Posterolateral | PIN Protection via Ulnar Flap | Monteggia and Radial Head Access
- Longitudinal incision along the subcutaneous ulnar border from the olecranon onto the proximal ulnar shaft.
- The anconeus and supinator origin are elevated subperiosteally from the ulna as a SINGLE flap and reflected radially — this protects the posterior interosseous nerve within the muscle mass.
- The posterior interosseous nerve enters the supinator about 1 cm distal to the radial head and is kept safe by staying strictly on bone; it is never formally identified.
- The radial head, radial neck, annular ligament and proximal radioulnar joint are exposed for ORIF, arthroplasty or ligament reconstruction.
- Radioulnar synostosis is the feared long-term complication — never strip periosteum from the radial side of the ulna and the ulnar side of the radius in the same case.
When & Why
What it exposes. The Boyd approach is a posterolateral exposure of the proximal radius and ulna that uses a single subperiosteal flap — containing anconeus and the origin of supinator — to protect the posterior interosseous nerve while giving access to the radial head, radial neck, annular ligament and proximal ulna. It is the classic approach when both the ulna and the proximal radius must be reached through one incision. Why this approach is chosen. It allows simultaneous exposure of the proximal ulna and the radial head or neck through a single posterolateral incision, and the subperiosteal flap technique protects the posterior interosseous nerve without requiring its formal identification or dissection. It is the standard approach for Monteggia fracture-dislocations, where the ulnar fracture and the radial head dislocation are addressed together, and for radial head arthroplasty or complex ORIF combined with ulnar fixation. Primary indications - Monteggia fracture-dislocations (Bado types I to IV) requiring ulnar fixation and radial head reduction.
- Radial head fractures (Mason III or IV, or comminuted) needing ORIF or arthroplasty.
- Annular ligament reconstruction or repair in chronic Monteggia or radial head instability.
- Complex proximal ulna fractures with associated radial head or neck injury.
- Revision surgery for failed radial head fixation or malunited Monteggia. Contraindications - Active infection over the proposed incision.
- Severe soft tissue compromise requiring an alternative exposure.
- An isolated radial head fracture better accessed through the Kocher or Kaplan approach (less invasive).
- Patient factors precluding lateral positioning. Alternative approaches
- Interval
- Between anconeus and ECU
- Best for
- Isolated radial head exposure
- Limitation vs Boyd
- Less extensile; no simultaneous ulnar access
- Interval
- Between EDC and ECU (more anterior)
- Best for
- Radial head exposure
- Limitation vs Boyd
- Limited ulnar access
- Interval
- Along the radial shaft
- Best for
- Radial shaft, formal PIN exploration
- Limitation vs Boyd
- Different field; not for the proximal ulna
- Interval
- Dorsal radial shaft
- Best for
- Radial shaft distal to the supinator
- Limitation vs Boyd
- Not for the proximal ulna
Position & landmarks. Position the patient in lateral decubitus with the affected arm on a padded arm board or bolster, elbow flexed 90 degrees; a supine position with the arm across the chest (shoulder internally rotated, elbow flexed) is a widely used alternative that allows easy conversion to anterior approaches. Apply the tourniquet high on the arm with exsanguination before inflation, and prepare from axilla to wrist including the hand so forearm rotation can be assessed intraoperatively. Palpate and mark the olecranon, the lateral epicondyle, the radial head (palpable anterior to the lateral epicondyle with forearm rotation) and the subcutaneous border of the ulna. The anconeus triangle — bounded by the olecranon, the lateral epicondyle and the radial head — is the key soft-tissue landmark. Plan a longitudinal incision along the subcutaneous ulnar border, centred over the radial head for isolated radial head work and extendable proximally and distally as required.
Lateral positioning risks brachial plexus stretch, pressure injury to the dependent arm, and compartment syndrome if tourniquet time is prolonged. Document all protective measures and limit tourniquet time to less than 120 minutes when possible.
