Arthroscopic via standard portals: posterior viewing portal, lateral working portal, anterior portal as needed. Focus on subacromial space for decompression.
- Primary indication: subacromial impingement syndrome failing 3-6 months conservative treatment (PT, NSAIDs, corticosteroid injections) with positive Neer/Hawkins signs and Bigliani Type II/III acromion morphology.
- Complete subacromial bursectomy is the MOST CRITICAL step - without thorough bursal debridement, accurate anatomic visualization for safe acromioplasty is impossible.
- Acromioplasty goal: create a flat Type I acromion undersurface by removing the anteroinferior spur; limit bone resection to 5-7mm maximum to preserve the deltoid origin and prevent acromion fracture.
- Coracoacromial (CA) ligament management is controversial: traditional teaching advocates release for decompression, modern evidence supports preservation as the superior humeral head restraint, especially with rotator cuff deficiency.
When & Why
Indication. Symptomatic subacromial (external) impingement syndrome that has failed 3-6 months of structured conservative treatment — activity modification, physiotherapy, NSAIDs and at least one subacromial corticosteroid injection — with positive Neer and Hawkins impingement signs, a painful arc between 60 and 120 degrees of forward flexion, full passive range of motion, and a Bigliani Type II (curved) or Type III (hooked) acromion with an anteroinferior spur on the outlet-view radiograph. The operation is for genuine mechanical impingement in a patient with an intact rotator cuff. Confirm the diagnosis and the pain source before offering surgery. A diagnostic subacromial injection of local anaesthetic (with or without steroid) is the single most useful test — greater than 50 percent temporary relief predicts a subacromial pain generator and a better surgical outcome. Then exclude the mimics that will NOT improve with decompression:
Bigliani Type III hooked acromion with a visible anteroinferior spur, positive impingement signs, full passive ROM, an intact cuff, and a positive subacromial injection test. This is true mechanical pathology.
A flat Type I acromion with impingement-type pain (wrong diagnosis — search for internal impingement, SLAP, cervical radiculopathy), primary cuff pathology without impingement, adhesive capsulitis, calcific tendinitis, or multifactorial pain (cervical referred pain, fibromyalgia).
The evidence caveat you must own in the viva. High-quality placebo-controlled trials (CSAW, FIMPACT) showed arthroscopic subacromial decompression is no better than sham surgery for unselected subacromial pain with an intact cuff. The defensible modern indication is therefore narrow: reserve decompression for true mechanical impingement — a Type III acromion with a spur and positive impingement signs — after genuine failure of an exercise-led pathway, with shared decision-making that cites this evidence. Consent specifically for persistent or recurrent pain (10-20 percent), stiffness or frozen shoulder (5-10 percent), deltoid dysfunction or detachment from over-resection (1-3 percent), acromion fracture (less than 1 percent), iatrogenic cuff injury (1-2 percent) and axillary nerve injury (less than 1 percent). Be honest that pain resolution is gradual over 3-6 months, not immediate. Setup. Two positioning options:
60-70 degrees upright, head in a gel holder, arm in a pneumatic arm positioner. Familiar anatomic orientation, easy conversion to open if an unexpected cuff tear is found, low fluid extravasation, no traction neuropraxia. Watch for hypotension/cerebral hypoperfusion in the upright position.
Beanbag, 10-12 lbs arm traction, 20-30 degrees forward flexion. Excellent posterior portal access, better joint distraction and glenohumeral visualisation, stable blood pressure. Disorienting at first, traction-related neuropraxia risk, harder to convert to open.
I prefer the beach chair position for anatomic orientation and the ability to convert to open if an unexpected cuff tear is found requiring a complex repair. Lateral decubitus gives excellent distraction for assessing glenohumeral pathology, but I use it selectively.
The Operation
The goal is to enter the subacromial space arthroscopically, perform a complete bursectomy to see the anatomy, reshape the anteroinferior acromion to a flat Type I undersurface removing the impinging spur, preserve the deltoid origin throughout, and confirm the cuff glides freely under the new acromial arch. The exposure — positioning, portal placement and entry into the subacromial space — is laid out as the first steps below (and in depth on the shoulder arthroscopy approach page).
Operative sequence
- Beach chair at 60-70 degrees upright (preferred) or lateral decubitus with arm traction; arm in a pneumatic holder allowing free abduction and rotation.
