathology that must be treated.
- Assess the cuff from the articular side, knowing the articular view underestimates tear size — the bursal view shows the true extent.
- Outside-in with a spinal needle: 3 cm lateral to the lateral acromion edge, in line with the posterior clavicle (Nevasier).
- This single portal must give a perpendicular trajectory to BOTH the articular margin (medial row) and the lateral footprint (lateral row) — the make-or-break of double-row repair.
- Confirm the trajectory from inside-out before placing the cannula; keep all portals greater than 5 cm from the acromion to protect the axillary nerve.
- Camera posterior, shaver and radiofrequency via the lateral portal; work in quadrants, anterior-to-posterior and medial-to-lateral.
- Excise all bursal tissue until the field is crisp: acromion undersurface, coracoacromial ligament, the full tear with anterior and posterior margins, the greater-tuberosity footprint and the humeral head.
- Take 15–20 minutes if needed — poor visualisation guarantees a poor repair, and double-row demands a clear view of both the articular margin and the lateral footprint.
- Classify morphology (Bigliani: Type I flat 15 percent, Type II curved 70 percent, Type III hooked 15 percent).
- Level 1 evidence shows no outcome difference between cuff repair performed with versus without acromioplasty — reserve decompression for a genuine Type III hook or mechanical outlet impingement.
- If performed, burr the anteroinferior acromion 3–5 mm to a smooth gliding surface and preserve the deltoid origin.
- From the bursal side, document SIZE (Cofield), PATTERN (crescent / U-shaped / L-shaped / massive), RETRACTION (Patte) and correlate QUALITY with the preoperative Goutallier grade.
- Crescent tears — direct repair; U-shaped — margin convergence first; L-shaped — repair the apex (corner stitch) first.
- Confirm the tissue will reach the lateral footprint after mobilisation, otherwise plan a medialiszed single-row from the outset.
- Release ALL adhesions: superior (acromion / CA ligament), medial (glenoid / superior capsule), lateral (deltoid) and inferior (capsule — mind the axillary nerve).
- For chronic retracted tears add anterior and posterior interval slides (10–15 mm of excursion each); the suprascapular nerve lies 2–3 cm medial to the glenoid, so keep medial releases within 2 cm and blunt.
- For U-shaped tears, margin convergence side-to-side sutures reduce footprint strain by 30–40 percent.
- Test of adequacy: with the arm at the side in neutral rotation, the tendon must reach the lateral footprint edge without tension — if not, do not proceed with double-row under tension.
- Define the anatomic footprint: supraspinatus on the superior facet (about 15 mm AP x 25 mm SI), infraspinatus on the posterior facet (about 20 mm AP x 25 mm SI); medial border at the articular margin, lateral edge 15–18 mm lateral.
- Clear soft tissue and decorticate GENTLY to punctate bleeding bone — do not create a deep trough, which weakens anchor fixation.
- Mark the medial-row position (articular margin) and the lateral-row position (10–15 mm lateral), preserving lateral bone stock.
- Place 2–3 double-loaded anchors (2 for medium, 3 for large tears) AT the articular margin, 8–10 mm apart, spanning the tear anterior-to-posterior.
- Insert via the lateral portal at a 45-degree deadman angle perpendicular to the articular surface; tap the pilot hole, seat flush or 1 mm below cortex, and test security with a gentle pull.
- Colour-code and retrieve suture limbs systematically (8–12 limbs in total); knotless medial anchors are increasingly preferred — faster, less bulk, equivalent strength.
- Pass mattress sutures 5–10 mm from the medial tear edge (too close risks cut-through), the second limb 5 mm lateral, capturing 8–10 mm of tissue per mattress.
- A mattress configuration gives roughly twice the failure load of simple sutures — important in degenerative tissue prone to cut-through.
- Aim for 5–8 mm of full-thickness tendon bite; choose the best-quality tissue available.
- Knotless (preferred): tension the tendon to the margin and seat the knotless anchors — faster, less subacromial bulk.
- Knotted: retrieve both limbs of each mattress through one cannula, tie a sliding-locking knot (SMC / Revo) plus three alternating half-hitches; keep knots low-profile and posterior.