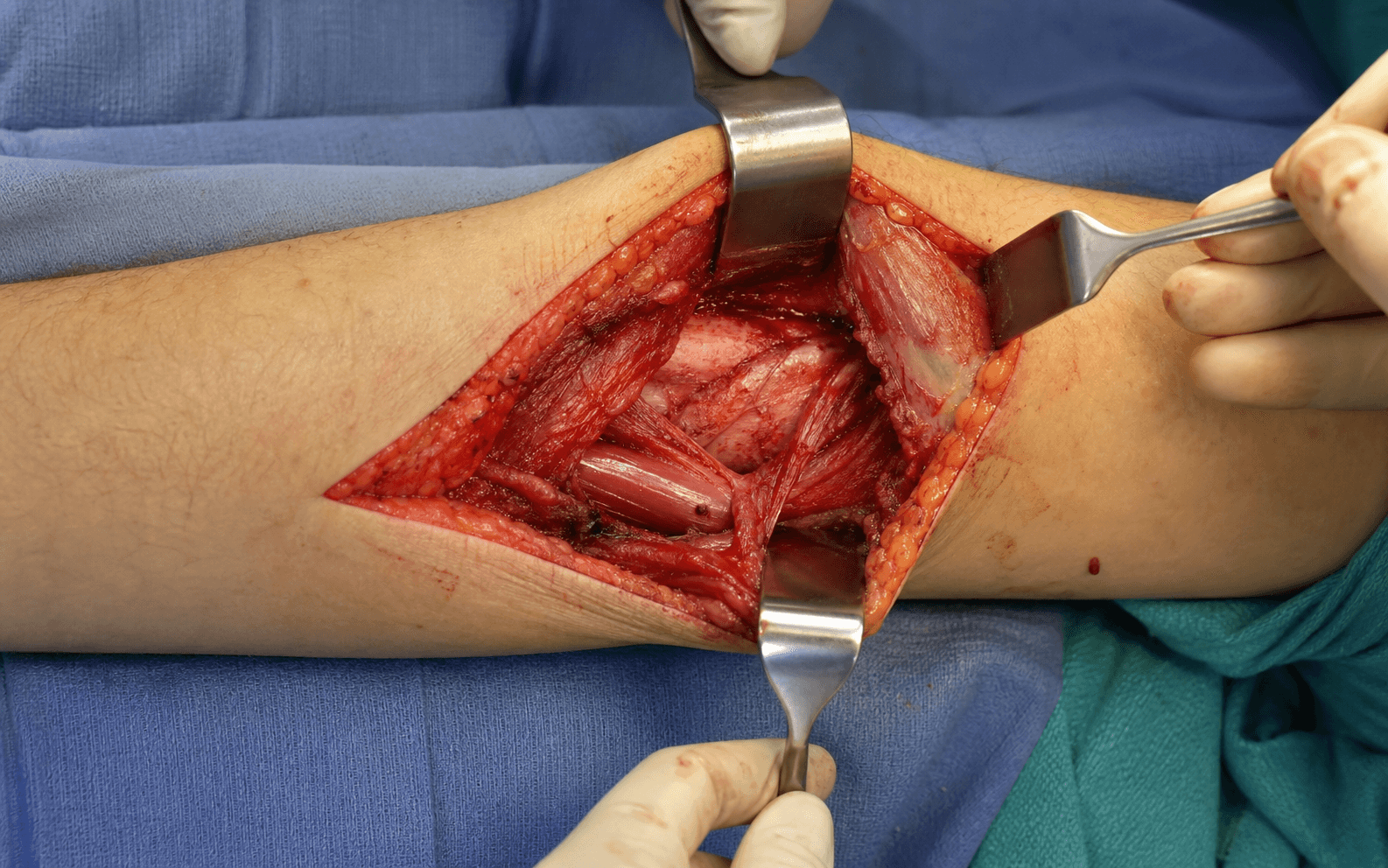
The Exposure
Work down through the layers along the subcutaneous ulnar border, develop the anconeus–ECU interval, then elevate the anconeus and supinator origin off the ulna as a single subperiosteal flap and reflect it radially — carrying the posterior interosseous nerve safely within the muscle mass. The internervous plane. The classical superficial interval lies between anconeus (radial nerve) and extensor carpi ulnaris (posterior interosseous nerve). The deep safety of the Boyd approach, however, does not come from internervous dissection: it comes from elevating the common origin of anconeus and supinator from the ulna as a single subperiosteal flap and reflecting it radially, with the posterior interosseous nerve carried within it.