- Mark every bony landmark: the anterior acromion edge (deltoid origin at risk), lateral acromion edge (portal reference), posterior acromion edge, clavicle, the AC joint (medial limit) and the coracoid.
- Mark the planned portals: posterior (soft spot), lateral, and anterior if needed.
- Create the posterior portal at the soft spot, 2cm inferior and 1cm medial to the posterolateral acromion corner, directed toward the coracoid to enter the glenohumeral joint.
- Perform a systematic diagnostic glenohumeral arthroscopy even though this is primarily a subacromial procedure: biceps tendon, superior labrum (SLAP), anterior labrum and capsule, subscapularis (look for partial tears), inferior recess, posterior structures, and the articular surface of the rotator cuff.
- This step identifies pathology that changes the plan — an articular-sided cuff tear greater than 50 percent that needs repair, biceps pathology, labral tears, arthritis — and is documented systematically.
- Create the lateral portal under direct arthroscopic visualisation, positioned 2-3cm distal to the lateral acromion edge, in line with the posterior border of the clavicle. Use an outside-in spinal needle to confirm the trajectory before committing.
- This is the primary working portal for bursectomy and acromioplasty because it gives the optimal angle on the anteroinferior acromion.
- Critical safety: the axillary nerve lies 5-7cm distal to the lateral acromion — the portal must stay within 2-3cm of the acromion, never beyond 5cm.
- From the posterior portal, redirect the scope superiorly and posteriorly and feel a distinct "pop" as it enters the subacromial space — the potential space between the acromion above and the rotator cuff below, filled with the subacromial-subdeltoid bursa.
- The space can also be entered directly through the lateral portal. In chronically inflamed cases adhesions may require gentle blunt dissection; forceful advancement risks cuff injury.
- Perform a COMPLETE bursectomy with a shaver and/or radiofrequency device, starting laterally and working medially to the AC joint and anteriorly to the CA ligament, removing all hypertrophic inflamed bursal tissue.
- Without thorough bursectomy the anatomy cannot be seen and safe acromioplasty is impossible; the hypertrophic bursa is itself often the dominant pain generator.
- Maintain meticulous haemostasis. Once cleared, identify the acromion undersurface, the CA ligament anteriorly, the bursal surface of the cuff, the greater tuberosity and the AC joint medially.
- Shaver safety: use oscillating mode with suction oriented away from the cuff to avoid iatrogenic cuff injury.
- Systematically assess the acromion undersurface (flat Type I, curved Type II, or hooked Type III), look for the anteroinferior acromial spur (often the main impinging structure), inspect the CA ligament insertion, the AC joint medially, and the cuff from its bursal surface.
- Decide the extent of decompression needed from this assessment. Stop short of unnecessary decompression in a Type I acromion where impingement is not the mechanical cause.
- CA ligament management is controversial. Three options: preserve the ligament (modern trend — it is a superior humeral head restraint, especially with cuff deficiency), release it (traditional — improves decompression), or debride only the thickened or calcified portion.
- If releasing: detach from the anteroinferior acromion with electrocautery/radiofrequency, lateral to medial, preserving the deltoid attachment above.
- With a massive irreparable cuff tear, definitely preserve the CA ligament — releasing it risks anterosuperior humeral escape.