- The endpoint is the medial tendon edge at the articular margin — no gap, no blanching. Over-tensioning causes ischaemia and cut-through.
- Place 2–3 KNOTLESS lateral anchors 10–15 mm lateral to the medial row, in line with the medial anchors.
- Carry the medial suture tails over (or through) the lateral tendon edge; the knotless anchor captures them and tensions the bridge on insertion.
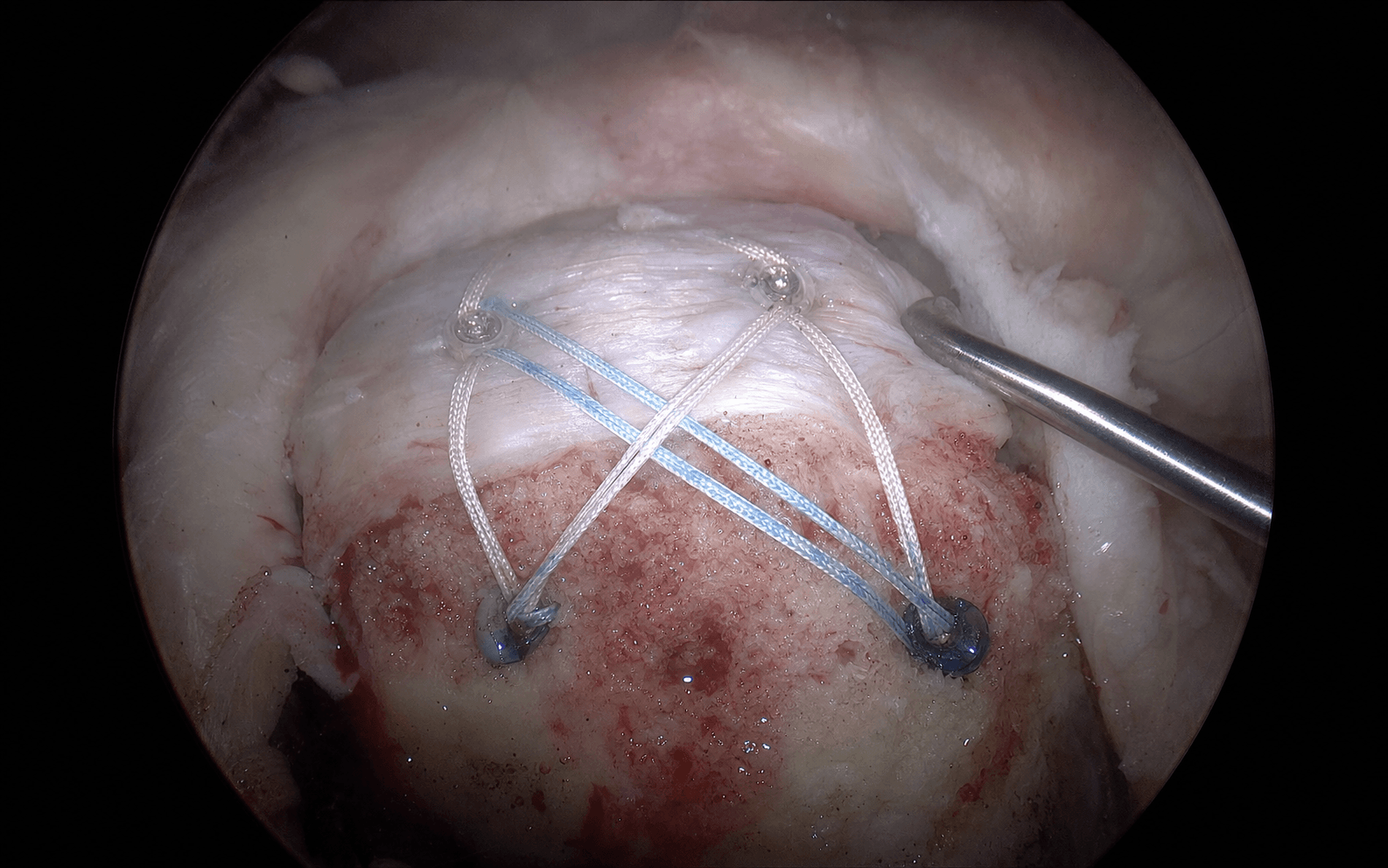
- The result is horizontal suture bridges compressing the tendon across the whole 15–18 mm footprint — the hallmark of the TOE construct (60–80 percent footprint contact versus 30–50 percent single-row).
