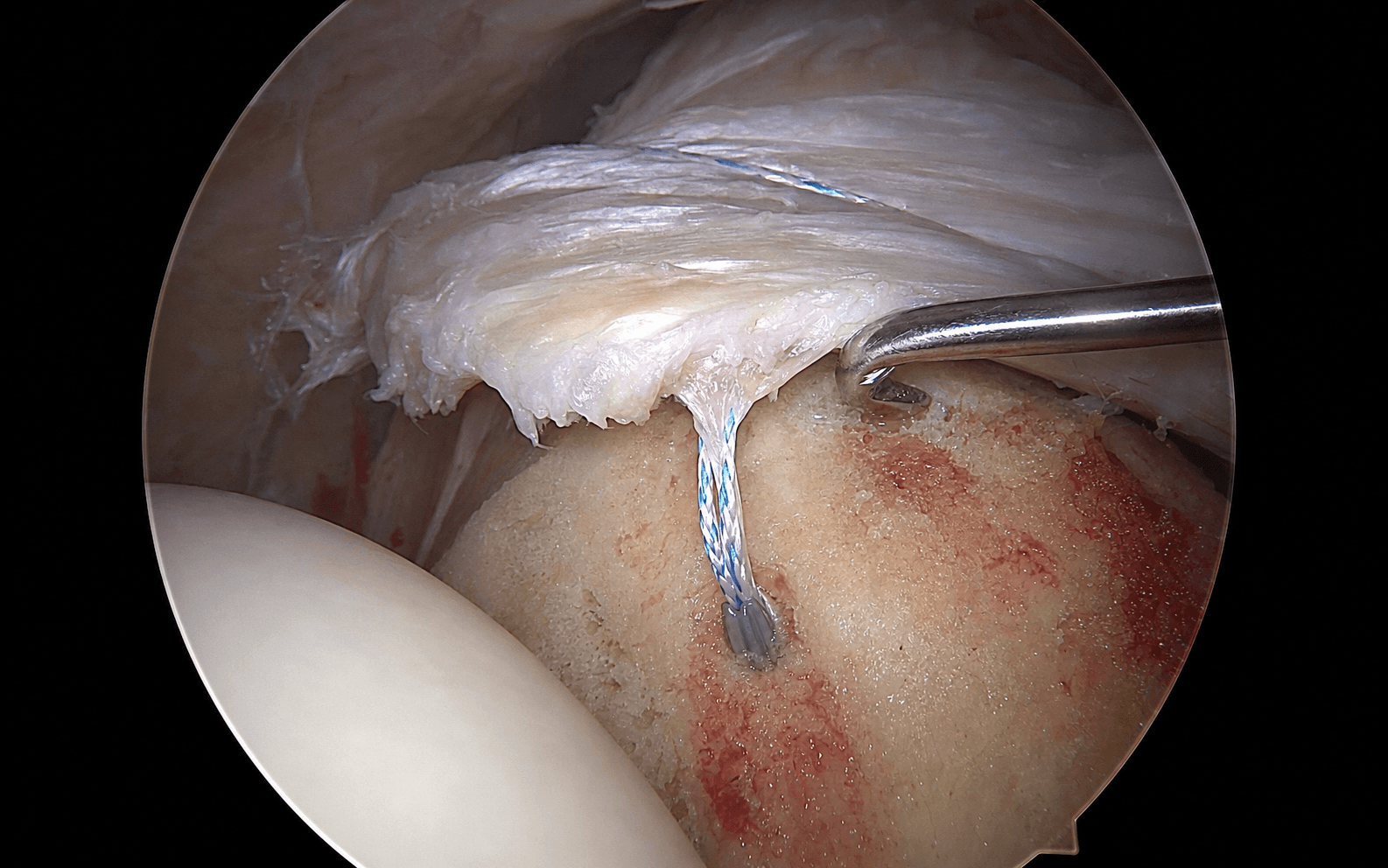
Arthroscopic repair through a posterior viewing portal, lateral working portal and anterior-superior accessory portal. The subacromial space is the working area; single-row suture anchors are placed at the lateral footprint edge at the 45 degree deadman angle.
- Single-row repair: anchors placed at the lateral footprint edge near the articular margin at a 45 degree deadman angle for optimal pull-out strength.
- Complete bursectomy is the foundation of success - poor visualization guarantees a suboptimal repair. You must see the acromion, the coracoacromial ligament, the entire tear, and the footprint.
- Tear pattern determines strategy: crescent (direct repair), U-shaped (margin convergence first), L-shaped (apex first), massive (partial repair / SCR / reverse TSA).
- Adequate mobilization without tension is critical: release all adhesions, use interval slides if needed. The tendon must reach the footprint with the arm at the side.
- “Single-row versus double-row: double-row is biomechanically superior (greater footprint coverage 60-80 percent versus 30-50 percent, higher ultimate load) BUT multiple meta-analyses show NO clinical difference in outcomes for small-medium tears. Reserve double-row for large tears or revision.
- “Reparability assessment: Patte Stage 3 retraction (to the glenoid) plus Goutallier Grade 3-4 fatty infiltration is often irreparable. Intraoperatively, after mobilization the tendon must reach the lateral footprint with the arm at the side without excessive tension.
- “Over-tensioning the repair is the number one technical error causing failure - it creates ischemia, necrosis and suture cut-through. The goal is gentle approximation, not a drum-tight repair. Biology provides the strength, not knot tension.
- “Post-op protocol dictates outcomes: Phase 1 (0-6 weeks) passive only in an abduction sling protects the repair. Early active motion causes re-tear. Large tears need 8 weeks of protection versus 6 weeks for small tears.
