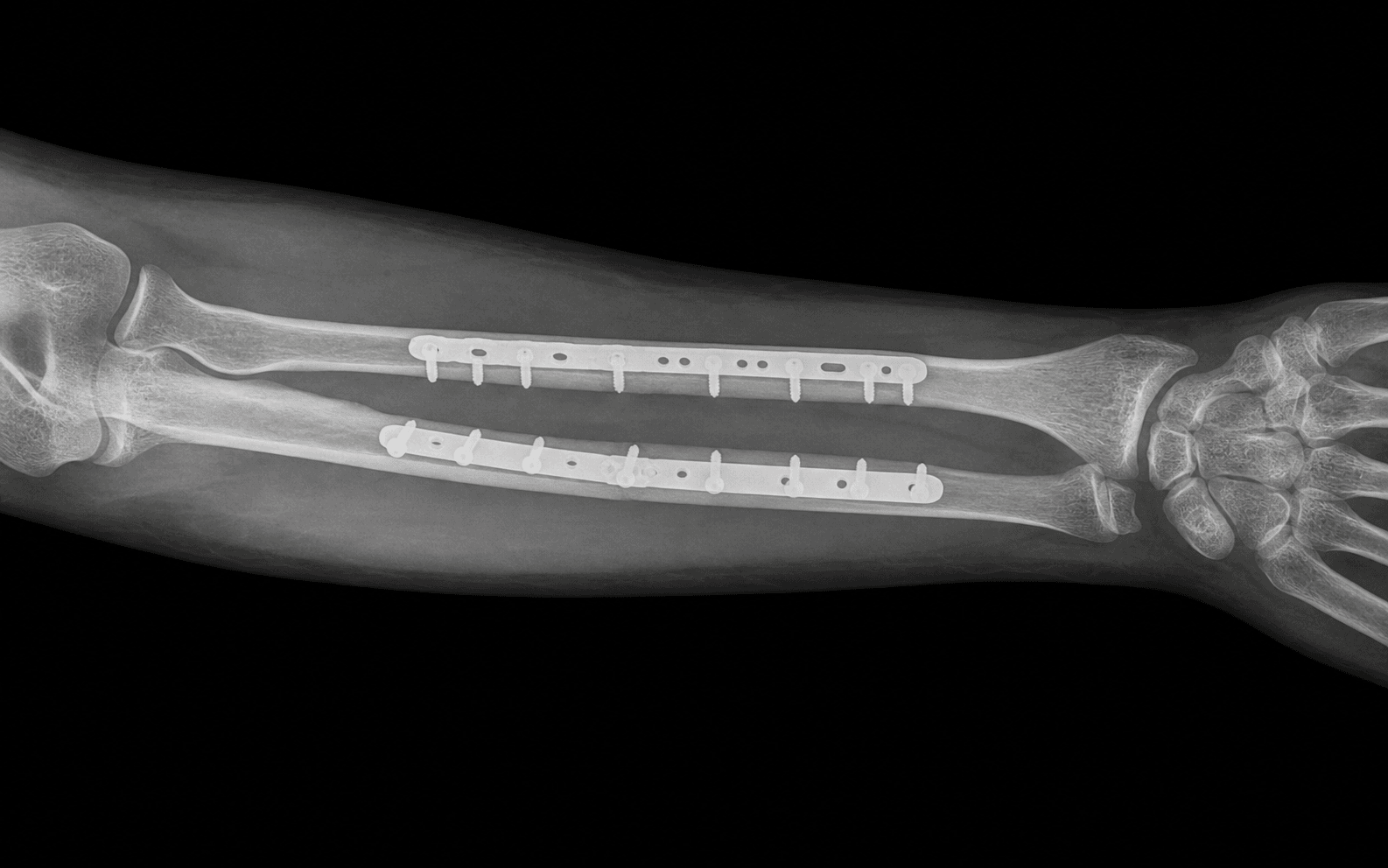
Anatomical reduction and rigid plate fixation of the adult both-bone forearm to restore the radial bow and forearm rotation
- The forearm functions as a JOINT, not two long bones: the radius rotates around the ulna, so a both-bone shaft fracture is an intra-articular-equivalent injury. ORIF must restore length, rotation, axial alignment and the RADIAL BOW so that the radius can clear the ulna through pronation and supination. Anatomical reduction is mandatory; malreduction of the radial bow directly costs forearm rotation.
