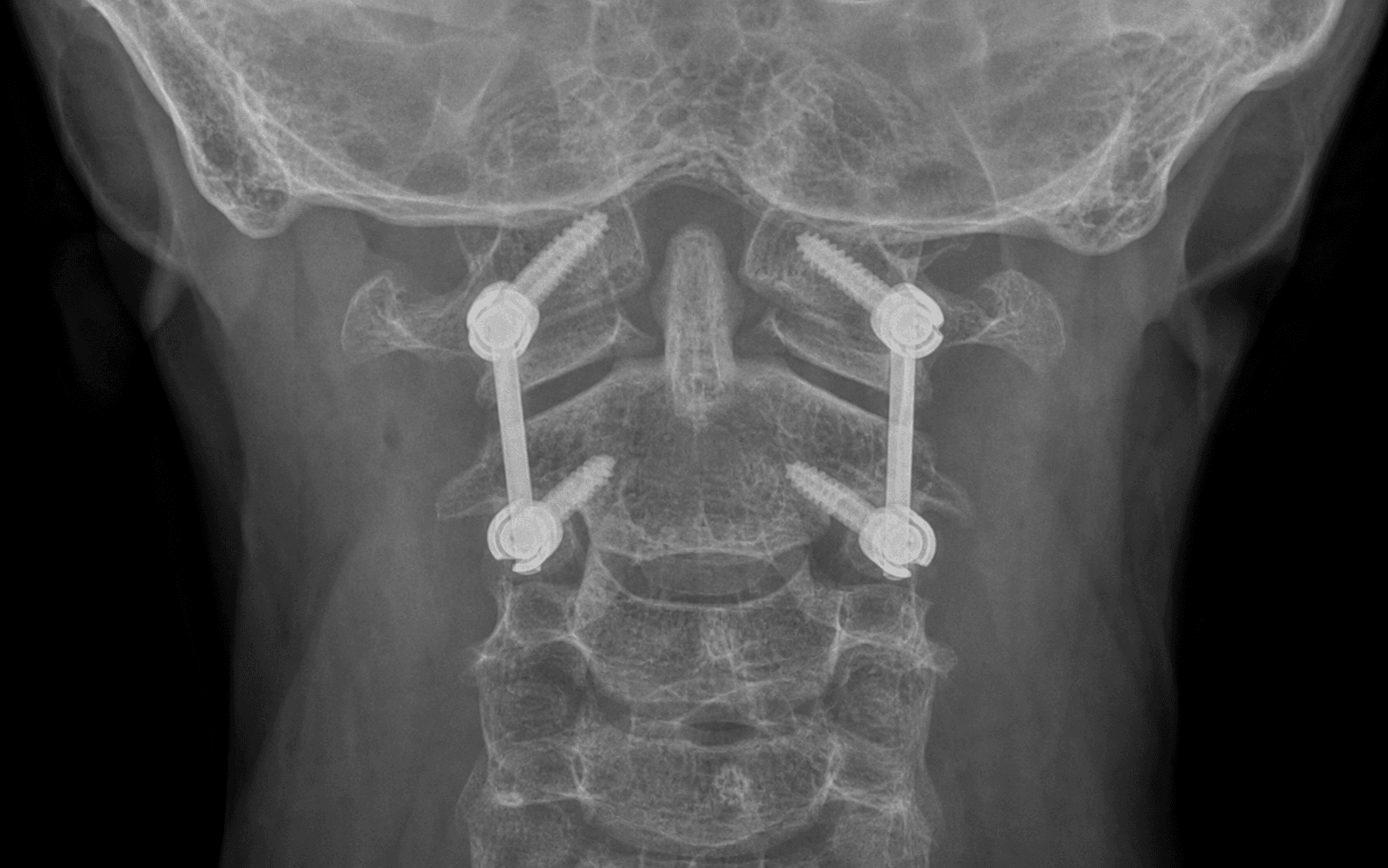
Posterior midline approach C1-C2 with the Harms technique: C1 lateral mass screws plus C2 pedicle or pars screws linked by rods, with facet-joint compression
- Atlantoaxial instability from a Type II odontoid fracture non-union, traumatic transverse atlantal ligament rupture, rheumatoid pannus, os odontoideum or Down syndrome produces an anterior atlantodental interval (ADI) greater than 3 mm in adults and warrants rigid C1-C2 fixation.