- For U-shaped tears, add 2–3 side-to-side convergence sutures to convert the U into a crescent and off-load the footprint repair.
- Inspect the finished construct: parallel, untangled bridges; taut compression without blanching or bunching; complete footprint coverage with no gaps.
- Remove traction and take the arm through passive forward flexion, abduction and rotation while watching the repair continuously.
- Probe-test: the construct should feel rock-solid with no gapping under moderate force. If it gaps with normal ROM it is over-tensioned — remove the lateral row and re-tension.
- Confirm there is no subacromial impingement of the construct.
- Final 360-degree inspection: no loose suture or anchor fragment in the joint (chondrolysis risk), repair intact, hemostasis secured; irrigate copiously (3–6 L).
- Close portals (posterior and lateral 3-0 nylon, anterior 4-0 monocryl); consider a subacromial injection of 20 ml of 0.25 percent bupivacaine for pain control.
- Immobilise in an abduction brace or sling with abduction pillow at 30–45 degrees — this reduces supraspinatus tension versus an arm-at-side position and protects biological healing.
Inadequate mobilisation is the number-one cause of cuff-repair failure — a tendon fixed under tension will cut through regardless of how elegant the construct looks. Before any fixation, confirm the tendon reaches the lateral footprint with the arm at the side in neutral rotation, tension-free. During medial releases remember the suprascapular nerve lies 2–3 cm medial to the posterior glenoid rim: keep medial dissection within 2 cm, use blunt technique, and never place thermal devices or medial anchors beyond the safe zone — an injury here denervates both supra- and infraspinatus and is difficult to salvage.
A single lateral portal 3 cm lateral to the acromion in line with the posterior clavicle (Nevasier) must give a perpendicular trajectory to BOTH the articular margin and the lateral footprint. Confirm the line with a spinal needle from inside-out before committing. A portal too medial cannot reach the lateral row; one too inferior endangers the axillary nerve (keep all portals greater than 5 cm from the acromion).
Multiple Level 1 trials show no difference in pain, function or re-tear rates when cuff repair is performed with versus without acromioplasty. Reserve decompression for a genuine Type III hook or mechanical outlet impingement; when you do burr, take only 3–5 mm of anteroinferior acromion to a smooth surface and protect the deltoid origin.
With the arm at the side and neutral rotation, grasp the tendon and pull laterally — it must reach the lateral footprint edge without tension. If it will not, add interval slides; if it still will not, convert to a medialiszed single-row. A tension-free repair with adequate coverage always beats a maximally tensioned repair with complete coverage.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation & motion | Goal | |-------|--------|--------------------------|------| | 1 — Protection | 0–6 weeks | Abduction brace 30–45 degrees, 24/7; passive ROM only (pendulums, passive FF to 90–120 degrees, passive ER to 30 degrees); no active or resisted motion | Protect biological healing; prevent stiffness | | 2 — Active motion | 6–12 weeks | Wean brace to sling (week 6–8), sling off by week 10; active-assisted then full active ROM; light isometrics week 10–12 | Restore full active ROM | | 3 — Strengthening | 12–20 weeks | Progressive resistance (Theraband, then light weights 1–3 lb advancing to 3–8 lb); scapular stabilisation and proprioception | Restore strength | | 4 — Return to activity | 20+ weeks | Full strengthening and sport-specific training; desk work 2–3 weeks, light duty 3 months, manual labour 5–6 months, overhead sports 6–9 months | Functional return | Biological maturation continues for 12–18 months, so further improvement can be expected late. Immobilisation compliance is critical — non-compliance drives re-tear. Complications
- Recognition
- Recurrent pain, weakness, positive lag signs; MRI shows a retracted tendon with a gap at the footprint; may be asymptomatic in the elderly
- Prevention
- Tension-free mobilisation, appropriate patient selection, avoid repairing massive tears with Goutallier 3–4, strict 6-week immobilisation, smoking cessation
- Management
- Small and asymptomatic — observe; symptomatic and active — revision repair if tissue adequate, SCR if irreparable, reverse arthroplasty if arthritis develops
- Recognition
- Progressive loss of passive ROM (especially external rotation), end-range pain, capsular pattern, normal X-rays