- Almost all DISPLACED adult both-bone forearm fractures require ORIF. Closed and cast treatment reliably fails because the deforming forces (biceps, supinator, pronator teres, pronator quadratus) cannot be controlled well enough to maintain the bow and interosseous space. Compression plating with 3.5 mm plates is the gold standard.
- Schemitsch and Richards showed that restoring the radius's normal radial bow (both its location and magnitude) correlates with recovery of forearm rotation and grip strength, so loss of the bow predicts loss of rotation. Each bone is reduced and plated separately, restoring the interosseous space.
- Use SEPARATE incisions for the radius and ulna whenever possible. A single combined incision and a shared surgical bed markedly raise the risk of radioulnar synostosis. Synostosis risk is highest with high-energy injuries, head injury, fractures at the same level, and bone graft placed in the interosseous space.
When & Why
The core principle. The radius and ulna form a functional unit, a forearm joint, linked proximally at the proximal radioulnar joint, distally at the distal radioulnar joint (DRUJ), and along the shaft by the interosseous membrane. The radius rotates around a relatively fixed ulna to produce pronation and supination, sweeping in its characteristic lateral radial bow so that it clears the ulna. Because of this, a displaced both-bone shaft fracture is biomechanically equivalent to an intra-articular fracture: anything less than anatomical restoration of length, rotation, axial alignment and the radial bow compromises rotation. (The biomechanics and deforming forces are laid out in full under Background and Evidence.) Absolute indications - Displaced both-bone forearm fracture in an adult (the overwhelming majority) where closed treatment fails to maintain reduction
- Open fractures, managed with debridement plus plate fixation when the soft tissues allow
- Galeazzi fracture (radial shaft plus DRUJ disruption), a fracture of necessity
- Monteggia fracture (proximal ulna plus radial head dislocation), requiring anatomic ulna fixation
- Fractures with compartment syndrome requiring fasciotomy, stabilising the skeleton at the same setting Relative indications - Minimally displaced both-bone fractures in adults, still usually fixed because even minor malalignment costs rotation
- Segmental or comminuted patterns, managed with bridge-plating principles to restore length, alignment and rotation
- Polytrauma, where early skeletal stabilisation aids overall management Contraindications and cautions - Absolute: active infection at the operative site (treat infection first) or a non-reconstructable, contaminated soft-tissue envelope (temporise with external fixation)
- Relative: children with substantial remodelling potential, in whom most both-bone fractures are managed by closed reduction or flexible intramedullary nailing rather than rigid plating; and severe comorbidity precluding anaesthesia Named forearm fracture-dislocations. These patterns define the injuries that demand operative fixation and the joints you must not miss:
- Components
- Radius and ulna shaft fractures
- Key Principle
- Separate ORIF of each bone; restore the bow and the interosseous space
- Pitfall
- Over-straightening the radius (a lost bow)
- Components
- Radial shaft fracture plus DRUJ disruption
- Key Principle
- Fix the radius anatomically, then stabilise the DRUJ
- Pitfall
- Missing the DRUJ injury; a 'fracture of necessity'
- Components
- Proximal ulna fracture plus radial head dislocation
- Key Principle
- Anatomic ulna fixation reduces the radial head
- Pitfall
- Missing the radial head dislocation; residual ulnar malreduction
- Components
- Radial head fracture plus IOM and DRUJ disruption
- Key Principle
- Preserve or replace the radial head; protect length
- Pitfall
- Treating the radial head in isolation causes proximal migration
- Components
- Isolated ulnar shaft fracture
- Key Principle
- Often non-operative if minimally displaced; ORIF if displaced
- Pitfall
- Failing to exclude a Monteggia (image the elbow)