- The Harms technique (2001) pairs C1 lateral mass screws (20-28 mm, 10-15° medial, bicortical) with C2 pedicle screws (22-28 mm, 20-30° medial, 15-25° cephalad toward the odontoid tip) joined by rods with compression across the C1-C2 facets. Goel described the same construct independently in 1994.
- The vertebral artery lies only 2-3 mm lateral to the C1 lateral mass screw trajectory (in its groove on the superior C1 arch) and lateral to the C2 pedicle in the transverse foramen. A preoperative CT angiogram is mandatory — anomalies are present in 18-20% of patients.
- C1-C2 fusion permanently eliminates about 50% of total cervical rotation. Counsel the patient preoperatively that they will not be able to turn the head fully to check blind spots when driving.
- If the C2 pedicle is less than 3 mm wide or a high-riding vertebral artery is present, use C2 translaminar screws (Wright technique): they cross the midline within the lamina, avoid the vertebral artery entirely, and give equivalent biomechanics.
When & Why
Indication. Symptomatic atlantoaxial (C1-C2) instability that has failed or is unsuitable for non-operative care, demonstrated by an abnormal ADI (greater than 3 mm in adults, greater than 5 mm in children), cord compression, or a clearly unstable injury. The common pathologies are: - Traumatic: Type II odontoid fracture non-union (after 6 months of failed healing, or in the elderly with poor bone quality unsuitable for an anterior odontoid screw), Type III odontoid fracture with C2 body comminution, irreducible atlantoaxial rotatory subluxation, transverse ligament rupture (ADI greater than 5 mm indicates ligament incompetence), and Jefferson (C1 burst) fracture with transverse ligament disruption and instability.
- Rheumatoid arthritis: pannus erosion of the odontoid or transverse ligament with an ADI greater than 9 mm (cord compression risk), basilar invagination from bone erosion, and atlantoaxial subluxation with myelopathy.
- Congenital: os odontoideum with instability (a separate ossicle detached from the C2 body), Down syndrome atlantoaxial instability from ligamentous laxity (ADI greater than 5 mm), and Morquio syndrome (mucopolysaccharidosis).
- Degenerative / other: atlantoaxial osteoarthritis with instability (rare), chronic irreducible rotatory subluxation, tumour destroying C1-C2 (primary or metastatic) requiring reconstruction, and infectious instability such as Grisel syndrome in children. Contraindications. Absolute: an irreducible atlantoaxial dislocation (needs anterior transoral odontoidectomy or occiput-C2 fusion first), severe osteoporosis preventing screw purchase (T-score less than -4.0), and active infection at C1-C2 until treated. Relative: a C2 pedicle less than 3 mm wide (use translaminar screws), a vertebral artery anomaly precluding safe pedicle screws (use translaminar), a previous failed C1-C2 fusion requiring revision, or a young patient who cannot accept the loss of 50% of cervical rotation. The one decision that matters — which C2 screw. Every Harms-Goel fusion begins with the same C1 lateral mass screws; the real choice is the C2 fixation, dictated by the preoperative CT:
Strongest fixation (600-800 N pullout), best biomechanics, and lets you reduce C1-C2 using the screws as joysticks. The default when the pedicle is at least 3 mm wide and there is no vertebral artery anomaly.
Wright technique: the screw enters lateral on the lamina and crosses the midline within it (30-35 mm). Completely avoids the vertebral artery. Equivalent biomechanics (550-700 N) and fusion. Use when the pedicle is less than 3 mm or a high-riding vertebral artery is present — needs an intact lamina.
Gallie or Brooks wiring (85-90% fusion, needs a halo for 3 months) or Magerl transarticular screws (4-8% vertebral artery risk, not feasible bilaterally in 20%). Reserved for osteoporosis/salvage or rare selected cases — not the modern default.
Consent specifically for the permanent loss of about 50% of cervical rotation (difficulty driving, checking blind spots, and rotation sports), likely occipital numbness if the C2 nerve is sacrificed, a 1-2% risk of an airway-threatening haematoma, a 2-4% vertebral artery injury risk with a small chance of posterior circulation stroke, and 8-12 weeks in a hard collar. Setup. Prone on a radiolucent Jackson table or chest rolls with Mayfield 3-pin head fixation. Biplanar fluoroscopy and SSEP/MEP neuromonitoring are essential throughout. Plan 150 minutes of anaesthetic time.