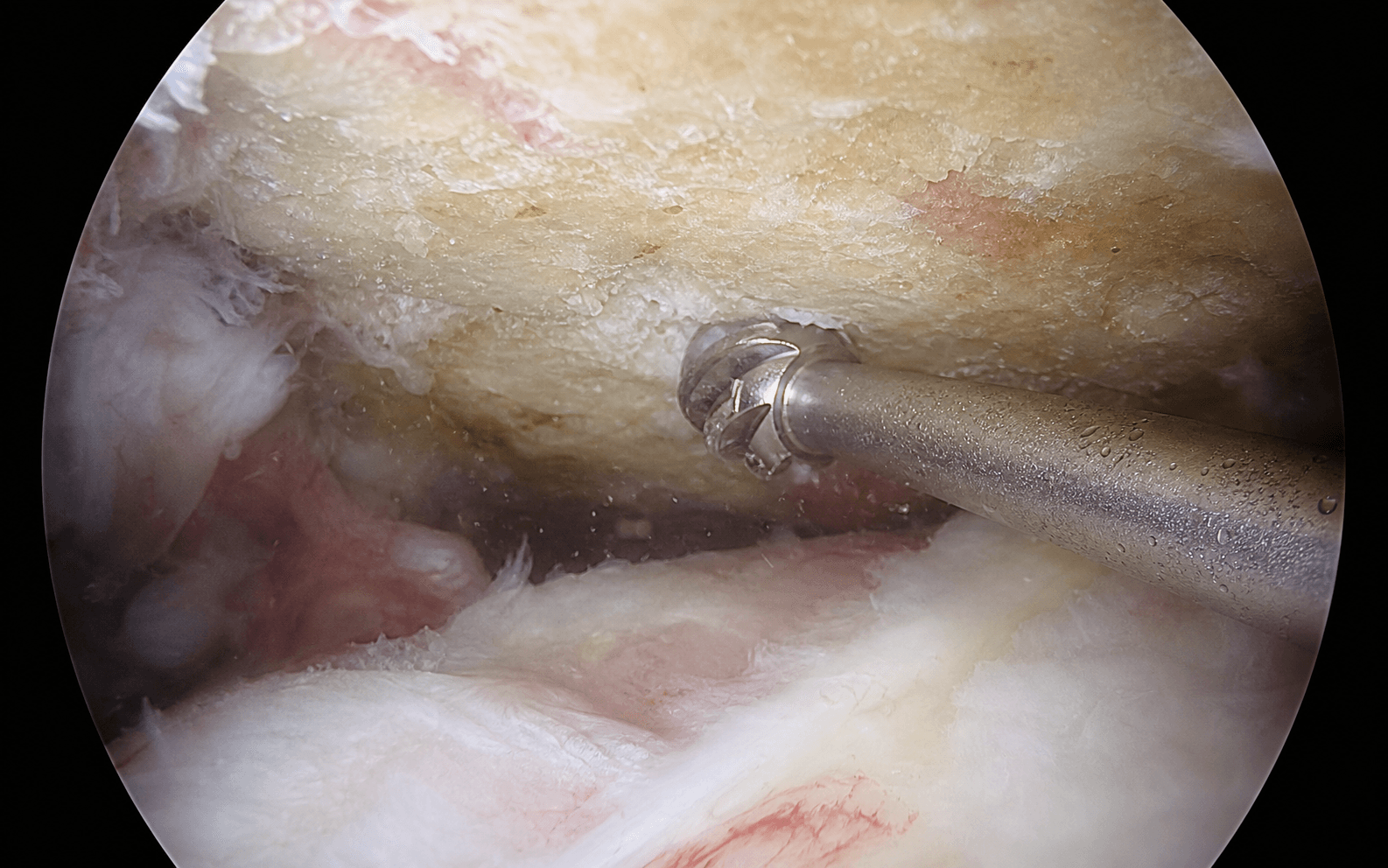
- Use a motorised burr (typically a 5.0-5.5mm round or oval burr) to reshape the acromion. Start at the anteroinferior corner — the primary impingement site — and work from lateral to medial.
- Goal: a flat Type I undersurface, removing the anteroinferior spur and any hooked portion.
- Stay directly on bone (the deltoid origin is on the superior surface you must protect). Limit resection to 5-7mm maximum — over-resection causes deltoid dysfunction and acromion fracture.
- Burr orientation: cutting surface toward the acromion (superiorly), never toward the cuff below.
- Continue systematically anterior-to-posterior and lateral-to-medial, creating a smooth continuous flat undersurface with no sharp edges. Remove all osteophytes.
- Test with a probe — the surface should glide smoothly without catching. Common residual areas are the anteroinferior corner, the lateral edge, and the anterior transition to the CA ligament.
- Stop medially at the AC joint — do not enter the joint unless AC pathology dictates a distal clavicle excision.
- With clear visualisation, assess the cuff thoroughly from the bursal surface and probe it for integrity: full-thickness tears (already assessed from the articular side), bursal-sided partial tears, cuff thinning, and degenerative change.
- Decision rule: a partial tear less than 50 percent of thickness from one side — debridement only; a partial tear greater than 50 percent, or combined articular plus bursal greater than 50 percent total — consider completion and repair. A full-thickness tear is repaired.
- If AC joint arthritis is present (osteophytes, joint-space narrowing, a positive cross-body adduction test), perform a distal clavicle excision: identify the AC joint capsule medially, resect 5-7mm of distal clavicle with the burr, creating a 5-7mm gap.
- Preserve the superior and posterior capsule for stability; remove anterior and inferior bone only. Test stability — translation should be less than 5mm.