Why cast treatment fails in adults. Powerful deforming forces act on the radius that a cast cannot neutralise: biceps and supinator supinate the proximal fragment, pronator teres acts at the mid-shaft, and pronator quadratus pronates the distal fragment. Maintaining the radial bow and interosseous space in plaster is unreliable, and historical closed-treatment series in adults show high rates of malunion, loss of rotation and nonunion, which is why rigid plate fixation became the standard. Timing and open fractures. Open fractures need urgent debridement with tetanus and antibiotic prophylaxis; definitive plate fixation at the index procedure is appropriate for most Gustilo I to IIIA injuries with a clean, closable wound. With severe contamination or type IIIB to IIIC injuries, consider temporary external fixation and staged definitive fixation. Compartment syndrome demands emergent fasciotomy and must not wait for fixation logistics. Goals of fixation — the Four Restorations. Restore length, restore rotation (using the bicipital tuberosity and radial styloid relationship and the oblique fracture-line key), restore axial alignment in both planes, and restore the radial bow in both magnitude and apex location. Setup and consent. Supine, arm on a radiolucent hand table, upper-arm tourniquet, the arm prepared and draped free to allow full pronation and supination and intra-operative imaging. General or regional (supraclavicular or axillary block) anaesthesia, antibiotic prophylaxis at induction, tetanus cover for open injuries. Counsel specifically regarding PIN and nerve injury, radioulnar synostosis, loss of forearm rotation, nonunion or malunion, infection, compartment syndrome, possible bone graft, and later plate removal with refracture risk.
The Operation
The goal is to anatomically reduce and rigidly fix each bone through separate incisions, protecting the posterior interosseous nerve and the interosseous membrane, restoring the radial bow, and confirming rotation and the radio-ulnar joints on the table. The exposure of each bone is laid out in full as the first steps of the sequence below.
Operative sequence
- Supine, radiolucent hand table, upper-arm tourniquet; the arm is free to pronate and supinate fully.
- A contralateral forearm radiograph is available as a template for the radial bow.
- Plan TWO separate incisions from the outset: a Henry (volar) or Thompson (dorsal) incision for the radius, and a separate subcutaneous-border incision for the ulna. Keeping the incisions and surgical beds separate is one of the most important things you do to reduce radioulnar synostosis risk.
- The ulna is subcutaneous along its dorsal border and directly palpable. Incise straight onto the crest in the interval between flexor carpi ulnaris (ulnar nerve) and extensor carpi ulnaris (PIN).
- Develop the plane directly onto bone, keeping the ulnar nerve and artery (which lie volar) protected; they are safe if dissection stays on the subcutaneous crest.
- Expose the fracture with minimal periosteal stripping. This is a separate incision and a separate bed from the radius.
- Henry (anterior/volar): develop the plane between brachioradialis (radial nerve) and pronator teres (median nerve) proximally, and between brachioradialis and flexor carpi radialis (median nerve) distally. It exposes the whole volar radius and is the workhorse for shaft and distal-third (Galeazzi) fractures.
- Henry PIN protection: in the proximal radius, keep the forearm fully SUPINATED so the supinator insertion (and the PIN within it) rotates dorsally away from the field at the radial neck.
- Henry hazards: distally, protect the superficial radial nerve and the radial artery beneath brachioradialis; proximally, ligate the leash of Henry (recurrent radial vessels).
- Thompson (dorsal/posterior): develop the plane between extensor carpi radialis brevis (radial nerve) and extensor digitorum communis (PIN) proximally, and between ECRB and extensor pollicis longus distally. It is best for the proximal and middle thirds.
- Thompson PIN protection: the PIN runs WITHIN the supinator here, so positively identify and protect it before any subperiosteal dissection; pronate the forearm to carry the insertion away laterally. Thompson carries a higher reported PIN injury rate than Henry for the proximal radius.