- Muscle
- Anconeus
- Nerve supply
- Radial nerve
- Action
- Elbow extension; stabilises the joint
- Muscle
- Extensor carpi ulnaris
- Nerve supply
- Posterior interosseous nerve
- Action
- Wrist extension, ulnar deviation
- Muscle
- Supinator
- Nerve supply
- Posterior interosseous nerve
- Action
- Forearm supination
- Muscle
- Common extensor origin
- Nerve supply
- Radial nerve / PIN
- Action
- Wrist and finger extension
Exposure sequence
- A longitudinal incision along the subcutaneous border of the ulna, beginning 2 to 3 cm proximal to the olecranon tip if proximal extension is needed and running distally along the ulnar border as far as required (typically 8 to 12 cm).
- Centre the incision over the radial head for isolated radial head work; extend it for Monteggia or complex fractures.
- Incise the deep fascia in line with the skin incision.
- Identify the interval between anconeus (posterior) and extensor carpi ulnaris (anterior) in the soft spot distal to the lateral epicondyle, and develop it bluntly toward the olecranon.
- Begin subperiosteal elevation on the ulna at the level of the radial head.
- Elevate the origin of anconeus (proximally) and supinator (distally) as a single continuous flap from the lateral aspect of the proximal ulna. Stay strictly on bone.
- Reflect the entire anconeus–supinator flap radially en masse.
- The posterior interosseous nerve, which enters the supinator about 1 cm distal to the radial head, stays protected within the reflected muscle mass — it is never visualised or dissected.
- With the flap reflected, the radial head, radial neck, annular ligament and proximal radioulnar joint are exposed.
- The annular ligament can be incised anteriorly or posteriorly as needed for radial head access, preserving enough tissue for repair; the radial neck is visualised for fracture reduction or prosthetic stem placement.
The Boyd approach is safe precisely because the surgeon does not attempt to identify the posterior interosseous nerve. The subperiosteal ulnar flap keeps the nerve protected within the muscle mass — trying to find and dissect the nerve increases the risk of injury.
Posterior interosseous nerve injury occurs when the surgeon dissects within the supinator muscle rather than staying subperiosteal on the ulna. The Boyd flap technique avoids this by reflecting the entire muscle origin with the nerve inside it. The injury rate is less than 5 percent when the subperiosteal technique is followed.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Lateral cutaneous nerve of the forearm (sensory branches)
- Protection strategy
- Identify and protect the sensory branches during the skin incision
- Structure at risk
- Posterior interosseous nerve within the supinator (1 cm distal to the radial head)
- Protection strategy
- Subperiosteal ulnar flap — never dissect within the supinator
- Structure at risk
- Radial recurrent artery
- Protection strategy
- Ligate branches crossing the field if encountered
- Structure at risk
- Annular ligament
- Protection strategy
- Preserve or repair to maintain radial head stability
- Structure at risk
- Ulnar and radial periosteum
- Protection strategy
- Never strip from both bones — prevents radioulnar synostosis
Heterotopic ossification and radioulnar synostosis occur in up to 5 to 10 percent of cases if the interosseous membrane or periosteum is stripped from both the ulna and the radius, creating a bridge for bone formation. Prevent it with meticulous subperiosteal technique on the ulna only, avoidance of haematoma in the interosseous space, thorough irrigation to remove bone debris, and early mobilisation.
Extensile options and approach variants. The incision extends proximally along the lateral border of the triceps tendon to expose the olecranon and distal humerus, and distally along the subcutaneous ulnar border for ulnar shaft fixation in Monteggia injuries (elevating extensor carpi ulnaris subperiosteally as needed). Never cross the interosseous space to the radius at any level, to avoid synostosis.
- Description
- Subperiosteal anconeus–supinator flap from the ulna reflected radially
- Use
- Standard for most indications
- Description
- Proximal extension along the triceps for olecranon access
- Use
- Complex proximal fractures
- Description
- Along the ulnar border for shaft involvement
- Use
- Monteggia with ulnar comminution
Closure. Reattach the subperiosteal flap (the anconeus and supinator origin) to the ulna using heavy absorbable or non-absorbable sutures through drill holes or to the periosteal sleeve, then close the fascia over extensor carpi ulnaris and close the subcutaneous tissue and skin in layers. A drain is rarely required. Immobilise the elbow in 90 degrees of flexion and neutral rotation for 7 to 10 days if an annular ligament repair was performed; otherwise encourage early gentle motion.
Procedures Through This Approach
- Radial head arthroplasty — press-fit or cemented stems for comminuted Mason III or IV fractures.