- Inadequate resection (less than 5mm) causes persistent pain; excessive resection (greater than 10mm) or capsule violation causes AC instability.
- Achieve meticulous haemostasis with radiofrequency or epinephrine irrigation; briefly reduce the arthroscopic pump pressure to unmask bleeding sources.
- Remove loose bone fragments and debris. Final check: smooth acromion undersurface, no residual spur or osteophyte, intact (or repaired) cuff, adequate subacromial space, AC joint addressed if needed.
- Test impingement — with the cuff gliding freely under the acromion through full range of motion, there should be no mechanical block.
- Test passive range of motion — forward flexion, abduction, internal and external rotation — which should be full or near-full and smooth without catching or grinding.
- If motion is limited, assess the cause: inadequate decompression (revise), adhesive capsulitis (gentle manipulation under anaesthesia), or cuff pathology. Document the final range.
- Irrigate the subacromial space thoroughly. Inject a long-acting local anaesthetic with epinephrine into the space (e.g. 20mL of 0.25 percent Marcaine with 1:200,000 epinephrine) for 12-18 hours of postoperative pain control.
- A corticosteroid injection is controversial — it may improve early pain but raises concerns about healing, especially if a cuff repair was performed. Remove instruments under direct vision, close portals with nylon or absorbable suture, and apply sterile dressings.
- For an isolated decompression, apply a sling for comfort only (1-3 days) and begin immediate active and passive range of motion with no restrictions — this is fundamentally different from a cuff repair, which must be protected. Physiotherapy starts day 1-2.
- Strengthening of the rotator cuff and scapular stabilisers begins at 2-4 weeks. Return to sedentary work at 1-2 weeks, manual labour at 6-8 weeks, non-contact sport at 6-8 weeks and contact sport at 10-12 weeks.
- Emphasise realistic expectations: gradual pain improvement over 3-6 months, and that recurrence is possible if underlying biomechanics (scapular dyskinesis, posture) are not addressed with therapy.
Courses 5-7cm (range 4.5-8cm) distal to the lateral acromion, wrapping the surgical neck of the humerus through the quadrangular space; innervates deltoid, teres minor and the lateral shoulder skin. Protect it by keeping the lateral portal within 2-3cm of the acromion and avoiding distal instrumentation.
Arises from the anterior border and superior surface of the acromion, extending 2-3cm posteriorly. The burr must stay on the inferior surface only and never extend beyond the anterior edge or onto the superior surface; limit resection to 5-7mm to preserve it.
Through the suprascapular notch (beneath the superior transverse scapular ligament) to supraspinatus, then around the spinoglenoid notch to infraspinatus. At risk only with excessive medial acromioplasty beyond the scapular base.
Supraspinatus lies directly beneath the subacromial space (footprint 1.5cm x 1.5cm on the superior facet of the greater tuberosity); infraspinatus lies posteriorly on the middle facet. Protect both with oscillating shaver use and a burr oriented superiorly, and probe the cuff before and after acromioplasty.
Pierces coracobrachialis 5-8cm (mean 6cm) distal to the coracoid. At risk only if an anterior portal is placed too medial or distal — keep it lateral to the coracoid and use outside-in spinal needle localisation.
Over-resection of the acromion (more than 7-10mm) detaches the deltoid origin and risks acromion fracture; a lateral portal placed more than 5cm distal to the acromion injures the axillary nerve. Both are prevented by marking the safe zone preoperatively, staying on the inferior acromial surface, and limiting bone removal to 5-7mm. If an iatrogenic full-thickness cuff tear is recognised, repair it at the same sitting and convert to a cuff-repair rehabilitation protocol.
You cannot safely perform acromioplasty through a hypertrophic, inflamed bursa. Complete bursectomy first — it is the step that makes every subsequent step safe and is the single most common reason for inadequate or dangerous decompression when skipped.