When & Why
Indications. A symptomatic full-thickness rotator cuff tear that has failed three to six months of conservative care (physiotherapy, NSAIDs, and at least one subacromial corticosteroid injection) — most commonly a small to medium tear less than 3 cm with good-quality tissue (Goutallier Grade 0-2) and minimal retraction (Patte Stage 1-2). Other indications are acute traumatic tears in active patients under 65 years, and partial tears greater than 50 percent thickness that have been completed and repaired. Contraindications. An irreparable tear (Patte Stage 3 retraction to the glenoid plus Goutallier Grade 3-4 fatty infiltration, or a tendon that will not mobilize to the footprint), active infection, and medical comorbidities that prohibit surgery. Massive tears in elderly low-demand patients with pseudoparalysis are increasingly managed with a primary reverse total shoulder arthroplasty rather than a repair likely to fail. Consent specifically for a re-tear rate of 15-30 percent overall (rising with tear size), stiffness or adhesive capsulitis (5-10 percent), infection (0.5-1 percent), axillary or suprascapular nerve injury (0.5-1 percent each), anchor-related problems (2-5 percent), persistent pain despite an intact repair (10-15 percent), and the possible need for revision surgery or conversion to a superior capsular reconstruction or reverse TSA. The one decision that matters. Everything begins with the same operation - complete bursectomy, mobilization, footprint preparation, and anchor fixation. The single real choice is the construct, and the evidence drives it:
Anchors at the lateral footprint edge. Level I evidence shows functional outcomes equivalent to double-row for small-medium tears, with shorter operative time, lower cost, and less technical complexity.
A medial plus lateral row, or bridging sutures. Better structural healing and footprint coverage; reserve for large tears greater than 3 cm, revision repairs, or high-demand patients where the marginal biomechanical benefit is justified.
When the tendon will not reach the footprint without tension, abandon the repair: partial repair, superior capsular reconstruction (SCR), tendon transfer, or - in the elderly pseudoparalyzed patient - reverse TSA.
Positioning. Beach chair (preferred): head elevated 60-70 degrees, arm in a pneumatic holder with 10-15 lbs of traction, 20-30 degrees of abduction and neutral rotation. Advantages: better arm mobility for dynamic repair assessment, easy conversion to mini-open, more physiologic and easier for anesthesia. Risks: hypotensive cerebral hypoperfusion and fluid extravasation tracking to the neck. Lateral decubitus (alternative): affected side up, 45 degrees of abduction in skin or skeletal traction, 20 degrees of forward flexion, 10-15 lbs of traction. Advantages: better superior visualization and a stable field with less extravasation. Disadvantages: difficult conversion to open and traction neuropraxia risk. Portals (three, each 5-8 mm). Posterior viewing portal in the soft spot 2 cm inferior and 1 cm medial to the posterolateral acromion corner, between infraspinatus and teres minor. Lateral working portal 2-3 cm lateral to the lateral acromion edge, in line with the posterior clavicle (the scapular plane) — this is the KEY portal whose position sets the perpendicular trajectory for the 45 degree deadman anchor angle; keep it clear of the axillary nerve (danger if more than 5 cm inferior to the acromion). Anterior-superior accessory portal through the rotator interval, established inside-out with a spinal needle for suture management. Equipment. A 30 degree arthroscope (70 degree optional for the medial cuff edge); fluid pump at 50-60 mmHg; 4.0 mm aggressive and 5.5 mm full-radius shavers, a radiofrequency wand, burr and probe; penetrating suture passers; 2-4 double-loaded suture anchors (4.5 mm for good bone, 5.5 mm for poor bone); 8 mm threaded clear cannulas. Inject the glenohumeral joint with 30-50 ml of saline with epinephrine 1:300,000 for distension and hemostasis.
The Operation
The goal is to restore the torn cuff to its anatomic footprint under minimal tension using a single row of suture anchors at the lateral footprint edge. Everything depends on visualization: a complete bursectomy, accurate portals, and a tension-free repair that survives dynamic range-of-motion testing. The exposure — positioning, portal placement and bursectomy — is laid out as the first steps because it is the foundation of the whole case.
Operative sequence
- Beach chair at 60-70 degrees, pneumatic holder with 10-15 lbs traction (just enough to distract the joint - excessive traction causes neuropraxia), 20-30 degrees of abduction, neutral rotation.
- Avoid head tilt or lateral neck flexion to prevent brachial plexus traction; prep and drape the shoulder, neck and arm to mid-forearm.
- Mark the acromion (all edges and corners), clavicle, coracoid and AC joint, then the portal sites; inject the joint with 30-50 ml saline and epinephrine 1:300,000 for hemostasis.
- Establish the posterior portal at the soft spot (2 cm inferior, 1 cm medial to the posterolateral acromion corner); direct the blunt trocar toward the coracoid tip to enter the joint.
- Perform a systematic glenohumeral examination: biceps origin and intra-articular course, subscapularis (look for the comma sign of a complete tear), labrum (SLAP, Bankart), glenohumeral ligaments, humeral head and glenoid cartilage, posterior labrum and capsule, and the articular surface of the cuff.
- The crescent sign (exposed greater tuberosity visible through the tear) confirms a full-thickness tear. Concomitant pathology occurs in 40-50 percent and changes the plan: a biceps tear greater than 50 percent, subluxation or pulley lesion needs tenotomy or tenodesis; a comma sign needs subscapularis repair. The articular view underestimates tear size — the bursal side shows the true extent.
- Create the lateral portal 2-3 cm lateral to the lateral acromion edge in line with the posterior clavicle (scapular plane), using an outside-in spinal needle to confirm trajectory under direct vision.
- This is the KEY working portal: its position sets a perpendicular trajectory to the greater tuberosity, allowing anchor placement at the 45 degree deadman angle. Too anterior and the posterior cuff is inaccessible; too posterior and the anterior cuff is inaccessible; too inferior (more than 5 cm below the acromion) and the axillary nerve is at risk.