The Operation
The goal is to stabilise a reducible atlantoaxial instability by placing independent C1 lateral mass and C2 pedicle screws, link them with rods, compress across the C1-C2 facets, decorticate and graft those facets, and confirm reduction on imaging — all while protecting the vertebral artery, the spinal cord and the venous plexus. The exposure and screw trajectories below are the heart of the operation.
Operative sequence
- A CT angiogram of the cervical spine from skull base to C7 is mandatory. On multiplanar reconstructions measure the C2 pedicle width (need at least 3 mm for a safe 3.5 mm screw), height, medial convergence (typically 20-30°) and cephalad angle (15-25°).
- Identify vertebral artery anomalies (18-20%): a high-riding vertebral artery coursing through the C2 pedicle (an absolute contraindication to a pedicle screw — plan translaminar), fenestration (2-3%), a persistent first intersegmental artery (1-2%), and a dominant vertebral artery with the contralateral side less than 2 mm (10%).
- Review the MRI for reducibility on flexion views and for cord compression from pannus, tumour or haematoma. If the ADI stays greater than 5 mm in flexion the dislocation is irreducible and may need anterior decompression or an occiput-C2 fusion.
- Apply the Mayfield 3-pin clamp supine: two pins posterolateral above the ears in the temporoparietal region (avoid the temporalis muscle anteriorly), one pin on the midline forehead 1-2 cm above the eyebrow (avoid the frontal sinus and sagittal sinus). Pin pressure 60-80 lbs in normal bone, reduced to 40-60 lbs in the osteoporotic elderly or children.
- Turn prone, then position the head in neutral to slight flexion (5-10°). This is the reduction manoeuvre: flexion translates C1 posteriorly relative to C2 and closes the ADI. Avoid extension, which worsens anterior subluxation and compresses the cord.
- Confirm reduction on the lateral C-arm before draping: the ADI should be less than 3 mm (ideal) and must be less than 5 mm. Tape the shoulders inferiorly so C3 is visible on lateral fluoroscopy; apply 15-20° reverse Trendelenburg to reduce venous congestion. Obtain baseline SSEPs and MEPs.
- Palpate the inion and the large bifid C2 spinous process. Mark a midline incision about 8-10 cm from just below the inion to C3, and infiltrate with local anaesthetic and epinephrine 1:200,000.
- Incise skin and subcutaneous tissue, identify the ligamentum nuchae, and divide it in the avascular midline plane — this is the key to minimising bleeding.
- Perform subperiosteal dissection with a Cobb elevator, staying directly on bone: expose the C1 posterior arch (a thin arc, 3-5 mm thick, with no spinous process — only a small posterior tubercle in the midline) and the C1 lateral masses (the rectangular thickening, 15-20 mm thick, where the arch meets the lateral mass, 15-20 mm lateral to the midline). Expose inferiorly onto the C2 lamina and large bifid spinous process, and laterally onto the C2 pars.
- Expect significant venous bleeding from the dense suboccipital venous plexus over the C1 arch and facets — control it with bipolar cautery, thrombin-soaked Gelfoam and patience. Meticulous exposure here (20-30 minutes) is what makes the screw placement safe.
- The large C2 ganglion (8-10 mm) sits directly on the superior surface of the C2 pedicle/pars, covering the screw entry point. Decide whether to retract or sacrifice it.
- Sacrifice (unilateral or bilateral) gives excellent, safe exposure; it causes expected ipsilateral posterior-scalp numbness with 20-30% temporary dysesthesias, less than 5% chronic significant pain, no motor deficit, and 92% patient satisfaction (Hott 2004). Attempting retraction instead carries a 30-40% traction-injury rate with similar or worse dysesthesias (Yeom 2008).
- Most surgeons sacrifice the C2 nerve (at least unilaterally) for safe drilling, having counselled the patient preoperatively about the expected numbness.
- Entry: at the junction of the C1 posterior arch and lateral mass, 1-2 mm medial to the lateral edge, about 15-20 mm from the midline. Stay off the superior surface of the arch (that is the vertebral artery groove).
- Trajectory: 10-15° medial toward the anterior tubercle, 0-10° cephalad. Drill 20-28 mm under lateral fluoroscopy aiming at the anterior tubercle, with a depth stop at 28 mm.