- Reduce the simpler fracture anatomically first (often the ulna via its straightforward subcutaneous approach, or whichever fracture is more transverse).
- Set rotation using the oblique or spiral fracture-line key, the bicipital tuberosity orientation (radius) and the subcutaneous crest (ulna).
- Hold provisionally with reduction forceps, or a lag screw for oblique patterns.
- Reduce the second bone, confirming that overall length and rotation are balanced between the two bones.
- The first fixed bone acts as a template and strut for restoring length.
- Reduce the radius restoring BOTH the magnitude and the location of the radial bow.
- Compare intra-operatively with the contralateral forearm radiograph. A radius reduced to length but left too straight must be re-reduced, because an over-straightened radius narrows the interosseous space and blocks rotation.
- Apply a 3.5 mm plate (LC-DCP or locking compression plate) to each bone.
- For transverse or short-oblique fractures use the plate in compression mode (eccentric drilling or an articulated tensioner).
- For long-oblique or spiral fractures place an interfragmentary lag screw and apply the plate as a neutralisation plate.
- Aim for at least six cortices (three bicortical screws) on each side of the fracture.
- For comminution or segmental bone loss, consider autograft (iliac crest) or bridge plating that maintains length without disturbing the comminuted zone.
- Keep all graft OUT of the interosseous space to avoid synostosis.
- Image both bones in two planes; confirm the restored bow and interosseous space.
- Take the forearm through full pronation and supination on the table.
- Check the DRUJ (in a Galeazzi) and the radiocapitellar line and radial head (in a Monteggia) where relevant.
- Assess the compartments before closure. Close the fascia loosely or leave it open if swelling is significant, and close the skin without tension.
- Apply a well-padded plaster slab in a comfortable position.
- Document the post-operative neurovascular examination, especially PIN and radial nerve function.
- Henry (Anterior/Volar)
- Brachioradialis (radial n.) / pronator teres (median n.)
- Thompson (Dorsal/Posterior)
- ECRB (radial n.) / EDC (PIN)
- Henry (Anterior/Volar)
- Whole shaft, distal third (Galeazzi)
- Thompson (Dorsal/Posterior)
- Proximal and middle thirds
- Henry (Anterior/Volar)
- Full supination displaces the PIN dorsally at the radial neck
- Thompson (Dorsal/Posterior)
- Identify and protect the PIN within the supinator; pronate to move the insertion away
- Henry (Anterior/Volar)
- Superficial radial nerve, radial artery under brachioradialis
- Thompson (Dorsal/Posterior)
- Less distal neurovascular risk
- Henry (Anterior/Volar)
- Leash of Henry (recurrent radial vessels)
- Thompson (Dorsal/Posterior)
- PIN injury (higher reported rate)
- Henry (Anterior/Volar)
- Volar (flat surface, soft-tissue cover)
- Thompson (Dorsal/Posterior)
- Dorsal / dorsoradial
Henry, proximal: protect the PIN by full supination, and ligate the leash of Henry recurrent vessels. Henry, distal: gently retract the superficial radial nerve and radial artery beneath brachioradialis. Thompson: the PIN lies within the supinator, so identify and protect it before any subperiosteal dissection. Ulna: the ulnar nerve and artery lie volar, so stay on the subcutaneous border.
For the radius I default to the Henry (anterior) approach for shaft and distal-third fractures because it gives full volar exposure and I protect the PIN proximally by fully supinating the forearm. I reserve the Thompson (dorsal) approach for proximal and middle-third work, where I deliberately identify and protect the PIN within the supinator. I always expose the ulna through a separate incision on its subcutaneous border, and I keep the two incisions and beds separate to reduce synostosis risk.
For a transverse both-bone fracture I plate in compression, using eccentric drilling or a tensioning device to load the fracture. For an oblique or spiral pattern I place an interfragmentary lag screw first to compress the fracture, then apply the plate as a neutralisation plate. I want at least three bicortical screws (six cortices) on each side of the fracture.