- Switch the camera to the lateral portal to view the subacromial space and work through the posterior portal to begin the bursectomy.
- The subacromial bursa is the largest bursa in the body and in chronic tears is thickened, inflamed and highly vascular. Perform a COMPLETE bursectomy with a shaver and radiofrequency device, working anterior-to-posterior and medial-to-lateral.
- At the end you must see clearly: the entire undersurface of the acromion, the coracoacromial ligament medially, the entire cuff tear from the bursal side (often much larger than it appeared articular-sided), and the greater tuberosity footprint.
- This step takes 15-20 minutes and cannot be rushed — poor visualization from incomplete bursectomy is the most common cause of a suboptimal repair. Use radiofrequency liberally for hemostasis; any bleeding obscures the field.
- Assess acromion morphology (Bigliani Type I flat, II curved, III hooked) and any anteroinferior traction spur.
- The role of acromioplasty is controversial: modern RCTs and meta-analyses show it does NOT improve outcomes in most repairs, because cuff tears reflect intrinsic tendon degeneration rather than extrinsic impingement. Routine coracoacromial ligament release can risk anterosuperior escape.
- Reserve minimal acromioplasty for a significant Type III hook or a large anteroinferior spur causing mechanical block; remove 3-5 mm anteroinferiorly to a flat surface, preserving the CA ligament medially.
- Assess five parameters: size (Cofield - small less than 1 cm, medium 1-3 cm, large 3-5 cm, massive greater than 5 cm); pattern (crescent, U-shaped, L-shaped, massive contracted); tissue quality; retraction (Patte Stage 1-3); and fatty infiltration (Goutallier Grade 0-4 on pre-op MRI).
- Mobilize by releasing adhesions on the superior (to acromion), lateral and bursal surfaces, and carefully on the medial border (the suprascapular nerve runs 2-3 cm medial to the glenoid rim). Use interval slides (anterior between supraspinatus and subscapularis, posterior between supraspinatus and infraspinatus) for retracted tears.
- The test of adequacy: the tendon must reach the lateral footprint with the arm at the side WITHOUT excessive tension. Inadequate mobilization leaving the repair under tension is the number one preventable cause of failure.
- Clear soft tissue, scar and granulation tissue with a shaver and radiofrequency to expose cortical bone, then lightly decorticate to punctate bleeding bone for biological healing.
- The supraspinatus footprint is 15 mm AP by 25 mm SI on the anterior facet; the infraspinatus footprint is 20 mm AP by 25 mm SI on the middle and posterior facets.
- Do NOT create a deep bony trough: over-aggressive decortication greater than 5 mm deep weakens the bone and reduces anchor pull-out strength by 40-60 percent. Aim for a roughened vascular surface 3-5 mm wide at the lateral edge.
- Place anchors at the LATERAL EDGE of the prepared footprint near the articular margin-lateral junction - this restores the footprint, maximizes tendon-bone contact and preserves bone stock.
- Use 1-2 anchors for small tears, 2-3 for medium (spaced 5-8 mm apart), 3-4 for large; double-loaded anchors give four suture limbs each. Choose 4.5 mm anchors for good bone and 5.5 mm for poor bone.
- Insert each anchor at the 45 degree DEADMAN ANGLE to the cortical surface via the lateral portal. This engages cortical bone at the surface and cancellous bone deep, giving 40-50 percent greater pull-out resistance than perpendicular or shallow oblique angles. Test each anchor with a gentle pull before proceeding.
- Immediately after each anchor is placed, retrieve and organize its suture limbs before placing the next anchor — tangled sutures can add 20-30 minutes.
- Color-code by anchor (for example blue equals anterior, white equals posterior) and pass different colors through different cannulas to keep them physically separated.
- Test each limb individually; it should slide freely without catching another suture.
- Pass sutures with a penetrating device (Spectrum, Scorpion, BirdBeak). MATTRESS sutures are preferred over simple sutures: they capture more tendon (5-10 mm width), distribute force and resist cut-through in degenerative tissue.
- Place each pass 5-10 mm from the tear edge (closer and the suture cuts through; further and the tendon bunches), with an adequate tissue bite of at least 5-8 mm of healthy tendon.
- Avoid friable degenerative zones; choose thicker tissue. For a two-anchor mattress repair this is four passes total.
- Tie systematically from anterior to posterior (consistency matters) using a sliding-locking knot (SMC or Revo); tighten the post limb first to slide the knot to tissue, then lock with a minimum of three alternating half-hitches.
- The CRITICAL concept is APPROPRIATE TENSION. Over-tightening is the number one technical error: it blanches the tendon (ischemia), causes necrosis and suture cut-through. The goal is gentle approximation — the biology provides the long-term strength, not knot tension.
- The tendon should touch bone with no gap but keep a healthy pink color; cut tails to 2-3 mm and bury any prominent knot.
- Visually confirm tendon-to-footprint coverage from multiple portals with no gap greater than 2 mm and no medial bunching; probe gently — the repair should not gap.
- Dynamic testing is the most important check: remove the arm from traction and take it through passive forward flexion to 120 degrees, abduction to 90 degrees and rotation, watching the repair throughout.
- If the repair gaps with normal passive motion it is UNDER EXCESSIVE TENSION and will fail. Options: re-tie looser accepting a 1-2 mm gap (biology will heal it), accept a medialized footprint (healing 5-10 mm medial may actually lower re-tear rates), or convert to a partial repair.
- U-shaped tears have retracted medial and lateral leaves separated by a gap. Direct repair to the footprint without convergence places the repair under massive tension and fails in over 60 percent.
- Pass side-to-side horizontal mattress sutures across the gap, 2-4 sutures spaced 1 cm apart; tie these FIRST to approximate the leaves and convert the U into a crescent, then proceed with standard footprint repair.