- Probe all four walls — the lateral wall is critical (the vertebral artery is 2-3 mm lateral). Any soft tissue laterally means a breach: abort that side. Insert a 3.5 mm screw, 24-30 mm, bicortical (300-400 N pullout versus 200 N unicortical). Confirm on biplanar fluoroscopy and repeat for the contralateral side.
- Entry: medial and high — the medial-superior quadrant of the C2 superior facet-lamina junction, 3-5 mm from the midline, 3 mm superior to the inferior laminar border.
- Trajectory: 20-30° medial toward the odontoid tip and 15-25° cephalad parallel to the C2 superior endplate, drilling 20-28 mm. This narrow corridor (4-8 mm) runs between the spinal canal medially and the vertebral artery foramen laterally.
- Drill under biplanar fluoroscopy simultaneously: on AP the screw must converge toward the odontoid; on lateral it must parallel the superior endplate. Advance 1-2 mm at a time. Probe the medial wall (breach equals canal) and lateral wall (breach equals vertebral artery). Insert a 3.5 mm screw, 22-28 mm, bicortical (600-800 N pullout).
- Alternative: if the pedicle is less than 3 mm or the vertebral artery is high-riding, use a C2 translaminar screw — entry 5-8 mm from the midline on the lamina, crossing the midline within the lamina at 15-20°, 30-35 mm long, parallel to the inferior endplate. It avoids the vertebral artery entirely (0% injury versus 4% for pedicle, Wright 2004) with equivalent fusion (96-97%).
- Verify the reduction on lateral fluoroscopy before rod placement — the ADI should be less than 3 mm. If subluxation persists, use the screw tulips as joysticks to compress, distract or translate C1-C2 into reduction (a major advantage of the Harms technique over transarticular screws, which require perfect reduction before insertion).
- Measure the rod length between the C1 and C2 tulips (typically 25-35 mm). Contour a 3.5 mm cervical rod to a slight lordosis matching the natural C1-C2 alignment, with smooth bends and no sharp stress-risers.
- Seat the pre-contoured rod into the C1 tulip first, then press it down into the C2 tulip using a persuader. Provisionally tighten the set screws finger-tight and repeat for the contralateral rod.
- Apply compression across C1-C2 (3-5 mm), watching lateral fluoroscopy — this closes the facet joints where fusion occurs and reduces any residual subluxation. Finally tighten all four set screws to manufacturer torque (typically 4-6 Nm). The construct should feel rigid with no motion.
- Fusion is the real goal — hardware alone eventually fatigues and fails. The primary fusion site is the C1-C2 facet joints: curette and burr away all articular cartilage from both the C1 inferior and C2 superior facets until bleeding cancellous bone shows.
- Decorticate the posterior surface of the C1 arch (without over-thinning it) and the C2 lamina with the burr.
- Pack morselised graft generously into the facet joints and over the posterior elements (about 10-15 cc total). Local autograft from the C2 spinous process or allograft works well (autograft 95% versus allograft 88% fusion with rigid fixation). Avoid BMP at C1-C2 — it is off-label here and risks soft-tissue swelling, dysphagia and airway compromise.
- Obtain final biplanar fluoroscopy and save it to PACS. On AP, the screws should converge medially as expected; on lateral, the ADI should be less than 3 mm, C1 screws parallel to the superior arch (not in the vertebral artery groove), C2 screws parallel to the superior endplate, and the rods connecting smoothly.
- Achieve meticulous haemostasis — a cervical haematoma causes airway obstruction. Copious irrigation, bipolar to all bleeders, thrombin-Gelfoam over the facets, bone wax for bony ooze, and a Valsalva to 30-40 cm H2O to expose venous bleeding. Release the Mayfield and check the pin sites.
- Place a subfascial Blake or Jackson-Pratt drain (10-12 Fr) over the hardware, exiting laterally through a separate stab. Close the ligamentum nuchae and midline raphe with heavy absorbable suture (the structural layer), then close in layers and apply a sterile dressing.
- Apply a hard cervical collar (Philadelphia or Miami-J) before turning the patient supine. Transfer to an ICU or monitored bed: watch the airway closely for the first 24 hours (C1-C2 haematoma risk is higher than subaxial because of pharyngeal proximity), perform an immediate wake-up neurological exam, repeat neuro checks every 2 hours, and remove the drain when output is less than 30 mL per 24 hours.