- ORIF of radial head fractures — plate or headless screw fixation.
- Paediatric Monteggia fracture-dislocation — ulnar plate with radial head reduction.
- Annular ligament reconstruction or repair using a tendon graft.
- Open reduction of radial neck fractures in adults and children.
- Excision of the radial head (rarely indicated now).
Viva & Exam Focus
BOYD SAFEBOYD SAFE — the surgical steps
PIN SAFEPIN SAFE — protecting the nerve
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old falls from a height onto an outstretched hand and presents with a displaced proximal ulna fracture and radial head dislocation; CT confirms a Bado type I Monteggia injury. Describe your surgical approach and key steps.”
“A 48-year-old sustains a comminuted radial head fracture (Mason type III) after a fall. CT shows greater than three fragments with significant articular comminution. Discuss your choice of approach and key operative considerations for radial head arthroplasty.”
“A 29-year-old labourer undergoes a Boyd approach for a complex Monteggia injury with a radial head fracture. Six months later he has complete loss of forearm rotation and CT confirms radioulnar synostosis. What went wrong and how could it have been prevented?”
Positioning
- Lateral decubitus with arm on a padded bolster, or supine with arm across the chest
- Elbow flexed 90 degrees for C-arm access
- Tourniquet high on the arm; limit time to less than 120 minutes
- Prepare from axilla to wrist including the hand for rotation assessment
- Mark the olecranon, lateral epicondyle, radial head and ulnar border
Incision and landmarks
- Longitudinal along the subcutaneous ulnar border from the olecranon distally
- Centre over the radial head for isolated radial head work
- The anconeus triangle (olecranon–lateral epicondyle–radial head) is the key landmark
- The anconeus–ECU interval is found distal to the lateral epicondyle
- Extend proximally along the triceps if olecranon access is needed
Internervous plane and PIN protection
- Superficial interval: anconeus (radial n.) and ECU (PIN)
- Deep safety: subperiosteal elevation of the anconeus–supinator origin as a SINGLE flap
- Reflect the flap radially — the PIN stays inside the supinator within the flap
- NEVER dissect within the supinator muscle itself
- Document finger and wrist extension pre- and post-operatively
Danger structures
- PIN: protected by the subperiosteal flap technique (injury less than 5 percent)
- Radial recurrent artery: ligate branches crossing the field
- Lateral cutaneous nerve of the forearm: protect the sensory branches superficially
- Annular ligament: preserve or repair for radial head stability
- Interosseous membrane and periosteum: never strip from both bones
Procedures and closure
- Monteggia fixation: ulnar plate first, then radial head reduction
- Radial head arthroplasty: correct height restores radiocapitellar contact
- Annular ligament repair: critical for stability after radial head work
- Reattach the flap with heavy sutures through drill holes or the periosteal sleeve
- Immobilise 7 to 10 days if a ligament repair was performed, otherwise early motion
Complications
- PIN injury (less than 5 percent with correct technique) — most recover
- Radioulnar synostosis (5 to 10 percent) — devastating loss of rotation
- Infection (2 to 5 percent) — higher with open injuries or soft tissue compromise
- Radial head prosthesis complications: loosening, overstuffing, capitellar erosion
- Stiffness and heterotopic ossification — early motion and HO prophylaxis in high-risk patients
References
Surgical Treatment of Monteggia-Like Lesions With a Modified Boyd Approach
- Modified Boyd approach provides safe extensile exposure for Monteggia-like lesions with radial head involvement
- The subperiosteal ulnar flap technique effectively protects the posterior interosseous nerve
The Boyd approach: a valuable alternative to treating simple to complex elbow fractures and dislocations
- The Boyd approach offers reliable exposure across a spectrum of elbow trauma including the proximal radius and ulna
- Low complication profile when strict subperiosteal technique is followed for PIN protection
Posterior (Boyd) approach to terrible triad injuries
- The Boyd approach enables simultaneous access to the radial head, coronoid and lateral collateral ligament complex
- Meticulous PIN protection via subperiosteal reflection is essential in terrible triad reconstruction
The Boyd Interval: A Modification for Use in the Management of Elbow Trauma
- The Boyd interval modification enhances safety and exposure in elbow trauma surgery
- It preserves the core principle of the subperiosteal ulnar flap for posterior interosseous nerve protection