Galeazzi — specific sequence. Anatomically reduce and plate the radius (usually through the Henry approach). Then reduce and test the DRUJ: if it is reduced and stable, splint in supination; if it is reduced but unstable, pin the DRUJ in supination with one or two K-wires proximal to the joint for about six weeks and consider the TFCC; if it is irreducible, open the DRUJ, because the extensor carpi ulnaris tendon is the classic interposed structure preventing reduction. Monteggia — specific sequence. Anatomically reduce and plate the ulna, restoring length, alignment and the subtle ulnar bow. The radial head usually reduces once the ulna is anatomic; confirm the radiocapitellar line. If the radial head will not stay reduced, the ulna is not truly anatomic (residual angulation or length) or there is interposition, so revisit the ulnar reduction.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Rehabilitation | |-------|--------|----------------|----------------| | 1 | 0 to 2 weeks | Well-padded plaster slab for comfort | Early gentle active motion of elbow, wrist and fingers (rigid fixation) | | 2 | 2 to 6 weeks | Removable splint as needed | Progressive active pronation/supination, elbow and wrist motion; wound review at 10 to 14 days | | 3 | 6 to 12 weeks | Splint for heavy tasks only | Strengthening as union advances; hand therapy for stiffness and oedema | | 4 | 12 weeks and beyond | None | Return to manual work and contact sport after radiographic union and restored strength | With rigid fixation, early active motion of the elbow, wrist and fingers is encouraged from the outset. Light activities and desk work resume within one to two weeks as comfort allows; driving returns when the patient can control the vehicle safely and is out of the slab; heavy manual work and contact sport wait for radiographic union and restored strength, commonly three to four months or more. Forearm rotation can continue to improve for several months. Plate removal — counsel carefully. Routine plate removal is NOT recommended. Diaphyseal forearm plate removal carries a notable refracture risk (reported around 5 to 25 percent). Remove plates only for a clear indication (symptomatic hardware or infection) and only after solid union, generally not before 18 to 24 months, and protect the forearm from significant loading for several weeks afterwards.
I do not remove forearm plates routinely. Diaphyseal forearm plate removal has a real refracture risk, so I only remove for symptomatic hardware or infection, after solid union (usually well beyond 18 to 24 months), and I protect the limb afterwards.
Synostosis surveillance. Track pronation and supination at each visit; a plateau or loss of rotation prompts imaging. If synostosis is suspected, CT confirms the bridge and its maturity; intervene (excision with interposition, with or without radiotherapy or indomethacin prophylaxis) only once it is mature, then rehabilitate aggressively. Special situations. Open both-bone fractures need staged soft-tissue care with close observation for infection and compartment syndrome. A Galeazzi injury is often immobilised post-operatively in supination if the DRUJ was unstable or pinned, and the DRUJ wires come out at about six weeks before mobilising rotation. A Monteggia injury needs confirmation and protection of the radial head reduction, with early gentle motion once the ulnar fixation is stable.