- Prevention
- Early passive ROM from week 2–3, avoid immobilisation beyond 6 weeks, patient education, NSAIDs
- Management
- Therapy and NSAIDs; intra-articular steroid after 8 weeks; manipulation under anaesthesia at 3–4 months; arthroscopic capsular release if persistent beyond 6 months
- Recognition
- Increasing pain, erythema, warmth, drainage, fever, raised inflammatory markers, positive cultures
- Prevention
- Chlorhexidine wash, prophylactic cefazolin, sterile technique, minimise operative time, glycaemic control
- Management
- Early (less than 3 weeks) — arthroscopic debridement and 6 weeks IV antibiotics, retain implants; late — debridement, implant removal, long-term antibiotics, staged reconstruction
- Recognition
- Sudden pain or pop (pull-out), mechanical symptoms, painful arc (prominence); imaging shows displaced or intra-articular anchor
- Prevention
- Assess bone stock, 45-degree deadman angle, countersink flush, right-size anchor, avoid osteoporotic bone
- Management
- Pull-out — revision if early; prominent anchor — arthroscopic removal and replacement; intra-articular anchor — immediate removal to prevent chondrolysis
- Recognition
- Progressive supra-/infraspinatus atrophy, weakness in abduction and external rotation; EMG confirms denervation
- Prevention
- Keep medial releases within 2 cm of the glenoid, blunt dissection, no thermal devices medially (nerve 2–3 cm medial to glenoid)
- Management
- Observe 3–6 months for neuropraxia; nerve decompression if no recovery (limited success); periscapular strengthening
- Recognition
- Deltoid weakness, loss of shoulder abduction, sensory loss over the lateral deltoid patch; EMG confirms
- Prevention
- All portals greater than 5 cm from the acromion, no inferior portals, care with inferior releases
- Management
- Most are neuropraxias — observe 3–6 months; explore if no recovery by 6 months
- Recognition
- Imaging shows the medial row pulled out with the lateral row still fixed — an over-tensioned lateral row
- Prevention
- Balanced tensioning; never seat the lateral row against an inadequately mobilised tendon
- Management
- Recognise intra-operatively, remove the lateral row, re-mobilise, re-tension or convert to single-row
Other important problems. Persistent pain despite an intact repair (10–15 percent) is usually multi-factorial — pre-existing arthritis, biceps or AC-joint pathology, or cervical radiculopathy — and is managed with diagnostic injections and treatment of the concomitant pathology. Residual weakness relates to pre-existing atrophy and fatty infiltration (Goutallier 3–4), age greater than 65 and tear size, and is best prevented by appropriate patient selection. Subacromial impingement from a bulky construct or prominent knots (2–5 percent) is reduced by knotless designs and managed by arthroscopic debridement if symptomatic.
Viva & Exam Focus
MEDIALMEDIAL — medial-row anchor position
BRIDGEBRIDGE — suture-bridge construct principles
- Course & location
- Exits the quadrangular space 5–7 cm inferior to the acromion, then wraps anteriorly around the surgical neck of the humerus
- How to protect it
- Keep all portals greater than 5 cm from the acromion; no inferior portals; care with inferior capsular releases
- Course & location
- Through the suprascapular notch under the transverse scapular ligament, then 2–3 cm medial to the posterior glenoid rim along the scapular spine; supplies supra- then infraspinatus
- How to protect it
- Keep medial releases within 2 cm of the glenoid; blunt dissection; no thermal devices or medial anchors beyond the safe zone
- Course & location
- Enters coracobrachialis 3–8 cm distal to the coracoid (variable), then runs between biceps and brachialis
- How to protect it
- Keep anterior portals superior and lateral to the coracoid; no deep rotator-interval dissection
- Course & location
- Accompanies the axillary nerve through the quadrangular space and around the surgical neck
- How to protect it
- Avoid aggressive inferior cuff mobilisation; care with thermal devices near the inferior capsule
- Course & location
- Runs in the deltopectoral groove, draining to the axillary vein
- How to protect it
- Mainly at risk in mini-open conversion; identify and protect laterally in a deltopectoral split
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old manual labourer has a 4 cm full-thickness supraspinatus tear and wants the 'best repair possible'. What is the evidence comparing double-row to single-row, and what would you recommend?”