Aftercare & Complications
Rehabilitation The protocol depends on whether the decompression was isolated or combined with a cuff repair. | Phase / situation | Immobilisation | Range of motion | Strengthening | Return to activity | |-------------------|----------------|-----------------|---------------|--------------------| | Isolated SAD (no cuff repair) | Sling for comfort 1-3 days | Immediate active and passive, no restriction | Rotator cuff and scapular stabilisers at 2-4 weeks | Sedentary 1-2 weeks, manual 6-8 weeks, contact sport 10-12 weeks | | With concurrent cuff repair | Sling 4-6 weeks continuous | Passive only 0-6 weeks, active-assisted 6-12 weeks, active after 12 weeks | Delayed until 12+ weeks | Prolonged, 4-6 months | Pain management is multimodal: acetaminophen and NSAIDs, minimal opioids (3-5 days), a subacromial local anaesthetic injection for the first 12-18 hours, and ice for 48-72 hours. Expect gradual improvement over 3-6 months, not immediate resolution. Wound care: waterproof dressings for 48 hours, shower after 48 hours, no submersion for 2 weeks, suture removal at 10-14 days, and monitor for infection (increasing pain, erythema, drainage, fever). Follow-up at 2 weeks (wound and ROM), 6 weeks (advance strengthening), 3 months (return-to-activity clearance) and 6-12 months (final outcome). Complications
- Recognition
- Pain unchanged at 3-6 months; may indicate wrong diagnosis (non-mechanical, cervical referred, multifactorial) or inadequate decompression with residual spur
- Prevention
- Meticulous selection for true mechanical impingement, complete bursectomy and adequate acromioplasty
- Management
- Re-evaluate the diagnosis (cervical spine, CT for bone, MRI for cuff, diagnostic injection); revision SAD only if a mechanical cause is confirmed
- Recognition
- Progressive global loss of passive and active ROM in the first 6 weeks
- Prevention
- Immediate mobilisation, sling for comfort only 1-3 days, early physiotherapy
- Management
- Aggressive ROM therapy, NSAIDs, suprascapular nerve block; manipulation or capsular release if refractory beyond 3 months
- Recognition
- Abduction weakness against gravity, pain with deltoid contraction, contour deformity, deltoid avulsion on MRI
- Prevention
- Limit acromioplasty to the undersurface, never extend onto the superior surface or beyond the anterior edge, resect 5-7mm maximum
- Management
- Partial: therapy and deltoid strengthening. Complete detachment: surgical repair to the acromion with suture anchors or bone tunnels, then 6-8 weeks protection
- Recognition
- Acute postoperative pain and crepitus over the acromion, fracture line on X-ray (often a stress fracture weeks post-op)
- Prevention
- Limit resection to 5-7mm (never more than 10mm), conservative in thin Type I acromia and elderly osteoporotic bone
- Management
- Most treated in a sling for 4-6 weeks; displaced or non-united: ORIF with plate and screws
- Recognition
- New postoperative weakness and positive cuff lag signs, new full-thickness tear on MRI
- Prevention
- Oscillating shaver with suction away from cuff, burr oriented superiorly, probe the cuff before and after acromioplasty
- Management
- If recognised intra-operatively: immediate repair and a cuff-repair protocol. Postoperative: re-operation if a significant tear
- Recognition
- Deltoid paralysis, inability to abduct, numbness over the lateral shoulder (badge area), confirmed on EMG/NCS at 3-4 weeks
- Prevention
- Lateral portal 2-3cm (never more than 5cm) below the acromion, outside-in spinal needle localisation
- Management
- Most are neuropraxia — observe and maintain ROM with recovery at 3-6 months; explore and graft if no recovery
Additional complications: recurrent impingement from inadequate decompression; suprascapular nerve injury from excessive medial dissection (rare, less than 0.5 percent); deep or superficial infection (0.5-1 percent, lower than open surgery); AC joint instability after excessive distal clavicle excision (more than 10mm or capsule violation); haematoma requiring drainage; instrument breakage with a retained fragment; and soft-tissue fluid extravasation (extensive subcutaneous emphysema; pneumothorax is rare).
Viva & Exam Focus
BURSABURSA — key technical principles
PORTALSPORTALS — shoulder arthroscopy setup
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old manual labourer has 18 months of anterolateral shoulder pain worse with overhead activity. He has failed 6 months of physiotherapy and two subacromial corticosteroid injections. Examination shows positive Neer and Hawkins signs, full passive ROM, and 4/5 abduction strength. MRI shows subacromial bursal thickening, a Bigliani Type III hooked acromion with an anteroinferior spur, and an intact rotator cuff. How would you manage him?”
“You perform an arthroscopic subacromial decompression on a 48-year-old with a 2-year history of shoulder impingement. At 6 months he returns with persistent anterolateral shoulder pain unchanged from before surgery, despite compliance with physiotherapy. How do you approach him?”