- Incidence
- approx 1 to 10 percent (higher with proximal/Thompson exposure)
- Recognition
- Post-op finger/thumb extension weakness (PIN); altered sensation (superficial radial n.); a pure PIN palsy has no sensory loss
- Prevention and Management
- Prevention: full supination in Henry; positively identify and protect the PIN within the supinator in Thompson; gentle retraction. Management: most traction neurapraxias recover over 8 to 12 weeks with serial exams and splinting; explore if transection is suspected or there is no recovery by about 3 months
- Incidence
- approx 2 to 9 percent (higher with single incision, same-level fractures, head injury, high-energy)
- Recognition
- Progressive loss of pronation/supination; a bony bridge across the interosseous space on imaging
- Prevention and Management
- Prevention: separate incisions, preserve the interosseous membrane, keep graft out of the interosseous space, minimise soft-tissue trauma. Management: let it mature (CT confirms), then excision with interposition (fat or muscle) with or without single-dose radiotherapy or indomethacin; aggressive early rehab
- Incidence
- variable
- Recognition
- Reduced forearm rotation despite union; a flattened or over-straightened radius versus the contralateral side
- Prevention and Management
- Prevention: restore the bow intra-operatively, template against the contralateral forearm, confirm rotation on the table. Management: corrective osteotomy with re-plating to restore the bow if functionally limiting
- Incidence
- approx 2 to 5 percent (higher in open/comminuted, smoking, infection)
- Recognition
- Persistent pain and motion at the fracture, with no bridging callus beyond expected union time
- Prevention and Management
- Prevention: stable rigid fixation, atraumatic technique, graft bone loss. Management: revision fixation with compression and autograft; treat any infection; optimise smoking and nutrition
- Incidence
- more common with high-energy/open injuries
- Recognition
- Escalating analgesia-resistant pain, pain on passive stretch, a tense compartment; late signs are pulselessness and paralysis
- Prevention and Management
- Prevention: avoid tension closure, monitor high-risk injuries. Management: emergent volar (with or without dorsal) fasciotomy; do not wait for late signs; delayed closure or skin graft as needed
- Incidence
- approx 1 to 3 percent closed; higher in open fractures
- Recognition
- Erythema, discharge, raised inflammatory markers, persistent pain; deep infection may present as nonunion
- Prevention and Management
- Prevention: antibiotic prophylaxis, thorough debridement of open injuries, careful soft-tissue handling. Management: antibiotics and debridement; retain stable implants if union is progressing, otherwise remove or revise and treat as an infected nonunion
- Incidence
- approx 5 to 25 percent reported after diaphyseal forearm plate removal
- Recognition
- A new fracture through or adjacent to the old plate or screw holes after removal, often low-energy
- Prevention and Management
- Prevention: only remove plates for a good indication after solid union (often more than 18 to 24 months); protect the limb after removal. Management: avoid unnecessary removal; if removed, protect activity for several weeks; treat refracture with re-fixation
- Incidence
- variable
- Recognition
- DRUJ pain or instability after radial fixation; persistent radial head subluxation after ulnar fixation
- Prevention and Management
- Prevention: anatomic reduction of the primary bone; intra-operative joint assessment. Management: Galeazzi, pin the DRUJ in supination or open for an interposed ECU; Monteggia, re-examine and revise the ulnar reduction
Viva & Exam Focus
FOREARMFOREARM — Principles of Both-Bone ORIF
SAFE BOWSAFE BOW — Intra-operative Reduction Checklist
The PIN is the deep motor branch of the radial nerve, passing through the supinator around the proximal radius, often via the arcade of Frohse. It is the structure most at risk in proximal radius exposure. In the Thompson approach, identify it within or distal to the supinator and protect it before subperiosteal dissection. In the Henry approach, fully supinate the forearm so the PIN and the supinator insertion rotate dorsally away from the field at the radial neck.
The trap is reducing the radius to length but leaving it too straight, so the radius can no longer clear the ulna and forearm rotation is lost even with a healed, well-aligned-looking fracture. Restore BOTH the magnitude and location of the radial bow and compare intra-operatively with a contralateral forearm radiograph. Schemitsch and Richards correlated bow restoration with rotation and grip recovery.
A bony bridge across the interosseous space welds the radius and ulna and abolishes rotation. Risk rises with a single combined incision, fractures at the same level, high-energy or comminuted injuries, associated head injury, and bone graft spilled into the interosseous space. Use separate incisions, keep graft out of the interosseous space, avoid stripping the interosseous membrane, and minimise soft-tissue trauma.
Recognise escalating analgesia-resistant pain, pain on passive finger or wrist stretch, and tense swollen compartments, especially in high-energy or open injuries and after fixation. Pulselessness and paralysis are LATE. Have a low threshold for compartment pressures and volar (with or without dorsal) fasciotomy. Never close skin under tension over a swollen forearm; consider leaving the fascia open.
A radial shaft fracture (classically distal third) with disruption of the DRUJ. Non-operative treatment fails, hence the name. Anatomically reduce and plate the radius first, then test and address DRUJ stability: reduced and stable means splint in supination; reduced but unstable means pin in supination; irreducible means open the DRUJ for the interposed ECU tendon or soft tissue.