“Describe the suture-bridge construct in detail. What are its biomechanical advantages over single-row repair, and why do these not always translate to better clinical outcomes?”
“During a double-row repair you complete the medial row, but tensioning the lateral row is pulling the medial row out. What is happening, what are the implications, and how do you prevent or manage this?”
Indications
- Medium to large full-thickness posterosuperior tears (about 2–5 cm) with adequate tissue and reparability
- Active patients, typically less than 70, with high demand, good tissue quality, non-smokers
- Evidence supports double-row for LARGE tears greater than 3 cm (15–20 percent lower re-tear); small-medium tears are equivalent to single-row
- Contraindicated: massive irreparable (Patte 3, Goutallier 3–4), severe osteoporosis, tissue that will not reach the lateral footprint
Key anatomy
- Supraspinatus footprint: superior facet of greater tuberosity, about 15 mm AP x 25 mm SI; medial border at the articular margin, extends 15–18 mm lateral
- Articular margin = cartilage-bone junction = exact medial-row anchor position
- Suprascapular nerve: 2–3 cm medial to the posterior glenoid rim (at risk in medial mobilisation)
- Axillary nerve: 5–7 cm inferior to the acromion — all portals greater than 5 cm
- Lateral portal: 3 cm lateral to the acromion in line with the posterior clavicle (Nevasier) — perpendicular to both rows
Critical steps
- Glenohumeral arthroscopy: treat concomitant pathology (biceps, subscapularis); articular view underestimates tear size
- Complete bursectomy for crystal-clear visualisation of the full footprint and tear margins
- Mobilisation (the key step): release adhesions, interval slides if needed, margin convergence for U-shaped — must reach the lateral footprint tension-free
- Footprint preparation: gentle decortication to punctate bleeding, preserve bone stock
- Medial row: 2–3 anchors at the articular margin, mattress sutures
- Lateral row: 2–3 knotless anchors 10–15 mm lateral capturing the medial sutures — the suture bridge
Danger zones
- Suprascapular nerve (2 cm medial to glenoid) — shallow blunt medial releases, no thermal devices medially
- Axillary nerve (5 cm inferior to acromion) — all portals greater than 5 cm, no inferior portals
- Articular cartilage — medial row AT the margin, not medial (an intra-articular anchor causes chondrolysis)
- Musculocutaneous nerve (3–8 cm distal to coracoid) — anterior portals superior and lateral to the coracoid
- Deltoid origin — minimal acromioplasty only; over-resection detaches the deltoid (catastrophic)
Technique pearls
- Mobilisation test: tendon must reach the lateral footprint with the arm at the side, tension-free — if not, mobilise more or convert to single-row
- Medial row AT the articular margin at a 45-degree deadman angle
- Lateral row 10–15 mm lateral at the anatomic footprint edge
- Balanced tension: medial approximates without blanching, lateral compresses without being drum-tight
- Dynamic ROM test: the completed repair must not gap with passive motion
- Acromioplasty: no proven outcome benefit — minimal or none unless a Type III hook
Complications
- Re-tear 10–20 percent overall, 20–30 percent for large tears (age greater than 65, smoking, diabetes, Goutallier 3–4, inadequate mobilisation, over-tension)
- Stiffness 8–15 percent — higher than single-row; early passive ROM
- Anchor problems 3–5 percent — pull-out, prominence, intra-articular
- Suprascapular nerve injury 0.5–2 percent — from aggressive medial releases
- Medial-row failure with lateral row intact — over-tensioned lateral row; revise intra-operatively
Post-op protocol
- Phase 1 (0–6 weeks): abduction brace 30–45 degrees 24/7; passive ROM only (FF to 90–120 degrees, ER to 30 degrees); no active or resisted motion