- This reduces peak strain at the footprint by 30-40 percent and improves healing for U-shaped tears from 50-60 percent to 75-85 percent. Do not over-tighten — the goal is approximation, not strangulation.
- Achieve hemostasis with radiofrequency or an epinephrine-soaked pattie; small ooze is acceptable but brisk bleeding risks a hematoma (which multiplies infection risk).
- Inspect both compartments: glenohumeral (no loose suture fragments or chondral damage, biceps and subscapularis intact) and subacromial (repair secure, no prominent knot, no residual bursal debris).
- Irrigate copiously with 3-6 L of saline; infiltrate the subacromial space and portals with 0.25 percent bupivacaine for post-op analgesia. Avoid intra-articular corticosteroid, which may impair healing.
- Remove all instruments under direct vision. Close the posterior and lateral portals with 3-0 nylon and the anterior-superior portal with 4-0 nylon or absorbable monocryl; apply sterile dressings and a compressive wrap.
- Immobilize in an ABDUCTION SLING at 30-45 degrees: abduction relaxes the supraspinatus musculotendinous unit and reduces repair-site strain by about 35 percent compared with the arm at the side. A simple sling is acceptable only for small tears.
- Patient education is critical: the sling stays on 24 hours a day for six weeks except for supervised passive exercises. Non-compliance is a major cause of re-tear (around three times higher risk).
The axillary nerve exits the quadrangular space with the posterior humeral circumflex artery and wraps around the surgical neck 5-7 cm inferior to the acromion — keep the lateral portal clear of the acromion and avoid inferior dissection beyond the inferior capsule. The suprascapular nerve runs through the suprascapular notch and then 2-3 cm medial to the posterior glenoid rim in the spinoglenoid notch — limit medial releases to within 1 cm of the glenoid and keep radiofrequency away from the medial border. Most nerve injuries are neurapraxia from traction and recover in 3-6 months; obtain an EMG at three months if there is no clinical recovery.
The natural instinct is to crank the knots down tight for solid tendon-bone contact — this is wrong and causes failure. Over-tightening blanches the tendon (ischemia), causes necrosis and suture cut-through. Aim for gentle approximation: tendon touching bone with no gap but a healthy pink color. Accepting a 1-2 mm gap is better than over-tensioning, because biology fills a small gap but cannot recover from ischemia.
Insert each anchor at 45 degrees to the cortical surface. This angle engages the strong cortical bone at the surface and the cancellous bone deep, giving 40-50 percent greater pull-out resistance than a perpendicular or a shallow oblique angle. The lateral working portal is positioned precisely to deliver this trajectory.
Critical danger structures
Wraps the surgical neck 5-7 cm inferior to the acromion with the posterior humeral circumflex artery. Protect: keep the lateral portal greater than 5 cm clear of the acromion; avoid inferior dissection beyond the inferior capsule.
Passes under the superior transverse scapular ligament, then runs 2-3 cm medial to the posterior glenoid rim in the spinoglenoid notch, supplying supraspinatus then infraspinatus. Protect: limit medial releases to within 1 cm of the glenoid; keep radiofrequency off the medial border.
Enters coracobrachialis 3-8 cm distal to the coracoid tip (variable, as proximal as 2 cm in 20 percent). Protect: limit anterior dissection beyond the conjoint tendon; avoid anterior-inferior capsular release.
Runs in the deltopectoral groove. Protect: identify and retract (laterally with deltoid or medially with pectoralis) if a mini-open approach is used; injury causes hematoma and a cosmetic defect.
Originates from the supraglenoid tubercle and superior labrum, exits through the rotator interval between supraspinatus and subscapularis. Protect: assess at glenohumeral arthroscopy; if pathologic (greater than 50 percent tear or subluxation) perform tenotomy or tenodesis to prevent persistent anterior pain.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|-----------------|---------| | 1 - Protection | 0-6 weeks | Abduction sling 30 degrees, 24 hours/day | Pendulums from day 1; passive forward flexion to 90 degrees by week 4 then 120 degrees by week 6; passive external rotation to 30 degrees. No active motion, no weight bearing | | 2 - Active motion | 6-12 weeks | Wean sling weeks 6-8, off by week 8 | Active-assisted ROM (pulley, cane, wall walks); full active ROM by week 8-10; light isometrics from week 10-12 | | 3 - Strengthening | 12-16 weeks | Splint for heavy tasks only | Theraband then 1-2 lb weights advancing to 3-5 lbs; rotator cuff, scapular stabilizers and deltoid; proprioception | | 4 - Return to activity | 16-24 weeks | None | Sport- or work-specific training; return to non-contact sport at 4-6 months, contact sport and heavy overhead labor at 6-9 months; full recovery 6-12 months | Large tears need prolonged protection (passive only 0-8 weeks, active 8-12 weeks); small tears can progress faster (active ROM at 4-6 weeks). Follow up at 2 weeks (wound check), 6 weeks (sling off, start active ROM), 3 months (advance strengthening) and 6 months (return-to-sport clearance). MRI is not routine unless a re-tear is suspected clinically (return of pain or weakness, positive lag signs). An asymptomatic re-tear can be observed; a symptomatic re-tear needs a decision between revision repair (if good tissue and compliance) and SCR or reverse TSA. Expected outcomes by tear size
- Re-tear rate
- 10-15 percent
- Pain relief
- 90-95 percent significant
- Strength recovery
- 85-90 percent normal
- Return to sport
- 4-6 months (90 percent)
- Satisfaction
- 90-95 percent
- Re-tear rate
- 20-25 percent
- Pain relief
- 85-90 percent significant
- Strength recovery
- 70-80 percent normal