“During arthroscopic acromioplasty, bleeding obscures your view. Once you achieve haemostasis and clear visualisation, you probe the cuff and find a 2cm full-thickness supraspinatus tear you believe is iatrogenic. How do you manage this intra-operative complication?”
Indications
- Subacromial impingement failing 3-6 months conservative care (PT, NSAIDs, injections)
- Positive Neer and Hawkins signs, painful arc 60-120 degrees, full passive ROM
- Bigliani Type II/III acromion with an anteroinferior spur on the outlet view, intact cuff on MRI
- Positive subacromial injection test (greater than 50 percent relief predicts success)
- CSAW showed no benefit over sham — reserve for TRUE mechanical impingement with a structural acromion abnormality
Critical steps
- Beach chair 60-70 degrees, mark all bony landmarks (anterior, lateral, posterior acromion, AC joint, coracoid)
- Posterior portal at the soft spot (2cm inferior, 1cm medial to the posterolateral corner); diagnostic glenohumeral arthroscopy first
- Lateral working portal 2-3cm distal to the lateral acromion (axillary nerve 5-7cm danger zone), in line with the posterior clavicle
- Enter the subacromial space from the posterior portal — redirect superiorly/posteriorly, feel the pop
- COMPLETE bursectomy — the most critical step for visualisation
- Acromioplasty with a 5.0-5.5mm burr: flat Type I undersurface, remove the spur, limit resection to 5-7mm maximum
- Smooth contouring, test with a probe, stop at the AC joint medially
Danger zones
- Axillary nerve: 5-7cm distal to the lateral acromion — lateral portal must stay within 2-3cm
- Deltoid origin: anterior border and superior acromion surface — burr on the undersurface only, 5-7mm maximum
- Suprascapular nerve: avoid excessive medial dissection beyond the scapular base
- Rotator cuff: oscillating shaver, burr oriented superiorly, probe before and after
- Musculocutaneous nerve: anterior portal lateral to the coracoid, outside-in technique
CA ligament and cuff decisions
- CA ligament: preserve (modern) as a superior restraint especially with cuff deficiency; debride only thickened portions
- Partial cuff tear less than 50 percent: debridement only
- Partial tear greater than 50 percent or combined greater than 50 percent: consider completion and repair
- Full-thickness tear: repair
Complications
- Persistent pain 10-20 percent (often wrong diagnosis or inadequate decompression)
- Stiffness or frozen shoulder 5-10 percent (prevent with immediate ROM)
- Deltoid dysfunction 1-3 percent (over-aggressive acromioplasty greater than 7mm)
- Acromion fracture less than 1 percent (resection greater than 10mm)
- Iatrogenic cuff injury 1-2 percent; axillary nerve injury less than 1 percent
Post-op protocol
- Isolated SAD: sling for comfort 1-3 days, immediate active and passive ROM, PT day 1-2
- Strengthening at 2-4 weeks; return to sedentary work 1-2 weeks, manual 6-8 weeks, contact sport 10-12 weeks
- Pain resolves gradually over 3-6 months, not immediately
- With a concurrent cuff repair: convert to sling 4-6 weeks, passive-only ROM, delayed strengthening after 12 weeks
Exam tips
- On CSAW: no benefit over sham in unselected patients, but I reserve SAD for true mechanical impingement (Type III acromion with a spur)
- On the CA ligament: preserve as a superior restraint especially with cuff deficiency
- On failed SAD: re-evaluate with CT (residual spur, os acromiale), MRI (cuff), and a diagnostic injection; inadequate decompression is most common but exclude wrong diagnosis
- On iatrogenic cuff injury: repair immediately if able, convert to a cuff-repair protocol, document and communicate honestly
Background & Evidence
Pathophysiology. Subacromial impingement is best understood as a combined model. Extrinsic compression — the rotator cuff squeezed between the humeral head and the coracoacromial arch during the 60-120 degree impingement zone of forward flexion — is driven by acromial morphology (Type III hooked), anteroinferior acromial spurs, AC joint osteophytes, CA ligament thickening or ossification, os acromiale instability, and bursal hypertrophy. Intrinsic cuff degeneration — age-related tendon wear with hypovascularity of the supraspinatus critical zone 1cm proximal to its insertion — may occur without any impingement and explains why some patients fail decompression (the problem is the tendon, not the arch). Most symptomatic patients have elements of both, with bursal inflammation amplifying the pain. Acromial morphology and the structural argument. The acromion is 4-5cm anteroposteriorly, 2.5-3cm wide and only 7-10mm thick (the reason resection is limited). An unfused acromial apophysis — os acromiale — is present in 3-15 percent of the population (bilateral in 60 percent), typically at the meso-acromion; a mobile fragment impinges with deltoid contraction and is a classic cause of failed SAD if missed on the axillary lateral. It is managed by acromioplasty alone if small and stable, ORIF if large and unstable, and excision if highly unstable with a cuff tear (only when less than two-thirds of the acromion).