A proximal ulna fracture with radial head dislocation (Bado I to IV by direction). The radial head dislocation is easily MISSED if the elbow is not imaged and the radiocapitellar line is not checked. Restore ulnar length, alignment and bow anatomically and this reduces the radial head in the great majority. Persistent dislocation means the ulna is not truly anatomic (residual angulation or length) or there is interposition.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old man falls from a ladder and sustains a closed, displaced midshaft fracture of both the radius and ulna of his dominant forearm. He is neurovascularly intact. Walk me through your management and the principles of your operation.”
“A 40-year-old woman has a displaced fracture of the distal third of the radial shaft. The ulna is intact, but she has pain and tenderness at the wrist. What is the diagnosis you must exclude, and how do you manage it?”
“Three months after both-bone forearm ORIF, a patient has united fractures but has progressively lost almost all pronation and supination. Imaging shows a bony bridge between the radius and ulna. What has happened, why, and how do you manage it?”
Core Principle
- The forearm is a JOINT: the radius rotates around the ulna, so a both-bone shaft fracture is intra-articular-equivalent
- Displaced adult both-bone fractures need anatomical ORIF; cast treatment fails (loss of bow, rotation, nonunion)
- Restore the FOUR: length, rotation, axial alignment and the RADIAL BOW
- Radial bow restoration (Schemitsch and Richards) is the key determinant of forearm rotation and grip
- Fix each bone separately through separate incisions to restore the interosseous space
Surgical Anatomy
- Radial bow: lateral apex; lets the radius clear the ulna; quantify height and location versus the contralateral side
- The interosseous membrane (central band) is the key longitudinal stabiliser; preserve it
- PIN: the deep motor branch of the radial nerve, running within the supinator around the proximal radius
- The ulna is subcutaneous along its dorsal border for a direct, safe exposure (FCU to ECU)
- Deforming forces on the radius: biceps/supinator (proximal), pronator teres (mid), pronator quadratus (distal)
Approaches to the Radius
- Henry (anterior): brachioradialis to pronator teres / FCR plane; whole shaft plus distal third (Galeazzi)
- Henry PIN protection: full SUPINATION displaces the PIN dorsally at the radial neck
- Henry distal hazards: superficial radial nerve and radial artery under brachioradialis; leash of Henry proximally
- Thompson (dorsal): ECRB to EDC plane; proximal and middle thirds; the PIN lies WITHIN the supinator, so identify and protect it
- Ulna: separate incision on the subcutaneous border (FCU to ECU)
Operative Technique — Key Steps
- 1. SEPARATE incisions for radius and ulna (synostosis prevention)
- 2. Reduce the simpler bone first (often the ulna) to restore length and act as a template
- 3. Restore the radial bow; compare with the contralateral radiograph
- 4. 3.5 mm plate: compression mode (transverse) or lag screw and neutralisation (oblique)
- 5. At least three bicortical screws (six cortices) each side of the fracture
- 6. Keep bone graft OUT of the interosseous space
- 7. Test full pronation and supination on the table; check the DRUJ and the radiocapitellar line
- 8. Assess compartments; close without tension; document nerve function
Galeazzi and Monteggia
- Galeazzi equals radial shaft plus DRUJ disruption (fracture of necessity): fix the radius, then stabilise the DRUJ
- DRUJ after fixation: stable means splint supinated; unstable means pin in supination for about 6 weeks; irreducible means open (ECU interposed)
- Monteggia equals proximal ulna fracture plus radial head dislocation (Bado I to IV)
- Anatomic ulna fixation reduces the radial head; if not, the ulna is malreduced or there is interposition
- Always image the wrist AND the elbow; check the radiocapitellar line
Danger Zones
- PIN at the proximal radius: supinate in Henry; identify within the supinator in Thompson
- Radioulnar synostosis: separate incisions, preserve the IOM, no graft in the interosseous space
- Loss of the radial bow: an over-straightened radius blocks rotation
- Compartment syndrome: high-energy and open injuries; a low threshold for fasciotomy
- Superficial radial nerve and radial artery under brachioradialis (distal Henry)
Complications