- Return to sport
- 6-9 months (75 percent)
- Satisfaction
- 85-90 percent
- Re-tear rate
- 30-40 percent
- Pain relief
- 75-85 percent significant
- Strength recovery
- 60-70 percent normal
- Return to sport
- 9-12 months (60 percent)
- Satisfaction
- 75-85 percent
- Re-tear rate
- 40-60 percent
- Pain relief
- 65-75 percent improvement
- Strength recovery
- 40-60 percent (often weak)
- Return to sport
- 12+ months (40 percent)
- Satisfaction
- 60-75 percent
Key outcome predictors: tear size (the strongest predictor — small 10 percent versus massive 60 percent re-tear); age greater than 65 years (OR 1.8, slower recovery); fatty infiltration (Goutallier 3-4 predicts 60 percent re-tear versus 15 percent for Grade 0-1); smoking (doubles re-tear risk, OR 2.1 — advise cessation 6 weeks pre-op); diabetes (infection 3 percent versus 0.5 percent, slower healing — optimize HbA1c less than 7 percent); and workers compensation (slower return to work, lower satisfaction). Complications
- Recognition
- Return of pain and weakness; positive lag and drop-arm signs; MRI shows a full-thickness defect with fluid and retraction
- Prevention
- Adequate mobilization without tension, six weeks passive-only immobilization, optimize biology (smoking cessation), avoid over-tensioning
- Management
- Small asymptomatic re-tear: observe and physiotherapy. Symptomatic: revision repair if good tissue, or SCR / patch / reverse TSA if massive or elderly
- Recognition
- Loss of passive ROM (forward flexion less than 120 degrees, external rotation less than 30 degrees); global restriction
- Prevention
- Balance six weeks of protection with early gentle passive ROM from week 2-4; avoid immobilization beyond 8 weeks; diabetics need early gentle ROM
- Management
- Aggressive physiotherapy, NSAIDs and intra-articular steroid; manipulation under anaesthesia at 3-4 months once healed, then arthroscopic capsular release if refractory
- Recognition
- Fever, severe pain out of proportion, erythema and effusion within days-weeks; raised WBC/CRP/ESR; aspiration WBC greater than 50,000, S. aureus most common
- Prevention
- Single-dose first-generation cephalosporin at induction (glycopeptide if true beta-lactam allergy), meticulous sterile technique, copious irrigation, optimize diabetes
- Management
- Immediate arthroscopic washout and debridement (retain well-fixed anchors), IV antibiotics by sensitivities, repeat washouts every 2-3 days; chronic infection may need anchor removal and staged reconstruction
- Recognition
- Pull-out: acute pop and return of weakness. Migration: delayed pain and mechanical symptoms. Prominence: pain and clicking
- Prevention
- 45 degree deadman angle, gentle decortication, adequate bone stock, test pull before suture passage, avoid proud insertion
- Management
- Pull-out: revise with a new position/trajectory. Migration into joint: arthroscopic removal and re-assess. Prominent: remove and replace if symptomatic
- Recognition
- Deltoid paralysis and anterior shoulder numbness; weak or absent abduction; EMG at 3-4 weeks confirms denervation
- Prevention
- Keep lateral portal greater than 5 cm from the acromion; avoid inferior dissection; beach chair reduces traction compared with lateral decubitus
- Management
- Most are neurapraxia and recover in 3-6 months; physiotherapy to prevent contracture; EMG at 3 months; consider exploration or nerve transfer (spinal accessory to axillary) if no recovery by 4-6 months
- Recognition
- Posterior shoulder pain, weak external rotation, supraspinatus/infraspinatus atrophy; EMG confirms denervation
- Prevention
- Limit medial releases to within 1 cm of the glenoid; avoid aggressive medial dissection; keep radiofrequency off the medial border
- Management
- Mostly neurapraxia: observe 4-6 months with physiotherapy; EMG at 3 months; MRI at 6 months if no recovery to exclude compression; decompression rarely needed
- Recognition
- Anterolateral pain and weakness, palpable defect; MRI shows deltoid origin disruption
- Prevention
- Arthroscopic technique avoids this; if mini-open, repair the deltoid anatomically with non-absorbable suture; avoid over-aggressive acromioplasty
- Management
- Acute intraoperative recognition: immediate repair to bone. Delayed: conservative if partial, surgical repair if complete with significant weakness; protect six weeks
- Recognition
- Continued pain with an intact repair on MRI, full ROM and good strength
- Prevention
- Address all pathology at the index operation (biceps, AC joint, subscapularis); thorough expectation setting
- Management
- Diagnostic workup (X-rays, MRI, cervical spine, diagnostic AC joint injection) and treat the source (AC resection, biceps tenotomy, adhesiolysis)
Failure analysis. Causes of repair failure are technical errors (40-50 percent: inadequate mobilization, over-tensioning, poor footprint preparation, anchor malposition), biological factors (30-40 percent: poor tissue quality with Goutallier 3-4, age greater than 70, smoking, diabetes), and patient factors (20-30 percent: non-compliance and early active motion). For revision, assess tissue quality: if reasonable and the failure was a correctable technical error, revision repair succeeds in 70-80 percent; if tissue is poor, move to SCR, patch augmentation or reverse TSA. Revision carries a higher re-tear rate (30-40 percent versus 20 percent primary), so consent accordingly and medialize the footprint if lateral bone stock is compromised.
Viva & Exam Focus
PORTALPORTAL placement essentials
REPAIRREPAIR success factors
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What determines whether you use single-row versus double-row repair for a rotator cuff tear?”
“How do you assess whether a rotator cuff tear is reparable or irreparable, and what are your options if irreparable?”
“What is margin convergence, when do you use it, and what is the biomechanical rationale?”