- Morphology
- Flat undersurface
- Prevalence
- 10%
- Impingement risk and management
- Minimal impingement risk — usually does not need acromioplasty; if symptomatic, search for another cause
- Morphology
- Curved undersurface
- Prevalence
- 40%
- Impingement risk and management
- Moderate risk — may benefit from conservative anteroinferior decompression
- Morphology
- Hooked with a prominent anteroinferior hook
- Prevalence
- 50%
- Impingement risk and management
- Highest impingement risk — a clear mechanical block, the primary indication for decompression; strongly associated with cuff tears
- Typical age
- Less than 25 years
- Pathology
- Edema and haemorrhage of the bursa and cuff — reversible
- Management
- Conservative (rest, NSAIDs, PT); surgery rarely indicated
- Typical age
- 25-40 years
- Pathology
- Fibrosis and tendinitis, bursal thickening, possible partial-thickness tears
- Management
- Conservative 3-6 months first; the primary surgical candidates for isolated SAD if mechanical impingement is confirmed
- Typical age
- Greater than 40 years
- Pathology
- Bone spurs and tendon rupture — irreversible; anteroinferior acromial osteophytes, full-thickness cuff tears, AC arthritis
- Management
- Surgery usually required (SAD plus cuff repair plus DCE as indicated); outcomes depend on cuff tear size and reparability
Differential diagnosis to exclude before offering SAD. Internal impingement (posterior cuff against the posterosuperior glenoid in the throwing position, with SLAP and PASTA lesions — treated with rehabilitation or labral repair, NOT SAD); cervical radiculopathy (C5-C6, positive Spurling test); adhesive capsulitis (global passive and active restriction); calcific tendinitis (acute severe pain, calcium on X-ray); and a true rotator cuff tear (weakness, positive lag signs — repair, not isolated SAD). Guidelines, registries and global practice. The modern evidence base is dominated by high-quality placebo-controlled randomised trials that have substantially narrowed the indications for isolated decompression. The default across major society guidance is now a prolonged exercise-first pathway, with surgery reserved for selected mechanical impingement after structured non-operative care has genuinely failed. | Body / region | Position on isolated ASD for impingement | |---|---| | BESS / BOA (UK) | Prolonged structured exercise first-line; surgery only after genuine failure of high-quality non-operative care, with shared decision-making citing CSAW | | AAOS (US) | Emphasises non-operative management for impingement without a structural cuff tear; weak or limited evidence for routine acromioplasty | | EFORT / European consensus | Exercise-led pathway; acromioplasty reserved for clear mechanical impingement (a hooked acromion, a subacromial osteophyte) | | Nordic practice (Finnish FICEBO, Swedish) | Strongly exercise-first following FIMPACT and the Ketola long-term data | High-resource systems have markedly reduced isolated ASD volumes since 2018 in response to CSAW and FIMPACT. In lower-resource settings where prolonged supervised physiotherapy is less accessible, thresholds for offering decompression may differ, but the underlying evidence (no benefit over placebo for an intact cuff) is universal. There is no global consensus mandating routine acromioplasty at the time of cuff repair — the meta-analytic evidence supports a selective rather than routine approach worldwide.