A preoperative CT angiogram is mandatory: it drops the vertebral artery injury rate from 10-12% (no CTA) to 2-4%. Place the C1 screw 10-15° medial and the C2 screw 20-30° medial toward the odontoid tip, use biplanar fluoroscopy, and probe the lateral wall after every drill pass. If brisk bright-red pulsatile bleeding occurs during screw work, do not remove the screw (it may be tamponading the artery) — pack tightly, call vascular surgery, and consider endovascular balloon occlusion. A unilateral injury is tolerated in about 70% of patients; a bilateral injury is catastrophic (30% fatal).
The C2 pedicle is the highest-risk step — a narrow 4-8 mm corridor between the canal medially and the vertebral artery laterally. Watch AP and lateral fluoroscopy simultaneously: on AP the drill must converge toward the odontoid (a lateral trajectory is heading for the artery); on lateral it must parallel the superior endplate. Drill 1-2 mm at a time and probe both walls before tapping.
If the preoperative CT shows a C2 pedicle less than 3 mm wide or a high-riding vertebral artery, do not force a pedicle screw (20-30% breach rate). Switch to a C2 translaminar screw (Wright 2004): it crosses the midline within the lamina, completely avoids the vertebral artery, and gives equivalent biomechanics and fusion (96-97%) — it only needs an intact lamina.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Activity | |-------|--------|----------------|----------| | 1 | 0-24 h | Hard collar on in theatre; ICU airway monitoring | Bed to chair day 1 if neurologically intact | | 2 | Days 1-7 | Hard collar 24/7 | Ambulate day 1-2 with therapy; soft diet (10-20% transient dysphagia); DVT prophylaxis; discharge day 2-4 | | 3 | Weeks 2-6 | Hard collar 24/7 | Remove staples week 2; upright lateral X-ray in collar at week 6 | | 4 | Weeks 8-12 | Wean collar if flexion-extension films stable | Desk work from 6-8 weeks (possible in collar) | | 5 | Months 6-12 | Off collar once CT confirms fusion | Driving after collar off and fusion stable; heavy labour after CT fusion | A hard collar (Philadelphia or Miami-J) is worn continuously for 8-12 weeks — longer than subaxial fusions (typically 6 weeks) because the biomechanical stress at C1-C2 is high. Driving is not allowed in a collar and only resumes once the collar is discontinued and the fusion is stable; counsel the patient about the permanent 50% rotation loss (they must adjust mirrors and turn the whole body to check blind spots). Contact sports are generally discontinued permanently. About 80-85% achieve good-to-excellent pain relief when instability was the pain source (Grob 1992). Complications
- Incidence
- 2-4% (screw-rod); 4-8% (transarticular, Madawi 1997)
- Recognition
- Bright red pulsatile bleeding from the screw hole; posterior-circulation stroke (ataxia, vertigo, diplopia) within 24-72 h
- Prevention
- Mandatory preoperative CTA; biplanar fluoroscopy; correct medial trajectory; probe the lateral wall; translaminar screws for a narrow pedicle or high-riding VA
- Management
- Do NOT remove the screw (tamponade); pack tightly; vascular surgery; endovascular balloon occlusion. Unilateral 70% asymptomatic; bilateral 30% fatal
- Incidence
- less than 1%
- Recognition
- Intraoperative MEP loss greater than 50%; immediate postoperative motor deficit at a C2-C3 level
- Prevention
- Preoperative pedicle measurement (abort if less than 3 mm); biplanar fluoroscopy; 20-30° medial trajectory toward the odontoid; probe the medial wall
- Management
- Stop, remove the screw if breach confirmed, urgent MRI, consider decompression; high-dose steroids controversial
- Incidence
- 1-2% (higher than subaxial)
- Recognition
- First 24 h: stridor, dyspnea, dysphagia, tense neck swelling
- Prevention
- Meticulous hemostasis and a Valsalva; subfascial drain; ICU monitoring first 24 h
- Management
- Anaesthesia STAT; open the wound at the bedside to evacuate; return to theatre for formal haemostasis; keep intubated 24-48 h
- Incidence
- 20-30% temporary dysesthesias; less than 5% chronic
- Recognition
- Numbness of the posterior scalp in the greater occipital nerve distribution; tender Tinel; triggered by touch