Indications
- Small-medium full-thickness tears less than 3 cm with symptoms failing 3-6 months conservative care
- Acute traumatic tears in active patients under 65
- Partial tears greater than 50 percent thickness (complete and repair)
- Contraindicated: irreparable tear (Patte 3 + Goutallier 3-4), active infection, medical unfitness
Key anatomy
- Supraspinatus footprint: anterior facet, 15 mm AP by 25 mm SI, initiates abduction 0-90 degrees
- Infraspinatus footprint: middle-posterior facets, 20 mm AP by 25 mm SI, external rotation and head depression
- Portals: posterior (soft spot), lateral (2-3 cm lateral, key working portal for perpendicular trajectory), anterior-superior (rotator interval)
- Danger zones: axillary nerve 5-7 cm inferior to acromion; suprascapular nerve 2-3 cm medial to glenoid
Critical steps
- Beach chair 60-70 degrees, 10-15 lbs traction, inject epinephrine 1:300,000 for hemostasis
- Posterior portal with a 21-point glenohumeral exam (biceps, subscapularis/comma sign, labrum, cartilage, cuff)
- Lateral portal 2-3 cm lateral in line with the posterior clavicle - the key working portal
- COMPLETE bursectomy (the foundation) - must see acromion, CA ligament, entire tear, footprint
- Minimal or no acromioplasty (no proven benefit; only for a Type III hook or large spur)
- Mobilize: tendon must reach the lateral footprint with the arm at the side without tension
- Footprint prep: gentle decortication to bleeding bone (avoid a trough greater than 5 mm)
- Anchors at the lateral edge, 45 degree deadman angle, 2-3 double-loaded for a medium tear
- Mattress sutures 5-10 mm from the edge; appropriate tension (gentle, not drum-tight)
- Dynamic ROM test: if it gaps with passive motion it is too tight
- Margin convergence first for U-shaped tears (reduces strain 30-40 percent)
- Copious irrigation (3-6 L), abduction sling at 30 degrees for six weeks
Danger zones
- Axillary nerve: wraps the surgical neck 5-7 cm inferior to the acromion - keep the lateral portal clear, avoid inferior dissection
- Suprascapular nerve: 2-3 cm medial to the glenoid in the spinoglenoid notch - limit medial releases to 1 cm
- Musculocutaneous nerve: enters coracobrachialis 3-8 cm from the coracoid (variable) - limit anterior dissection
- Cephalic vein: deltopectoral groove - identify and retract if mini-open
- Long head of biceps: assess for greater than 50 percent tear or subluxation - tenotomy or tenodesis if abnormal
Technique pearls
- Complete bursectomy is the foundation - poor visualization guarantees a suboptimal repair
- The lateral portal sets the perpendicular trajectory for the 45 degree deadman angle
- Adequate mobilization without tension is the number one technical factor
- Appropriate knot tension - over-tightening is the number one error (ischemia, cut-through)
- Dynamic ROM testing confirms viability - if it gaps, accept a medialized repair or re-tie looser
- Margin convergence is essential for U-shaped tears - direct repair fails in over 60 percent
Complications
- Re-tear 15-30 percent (small 10-15 to massive 40-60); causes: tension, ischemia, poor tissue, non-compliance
- Stiffness 5-10 percent - balance protection with early passive ROM; MUA or capsular release if refractory
- Infection 0.5-1 percent - single-dose cephalosporin at induction; immediate arthroscopic washout and IV antibiotics
- Anchor problems 2-5 percent - 45 degree angle and gentle decortication prevent pull-out
- Axillary nerve injury 0.5-1 percent - mostly neurapraxia recovering in 3-6 months
- Persistent pain despite intact repair 10-15 percent - missed biceps, AC arthritis, subscapularis
Post-op protocol
- Phase 1 (0-6 weeks) protection: abduction sling 24/7, passive ROM only, no active motion
- Phase 2 (6-12 weeks) active motion: wean sling, active-assisted then active ROM, light isometrics
- Phase 3 (12-16 weeks) strengthening: theraband to 3-5 lbs, target 80 percent contralateral strength
- Phase 4 (16-24 weeks) return to activity: sport-specific training, return to sport 4-6 months
- Large tears need longer protection; non-compliance triples re-tear risk
Exam tips
- Know the evidence: Lapner RCT and Level I meta-analyses show no functional difference between single and double-row for small-medium tears
- Reparability: Patte 3 + Goutallier 3-4 often irreparable; intraop the tendon must reach the footprint after mobilization
- Margin convergence for U-shaped tears, side-to-side FIRST, reduces strain 30-40 percent
- Technical errors: inadequate mobilization, over-tensioning, poor footprint prep, anchor angle less than 45 degrees, non-compliance
- Registry trend (NJR, AOANJRR): rising reverse TSA for massive irreparable tears in patients over 70 with pseudoparalysis
- Abduction sling reduces supraspinatus strain about 35 percent; passive-only 0-6 weeks protects the repair
Background & Evidence
Epidemiology. Rotator cuff repair is one of the most rapidly growing orthopaedic procedures. Colvin et al.'s national-trends study documented a 141 percent increase in cuff repairs between 1996 and 2006, with a decisive shift from open to arthroscopic technique - establishing arthroscopic repair as the standard of care. Pathoanatomy and etiology. Modern understanding is that most degenerative cuff tears reflect INTRINSIC tendon degeneration (age-related, vascular and genetic), not extrinsic mechanical impingement from acromial morphology. This is the basis for the move away from routine acromioplasty. The cable-crescent concept explains tear behaviour: a thick load-bearing cable runs from biceps to infraspinatus, and the thin crescent anterior to it is where tears initiate; anterior crescent tears are common, while posterior cable tears indicate massive damage. Classification of the tear
- Size
- Less than 1 cm
- Typical anchors
- 1-2 anchors
- Re-tear rate
- 10-15 percent
- Clinical notes
- Best prognosis, rapid recovery, single-row adequate, return to sport 4-6 months
- Size
- 1-3 cm
- Typical anchors
- 2-3 anchors
- Re-tear rate
- 20-25 percent
- Clinical notes