- PIN or nerve injury: about 1 to 10 percent; most traction palsies recover by 8 to 12 weeks
- Radioulnar synostosis: about 2 to 9 percent; excise when mature, with interposition and plus or minus prophylaxis
- Nonunion: about 2 to 5 percent; revision with compression and autograft
- Malunion or loss of bow: corrective osteotomy if functionally limiting
- Refracture after plate removal: about 5 to 25 percent; avoid routine removal
Post-op and Plate Removal
- Stable fixation allows early active motion of the elbow, wrist and fingers
- Watch for compartment syndrome in the first 24 to 48 hours
- Progressive pronation and supination; strengthening once union advances
- Do NOT remove plates routinely (refracture risk); only for a clear indication after solid union (more than 18 to 24 months)
- Protect the forearm for several weeks after any plate removal
Background & Evidence
The forearm as a joint. The radius and ulna form a functional unit linked proximally at the proximal radioulnar joint, distally at the DRUJ, and along the shaft by the interosseous membrane. The radius rotates around a relatively fixed ulna to produce pronation and supination, sweeping in its characteristic lateral radial bow so that it clears the ulna. A displaced both-bone shaft fracture is therefore biomechanically equivalent to an intra-articular fracture: anything less than anatomical restoration of length, rotation, axial alignment and the radial bow compromises rotation. This is the central principle driving operative management. The radial bow — anatomy and significance. The radius is not straight: it has a lateral (apex-radial) radial bow that lets it rotate around the ulna without impinging. The bow is quantified by its maximum height and its location along the radius (the Schemitsch and Richards method, using the contralateral radius as the template). Restoring the bow correlates with recovery of forearm rotation and grip strength; an over-straightened radius narrows the interosseous space and blocks rotation. The interosseous membrane (its central band is the key stabiliser) links the bones and transfers load, so preserving the interosseous space is essential to rotation. Why cast treatment fails — the deforming forces. Powerful muscle forces act on the radius that a cast cannot neutralise: biceps and supinator supinate the proximal fragment, pronator teres acts at the mid-shaft, and pronator quadratus pronates the distal fragment. Maintaining the radial bow and interosseous space in plaster is unreliable, and historical closed-treatment series in adults show high rates of malunion, loss of rotation and nonunion, which is why rigid plate fixation became the standard. Key evidence. Anderson and colleagues (1975) established compression-plate fixation as the standard for adult both-bone forearm fractures with high union rates. Schemitsch and Richards (1992) showed that restoration of the normal radial bow, both its magnitude and location, correlates with recovery of forearm rotation and grip strength after plate fixation. Chapman and colleagues (1989) confirmed high union and functional rates with 3.5 mm compression-plate fixation in a large series. Bot and colleagues (2011) reported long-term functional outcomes after plate fixation, and Goldfarb and colleagues (2005) documented functional recovery and residual deficits, reinforcing the importance of anatomical reduction.
References
Compression-plate fixation in acute diaphyseal fractures of the radius and ulna
Landmark series establishing compression plating as the standard for adult both-bone forearm fractures, with high union rates.
The effect of malunion on functional outcome after plate fixation of fractures of both bones of the forearm in adults
Demonstrated that restoration of the normal radial bow (its magnitude and location) correlates with recovery of forearm rotation and grip strength.
Compression-plate fixation of acute fractures of the diaphyses of the radius and ulna
Large series confirming high union and functional rates with 3.5 mm compression-plate fixation.
Long-term outcomes of fractures of both bones of the forearm
Long-term functional outcome data after plate fixation of adult both-bone forearm fractures.
Functional outcome after fracture of both bones of the forearm
Reports functional recovery and residual deficits after operative treatment, reinforcing the importance of anatomical reduction.