- Phase 2 (6–12 weeks): wean brace to sling; active-assisted to full active ROM; light isometrics week 10–12
- Phase 3 (12–20 weeks): progressive resistance, scapular stabilisation, proprioception
- Phase 4 (20+ weeks): full strengthening; desk work 2–3 weeks, light duty 3 months, manual labour 5–6 months, overhead sports 6–9 months
- Immobilisation compliance is critical for biological healing
Exam tips
- Double-row is superior for LARGE tears greater than 3 cm only (lower re-tear); not for small-medium tears; clinical outcomes are similar regardless
- Mobilisation quality matters more than fixation construct — inadequate mobilisation guarantees failure
- Biomechanically superior (60–80 percent contact, 3–5 times pressure, 20–40 percent stronger) but clinically equivalent — know this discrepancy
- Individualise: young active patients with large tears benefit most; elderly low-demand may not need the complexity
- Bail out: if tissue is inadequate after full mobilisation, convert to a medialiszed single-row — tension-free adequate beats over-tensioned maximal
Background & Evidence
Epidemiology. Rotator cuff disease is one of the most common causes of shoulder pain and disability, and the prevalence of full-thickness tears rises steeply with age. Most are degenerative and many are bilateral; only a minority come to surgical repair, typically when pain, weakness and loss of function fail an adequate trial of non-operative management (activity modification, physiotherapy, NSAIDs and, selectively, a subacromial injection). Pathoanatomy. The posterosuperior cuff inserts across the greater tuberosity. The supraspinatus footprint lies on the superior facet (about 15 mm AP x 25 mm SI) with its medial border at the articular margin, extending 15–18 mm laterally; the infraspinatus occupies the posterior facet (about 20 mm AP x 25 mm SI); the subscapularis inserts on the lesser tuberosity (about 20 mm ML x 25 mm SI). A double-row suture-bridge construct aims to recreate this native enthesis — medial fixation at the articular margin and lateral compression across the full footprint. Chronic tears retract, scar down, and undergo fatty infiltration (Goutallier), which is the dominant determinant of healability and frequently overrides any construct advantage.
- Definition
- Less than 1 cm in any dimension
- Surgical relevance
- Single-row adequate
- Definition
- 1–3 cm in largest dimension
- Surgical relevance
- Single-row or double-row
- Definition
- 3–5 cm in largest dimension
- Surgical relevance
- Double-row favoured for structural healing
- Definition
- Greater than 5 cm, or two or more tendons
- Surgical relevance
- Often irreparable; consider SCR, partial repair or reverse arthroplasty
- Tendon position
- Tendon edge near the greater tuberosity
- Surgical relevance
- Excellent prognosis; direct repair
- Tendon position
- Retracted to the level of the humeral head apex
- Surgical relevance
- Mobilisation required
- Tendon position
- Retracted to the level of the glenoid
- Surgical relevance
- Often irreparable; consider SCR
- Fatty infiltration
- Normal muscle, no fat
- Prognosis
- Good healing potential
- Fatty infiltration
- Some fatty streaks
- Prognosis
- Good
- Fatty infiltration
- Less fat than muscle
- Prognosis
- Acceptable
- Fatty infiltration
- Equal fat and muscle
- Prognosis
- Poor healing; relative contraindication
- Fatty infiltration
- More fat than muscle (greater than 50 percent)
- Prognosis
- Poor; high failure regardless of technique
Tear patterns drive the repair strategy:
- Crescent — straight, mobile tear edge; direct repair.
- U-shaped — retracted leaves; margin convergence first to convert to a crescent, then repair.
- L-shaped — apex extends anteriorly or posteriorly; repair the apex (corner stitch) first, then the margins.