- Most common size; single-row and double-row equivalent outcomes; 6-9 month recovery
- Size
- 3-5 cm
- Typical anchors
- 3-4 anchors
- Re-tear rate
- 30-40 percent
- Clinical notes
- Consider double-row or suture-bridge; margin convergence often needed; 9-12 month recovery
- Size
- Greater than 5 cm or 2 or more tendons
- Typical anchors
- 4+ anchors or alternative
- Re-tear rate
- 40-60 percent
- Clinical notes
- Often irreparable; consider partial repair, SCR, patch, or reverse TSA
- Description
- Linear tear parallel to the footprint, minimal retraction
- Repair technique
- Direct repair to the lateral footprint, single or double-row
- Technical considerations
- Simplest repair, minimal mobilization, excellent outcomes
- Description
- Retracted medial and lateral leaves creating a U or V
- Repair technique
- Margin convergence FIRST (side-to-side), then footprint repair
- Technical considerations
- Direct repair without convergence means massive tension and failure; convergence reduces strain 30-40 percent
- Description
- Longitudinal split plus lateral retraction
- Repair technique
- Repair the apex FIRST (corner stitch), then the edges sequentially
- Technical considerations
- The apex is under highest stress and must be secured first; common in anterosuperior tears
- Description
- Greater than 5 cm, retracted to the glenoid, poor excursion
- Repair technique
- Partial repair to maximal medialization, OR SCR / patch / reverse TSA
- Technical considerations
- Complete anatomic repair often impossible; partial repair improves pain even if not healed
- Retraction level
- Tendon edge near the anatomic insertion
- Reparability
- Excellent - usually reparable
- Surgical implications
- Minimal mobilization, direct repair, excellent prognosis
- Retraction level
- Retracted to the apex of the humeral head
- Reparability
- Good - usually reparable with mobilization
- Surgical implications
- Complete mobilization, interval slides, may need margin convergence
- Retraction level
- Retracted to the glenoid rim
- Reparability
- Poor - often irreparable despite maximal mobilization
- Surgical implications
- Consider partial repair, SCR, patch, or reverse TSA; the Goutallier grade is critical
- MRI appearance
- Normal muscle, no fat
- Fat-to-muscle ratio
- Normal
- Re-tear risk
- Baseline 10-15 percent
- Clinical impact
- Excellent healing potential, normal strength recovery
- MRI appearance
- A few fatty streaks
- Fat-to-muscle ratio
- Less than 10 percent fat
- Re-tear risk
- Mild increase 15-20 percent
- Clinical impact
- Good healing, near-normal outcomes
- MRI appearance
- Moderate infiltration, more muscle than fat
- Fat-to-muscle ratio
- 10-50 percent fat
- Re-tear risk
- Moderate increase 25-35 percent
- Clinical impact
- Fair healing, incomplete strength recovery; consider double-row
- MRI appearance
- Advanced infiltration, equal muscle and fat
- Fat-to-muscle ratio
- About 50 percent fat
- Re-tear risk
- High 40-50 percent
- Clinical impact
- Poor healing, strength recovery unlikely; consider alternative procedures
- MRI appearance
- Severe infiltration, more fat than muscle
- Fat-to-muscle ratio
- Greater than 50 percent fat
- Re-tear risk
- Very high 50-60 percent
- Clinical impact
- Very poor prognosis; repair may fail; strongly consider SCR or reverse TSA
Surgical anatomy. The subacromial space is bounded superiorly by the undersurface of the acromion, the CA ligament and the AC joint, inferiorly by the superior cuff, medially by the coracoid base and the medial CA attachment, and laterally by the deltoid insertion and lateral humeral cortex; it contains the large vascular subacromial bursa, the supraspinatus (anterior) and infraspinatus (posterior) tendons, the long head of biceps traversing the rotator interval, and the coracoacromial arch (which prevents superior humeral head migration and should be preserved). Acromion morphology (Bigliani): Type I flat (10-15 percent, lowest impingement risk), Type II curved (40-50 percent), Type III hooked (30-40 percent, highest risk) - Type III is associated with cuff tears, but acromioplasty does not improve repair outcomes. Construct biomechanics: single-row versus double-row
- Single-row
- 30-50 percent
- Double-row
- 60-80 percent
- Evidence-based recommendation
- Double-row is biomechanically superior, but with no proven clinical difference
- Single-row
- Lower (250-350 N typical)
- Double-row
- Higher (400-500 N typical)
- Evidence-based recommendation
- Double-row is 20-30 percent stronger in biomechanical studies, not translated to clinical outcomes
- Single-row
- Point contact, higher stress
- Double-row
- Distributed, lower stress per area
- Evidence-based recommendation
- Double-row advantage in early healing, same re-tear rates long-term
- Single-row
- Small 10-15, medium 20-25, large 30-40 percent
- Double-row
- Small 8-12, medium 15-20, large 25-35 percent
- Evidence-based recommendation
- Meta-analyses: no significant difference for small-medium tears, marginal benefit for large tears
- Single-row
- 60-90 minutes
- Double-row
- 90-120 minutes
- Evidence-based recommendation
- Single-row faster, less complex, fewer anchors and lower cost
- Single-row
- 2-3 anchors
- Double-row
- 4-6 anchors (roughly double)
- Evidence-based recommendation
- Single-row significantly less expensive for a marginal benefit
- Single-row
- Small-medium tears less than 3 cm, good tissue
- Double-row
- Large tears greater than 3 cm, revision, high-demand
- Evidence-based recommendation
- Single-row adequate for most; double-row for large tears or athletes
- Region
- US
- Key statement relevant to cuff repair
- Supports repair for symptomatic full-thickness tears failing non-operative care; no established superiority of double-row over single-row for routine tears; routine acromioplasty not required
- Region
- UK
- Key statement relevant to cuff repair
- Repair appropriate for acute traumatic and symptomatic degenerate tears with reparable tissue; emphasizes tissue quality (fatty infiltration) and patient factors over rigid age cut-offs