- Prevention
- Counsel preoperatively about expected numbness; planned sacrifice is safer than aggressive retraction (30-40% traction injury)
- Management
- Reassure (70-80% settle in 6-12 months); gabapentin, amitriptyline, topical lidocaine; refractory cases — occipital nerve blocks, neurectomy or stimulation
- Incidence
- 5-15% cortical breach on CT; 21% of C2 pedicle screws violate the VA groove (Yeom 2008)
- Recognition
- Abnormal trajectory on fluoro; soft tissue on probing; most breaches asymptomatic (less than 3% symptomatic)
- Prevention
- Biplanar fluoroscopy; probe all four walls; low threshold for postoperative CT (fluoroscopy only 60-70% sensitive)
- Management
- Observe if asymptomatic and stable; revise if VA or cord compression (re-drill or switch to translaminar)
- Incidence
- 2-5% (screw-rod); 10-15% (wiring)
- Recognition
- Persistent neck pain 6-12 months; greater than 2 mm translation or greater than 5° motion on flexion-extension films; no bridging bone on CT
- Prevention
- Complete facet decortication; generous graft (10-15 cc); rigid compression fixation; smoking cessation; collar compliance
- Management
- Revision fusion — repeat decortication, iliac-crest autograft, new construct, extend to occiput-C3 if bone quality poor
- Incidence
- 2-5%
- Recognition
- Crack during screw insertion; sudden loss of purchase; fracture line on CT
- Prevention
- Gentle hand-tightening; avoid over-tightening on the thin 3-5 mm arch; bicortical purchase distributes force
- Management
- Abandon the fractured screw; use the contralateral C1 screw plus bilateral C2, or an alternative (occiput-C2, C1 hooks/cable)
- Incidence
- Permanent — about 50% of total rotation
- Recognition
- Cannot turn the head fully to check blind spots when driving; head turns only about 40° versus 80-90°
- Prevention
- Cannot prevent — preoperative counselling is the management
- Management
- Teach compensatory strategies (turn the whole body, adjust mirrors); most adapt well over 3-6 months
Viva & Exam Focus
HARMSHARMS — the Harms-Goel technique
VA-SAFEVA-SAFE — protecting the vertebral artery
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Why is the Harms technique superior to older methods like Gallie or Brooks wiring, and when might you still use wiring?”
“You get brisk bleeding during C1 or C2 screw insertion. How do you tell vertebral artery from venous plexus bleeding, and what do you do?”
“A patient has a C2 pedicle width of 2.5 mm on preoperative CT. What are your options, and how do you decide?”
Indications
- Type II odontoid non-union (after 6 months or unsuitable for anterior screw in the elderly)
- Transverse ligament rupture (ADI greater than 5 mm); Jefferson C1 burst with TAL disruption
- Rheumatoid pannus with ADI greater than 9 mm, basilar invagination, or myelopathy
- Os odontoideum, Down syndrome (ADI greater than 5 mm), Morquio
- Tumour or infection destroying C1-C2 with instability
Key anatomy
- C1 lateral mass: 15-20 mm thick at the arch-lateral mass junction; screw entry 1-2 mm medial to the lateral edge, 15-20 mm from the midline
- C1 screw: 10-15° medial toward the anterior tubercle, 0-10° cephalad, 20-28 mm bicortical (VA 2-3 mm lateral)
- C2 pedicle: 4-8 mm wide (18% less than 3 mm), entry medial-superior quadrant 3-5 mm from the midline
- C2 screw: 20-30° medial toward the odontoid tip, 15-25° cephalad, 20-28 mm
- VA: 2-3 mm lateral to the C1 lateral mass in the groove on the superior arch; anomalies in 18-20%
- C2 ganglion (8-10 mm) on the superior surface of the C2 pedicle obscures the entry point
Critical steps
- Preoperative CTA mandatory: pedicle width (translaminar if less than 3 mm), VA anomalies (18-20%), reducibility on flexion MRI
- Mayfield in slight flexion (5-10°) reduces most subluxations — confirm ADI less than 3 mm on lateral fluoro before draping
- Midline subperiosteal exposure to the C1 arch, lateral masses and C2 pars; control the venous plexus patiently
- C1 lateral mass screw: probe the lateral wall (VA); bicortical 3.5 mm by 24-30 mm
- C2 pedicle screw: biplanar fluoro simultaneously, probe medial (canal) and lateral (VA) walls; 3.5 mm by 22-28 mm