- Massive / irreparable — greater than 5 cm with Patte Stage 3 and Goutallier Grade 3–4; consider SCR, partial repair or reverse arthroplasty. Key evidence. Multiple Level 1 RCTs and meta-analyses compare double-row with single-row. For small-medium tears (less than 3 cm) there is no significant difference in pain, function, ROM, satisfaction or re-tear. For large tears (greater than 3 cm) double-row lowers imaging re-tear rates — pooled data (Millett, 7 RCTs) report 25.9 percent single-row versus 14.2 percent double-row (relative risk 1.76) — yet patient-reported outcomes remain similar between groups. The highest-quality concordant meta-analyses (Mascarenhas) confirm superior structural healing, most evident for tears greater than 3 cm. The consistent message — structural superiority without proven clinical superiority, with the largest benefit in big tears — is the perennial exam point. Detail is carried in the EvidenceCards below.
References
Footprint contact characteristics for a transosseous-equivalent (suture bridge) repair compared with a double-row technique
- Cadaveric biomechanical study (6 fresh-frozen shoulders) using pressure-sensitive film at the tendon-footprint interface
- Four-suture-bridge transosseous-equivalent repair restored 77.6 percent of the footprint (124.2 mm2) versus 39.6 percent (63.3 mm2) for a conventional double-row repair
- Mean tendon-bone interface pressure was higher with the suture bridge construct (0.27 MPa) than the double-row construct (0.19 MPa)
Clinical and structural outcomes after arthroscopic single-row versus double-row rotator cuff repair: meta-analysis of Level I RCTs
- Meta-analysis of 7 Level 1 RCTs (524 shoulders)
- Imaging-confirmed re-tear rate 25.9 percent (single-row) versus 14.2 percent (double-row); relative risk 1.76 (95 percent CI 1.25–2.48) favouring double-row, driven mainly by partial-thickness re-tears
- No significant difference between groups in ASES, UCLA or Constant scores
Is double-row rotator cuff repair clinically superior to single-row? A systematic review of overlapping meta-analyses
- Systematic review of 8 meta-analyses, quality-appraised with Oxman-Guyatt, QUOROM and the Jadad decision algorithm
- 6 of 8 meta-analyses found no patient-outcome difference; 2 favoured double-row for tears greater than 3 cm
- The 3 highest-quality concordant meta-analyses all found significantly better structural healing with double-row repair
Prospective randomised trial comparing arthroscopic single- and double-row repair: MRI and early clinical evaluation
- RCT of 40 patients (mean tear 1.8 cm) with serial MRI to 1 year
- Two re-tears in each group; no significant difference in MRI footprint coverage, tendon thickness or tendon signal
- No difference in WORC, Constant, ASES, UCLA or SANE scores at 1 year
Single-row versus double-row arthroscopic rotator cuff repair: a prospective randomised clinical study
- RCT of 80 patients with full-thickness tears, 2-year follow-up
- No significant difference in DASH, Work-DASH, Constant score or muscle strength between single-row and double-row
- Multivariate analysis showed age, gender and baseline strength — not fixation construct — independently influenced outcome
Further reading & classification sources 1. Ma HL, Chiang ER, Wu HT, et al. Clinical outcome and imaging of arthroscopic single-row and double-row rotator cuff repair: a prospective randomised trial. Arthroscopy. 2012;28(1):16-24. doi:10.1016/j.arthro.2011.07.003 2. Bedeir YH, Jimenez AE, Grawe BM. Outcomes of arthroscopic rotator cuff repair with and without acromioplasty: a systematic review. J Shoulder Elbow Surg. 2022;31(4):e171-e181. doi:10.1016/j.jse.2021.10.025 3. Goutallier D, Postel JM, Bernageau J, Lavau L, Voisin MC. Fatty muscle degeneration in cuff ruptures: pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res. 1994;(304):78-83. 4. Patte D. Classification of rotator cuff lesions. Clin Orthop Relat Res. 1990;(254):81-86. 5. Cofield RH. Subscapular muscle transposition for repair of chronic rotator cuff tears. Surg Gynecol Obstet. 1982;154(5):667-672.