- Region
- Global
- Key statement relevant to cuff repair
- Sustained year-on-year rise in reverse total shoulder arthroplasty for cuff-tear arthropathy and irreparable massive tears, particularly in patients over 70 with pseudoparalysis
- Region
- Global
- Key statement relevant to cuff repair
- Candidates must justify single-row versus double-row from Level I evidence, demonstrate intraoperative reparability assessment, and articulate the irreparable-tear algorithm (partial repair, SCR, tendon transfer, reverse TSA)
References
Single-row vs double-row fixation in arthroscopic cuff repair: 10-year follow-up of a multicentre RCT
- Randomised 90 patients with full-thickness tears to single-row vs double-row; 77 (85 percent) reviewed at a mean 10 years
- Between baseline and 10 years the mean WORC between-group difference was 3.9 points (95 percent CI -7.8 to 15.6) - statistically detectable at 10 years but below the clinically important threshold
- Only 3 patients developed a new full-thickness tear after 2 years (2 double-row, 1 single-row); 1 revision in each group
- Most outcome scores declined between 2 and 10 years in BOTH groups, reflecting natural progression rather than construct choice
Arthroscopic single-row versus double-row rotator cuff repair: meta-analysis of randomized clinical trials
- Pooled five Level I randomized trials; a test of heterogeneity showed no difference across studies
- No significant difference in ASES, Constant, or UCLA functional scores between single-row and double-row repair
- Confirms that the biomechanical superiority of double-row constructs does not translate into superior clinical function
Single-row versus double-row repair of full-thickness rotator cuff tears (healing versus function)
- Meta-analysis of three RCTs and two cohort studies comparing single-row versus double-row repair
- Double-row improved STRUCTURAL tendon healing and external rotation and reduced recurrence rate, at the cost of longer operative time
- No significant difference in Constant, ASES, UCLA, WORC, DASH, strength, satisfaction, or return to work
Outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears
- 18 patients with tears over 2 cm; recurrent defects on ultrasound in 17 of 18 despite arthroscopic repair
- Mean ASES improved from 48.3 to 84.6 at a minimum 12 months despite the high re-tear rate, with all patients regaining elevation above shoulder level
- At a minimum 24 months results deteriorated (mean ASES fell to 79.9), showing structural failure ultimately undermines durability
Fatty muscle degeneration in cuff ruptures: pre- and postoperative evaluation by CT scan (Goutallier classification)
- Introduced the five-stage CT grading of muscular fatty degeneration in 63 patients undergoing cuff repair
- Supraspinatus repair recurred in 25 percent overall; infraspinatus fatty degeneration correlated strongly with impaired active external rotation and poor outcome
- Recommended operating before irreversible muscular fatty change develops
Fatty infiltration and atrophy do not improve after rotator cuff repair and correlate with poor functional outcome
- Prospective MRI study of 38 patients before and 1 year after repair
- Infraspinatus atrophy and fatty infiltration were the only independent predictors of ASES and Constant scores on multivariate analysis
- Fatty infiltration and atrophy did NOT reverse after repair and progressed more when the repair re-tore
Rehabilitation following arthroscopic rotator cuff repair: RCT of immobilization compared with early motion
- 124 patients under 65 with tears under 30 mm randomised to early ROM versus 6-week immobilization (double-row repair)
- The early-motion group had better elevation and external rotation at 3 months, but NO difference in function at later time points
- Overall 92 percent of tears healed with no difference in healing between protocols (p equals 0.46)
Is acromioplasty necessary in the setting of full-thickness rotator cuff tears? A systematic review
- Systematic review of four RCTs (two Level I, two Level II), 354 patients, repair with versus without acromioplasty or subacromial decompression
- No statistically significant difference in clinical outcomes with versus without acromioplasty
- Routine coracoacromial ligament release can risk anterosuperior escape and worsening symptoms
Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears
- 24 shoulders (23 patients, mean 65 years) with irreparable tears reconstructed with a fascia lata graft
- Active elevation improved from 84 degrees to 148 degrees and ASES from 23.5 to 92.9; the acromiohumeral distance increased from 4.6 mm to 8.7 mm
- 83.3 percent had no graft tear or retear at 24-51 months of follow-up
National trends in rotator cuff repair
- Landmark epidemiology study documenting a dramatic increase in cuff repair - a 141 percent rise between 1996 and 2006
- Captured a decisive shift from open to arthroscopic technique over the study period
Which method of rotator cuff repair leads to the highest rate of structural healing? A systematic review
- Systematic review of repair techniques comparing structural healing rates
- Double-row constructs show biomechanical advantages in footprint coverage and contact pressure
- No clinical superiority of double-row over single-row for small-medium tears, supporting single-row as first-line
Footprint contact characteristics for a transosseous-equivalent (suture-bridge) versus double-row rotator cuff repair
- Biomechanical study establishing that the suture-bridge (transosseous-equivalent) provides superior footprint coverage (about 80 percent versus 60 percent double-row versus 40 percent single-row) and contact pressure
The duration of symptoms does not correlate with rotator cuff tear severity or other patient-related features (MOON Shoulder Group)
- Cross-sectional study of patients with atraumatic full-thickness cuff tears
- Symptom duration did NOT correlate with tear size, retraction, or fatty infiltration