Arthroscopic subacromial decompression for subacromial shoulder pain (CSAW)
- Multicentre placebo-controlled three-group RCT: 313 patients (decompression versus arthroscopy-only placebo versus no treatment), intact cuff, all had failed exercise plus at least one steroid injection
- No difference in Oxford Shoulder Score at 6 months between decompression and placebo arthroscopy (mean difference -1.3 points, 95 percent CI -3.9 to 1.3)
- Both surgical groups beat no treatment by only 2.8-4.2 points — below the clinically important threshold of 4.5 points (likely placebo effect plus postoperative physiotherapy)
Subacromial decompression versus diagnostic arthroscopy for shoulder impingement (FIMPACT)
- Finnish multicentre double-blind sham-controlled RCT: 210 patients randomised to ASD, diagnostic arthroscopy (placebo), or exercise therapy, with 24-month follow-up
- No clinically relevant difference in pain VAS between ASD and placebo diagnostic arthroscopy at rest (-4.6) or on activity (-9.0), both below the 15-point minimal clinically important difference
- The apparent advantage of ASD over exercise did not exceed the minimal clinically important difference and was biased by selective loss of poor-prognosis patients from the surgical arm
No evidence of long-term benefits of arthroscopic acromioplasty in shoulder impingement: 5-year RCT
- 140 patients with stage II impingement randomised to supervised exercise alone versus acromioplasty plus the same exercise programme
- At 5 years both groups improved markedly in VAS pain (exercise 6.5 to 2.2; combined 6.4 to 1.9) with continued improvement between 2 and 5 years
- No statistically significant difference between groups in any patient-centred outcome — the authors concluded acromioplasty is not cost-effective
Role of subacromial decompression in arthroscopic full-thickness rotator cuff repair: systematic review and meta-analysis
- Level I systematic review of 4 randomised trials and 373 patients undergoing arthroscopic repair of full-thickness cuff tears, with or without concomitant acromioplasty
- No statistically significant difference in ASES or Constant scores or re-operation rate between repair with versus without acromioplasty at intermediate follow-up
- No difference in disease-specific quality of life (Western Ontario Rotator Cuff index) between groups
Acromion morphology and prevalence of rotator cuff tear: systematic review and meta-analysis
- Pooled 17 studies (1993-2017); acromion type analysed in 11 and acromial index in 10
- Type III (hooked) acromion carried almost three times the odds of a rotator cuff tear versus Type I or II (overall OR 2.82, p=0.000003)
- A larger acromial index was independently associated with a greater likelihood of a non-traumatic cuff tear (raw mean difference 0.071, p less than 0.0000001)
References
- Beard DJ, Rees JL, Cook JA, et al. Arthroscopic subacromial decompression for subacromial shoulder pain (CSAW): a multicentre, pragmatic, parallel group, placebo-controlled, three-group, randomised surgical trial. Lancet. 2018;391(10118):329-338. doi:10.1016/S0140-6736(17)32457-1 2. Paavola M, Malmivaara A, Taimela S, et al. Subacromial decompression versus diagnostic arthroscopy for shoulder impingement: randomised, placebo surgery controlled clinical trial. BMJ. 2018;362:k2860. doi:10.1136/bmj.k2860 3. Hao Q, Devji T, Zeraatkar D, et al. Minimal important differences for improvement in shoulder condition patient-reported outcomes: a systematic review to inform a BMJ Rapid Recommendation. BMJ Open. 2019;9(2):e028777. doi:10.1136/bmjopen-2018-028777 4. Bigliani LU, Morrison DS, April EW. The morphology of the acromion and its relationship to rotator cuff tears. Orthop Trans. 1986;10:228. 5. Neer CS 2nd. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972;54(1):41-50. 6. Chahal J, Mall N, MacDonald PB, et al. The role of subacromial decompression in patients undergoing arthroscopic repair of full-thickness tears of the rotator cuff: a systematic review and meta-analysis. Arthroscopy. 2012;28(5):720-727. doi:10.1016/j.arthro.2011.11.022 7. Ketola S, Lehtinen J, Rousi T, et al. No evidence of long-term benefits of arthroscopic acromioplasty in the treatment of shoulder impingement syndrome: five-year results of a randomised controlled trial. Bone Joint Res. 2013;2(7):132-139. doi:10.1302/2046-3758.27.2000163 8. Sambandam SN, Khanna V, Gul A, Mounasamy V. Rotator cuff tears: an evidence based approach. World J Orthop. 2015;6(11):902-918. doi:10.5312/wjo.v6.i11.902 9. Karnes JM, Harrier CD, Bernas GA, Weiss AP, Akelman E. Anterior portal anatomy for shoulder arthroscopy: defining a safety zone. Arthroscopy. 2014;30(12):1521-1525. doi:10.1016/j.arthro.2014.07.011 10. Ponce BA, Kundukulam JA, Pflugner R, Abrams RA, Vrahas MS. Shoulder arthroscopy in the beach chair position: risk of arterial air embolism. Arthroscopy. 2009;25(4):481-482. doi:10.1016/j.arthro.2009.01.006