- Rods in slight lordosis; compress 3-5 mm to close the facets; torque 4-6 Nm
- Decorticate the C1-C2 facets completely and pack 10-15 cc graft (primary fusion site)
Danger zones
- Vertebral artery (2-3 mm lateral to C1 lateral mass; lateral to C2 pedicle): injury 2-4%; leave screw in, pack, vascular, endovascular occlusion
- Spinal cord (8-10 mm from the C2 medial wall): injury less than 1%; proper medial trajectory and biplanar fluoro
- C2 nerve root and ganglion: sacrifice for exposure (expected occipital numbness); stay within 15 mm of the midline to avoid the greater occipital nerve
- Internal carotid (15-20 mm anterior to the C1 anterior tubercle): rare (less than 0.5%); depth stop at 28 mm
- Venous plexus: expect 100-300 mL; control with bipolar and Gelfoam; inadequate haemostasis causes airway-threatening haematoma
Technique pearls
- Harms (2001) and Goel (1994) independently described identical constructs — the modern gold standard at approx. 97% fusion
- C2 pedicle less than 3 mm: use C2 translaminar screws (0% VA injury versus 2-4%, equivalent fusion)
- Bicortical C1 purchase gives 300-400 N pullout versus 200 N unicortical
- Compression at the facets is the critical step for fusion
- Slight flexion reduces most subluxations — advantage over techniques needing pre-fixation reduction
- Sacrifice the C2 nerve for safer exposure (92% satisfaction) rather than risk traction injury
- A drain is mandatory — haematoma causes airway obstruction at C1-C2
- Avoid BMP at C1-C2 — risk of soft-tissue swelling and airway compromise
Post-op protocol
- ICU first 24 h: airway watch, neuro checks every 2 h for posterior-circulation stroke
- Subfascial drain 10-12 Fr; remove when less than 30 mL per 24 h; do not leave more than 48 h
- Hard collar (Philadelphia or Miami-J) 24/7 for 8-12 weeks (longer than subaxial)
- Mobilise day 1; soft diet (10-20% transient dysphagia); DVT prophylaxis; discharge day 2-4
- Week 2 wound check; week 6 upright lateral X-ray; week 8-12 flexion-extension films to wean collar
- CT at 6-12 months confirms fusion (bridging bone across both C1-C2 facets)
- Counsel: permanent 50% rotation loss; desk work 6-8 weeks; driving only after collar off and fusion stable
Background & Evidence
Historical evolution. Atlantoaxial fixation has progressed through four generations. Gallie wiring (1939) passed a sublaminar wire under the C1 arch and over the C2 spinous process with graft between — a posterior tension band giving flexion stability only, with 85-90% fusion and a 3-month halo. Brooks wiring (1978) added bilateral sublaminar wires for better rotational control but similar fusion. Magerl transarticular screws (1987) crossed the C1-C2 facet into the C1 lateral mass with excellent biomechanics, but the vertebral artery overlies the trajectory in 18-20%, so bilateral screws cannot be placed safely in 20%, and perfect reduction is required before screw insertion. The Harms technique (2001) — C1 lateral mass plus C2 pedicle screws linked by rods — became the gold standard because it allows reduction after screw insertion, is safer for the vertebral artery, and is feasible in 98% of patients. Goel (1994) described the same segmental construct independently and earlier; the two are now called the Harms-Goel technique. Why it works: pathoanatomy. The atlas is a ring without a vertebral body; its lateral masses (15-20 mm thick at the arch junction) are the screw target, and the vertebral artery runs in a groove on the superior surface of the posterior arch only 2-3 mm lateral to that target. The axis carries the odontoid; its pedicle (pars/isthmus — the same structure) is a narrow 4-8 mm corridor between the spinal canal medially and the transverse foramen laterally. The transverse atlantal ligament (TAL) is the prime C1-C2 stabiliser — its rupture or an odontoid fracture allows anterior C1-on-C2 translation, measured by the ADI (normal less than 3 mm adults, less than 5 mm children; greater than 5 mm means TAL incompetence; greater than 9 mm in rheumatoid disease risks cord compression). Fusing C1-C2 sacrifices the 40-50° of rotation each way that the C1-C2 articulation contributes — half of all cervical rotation — while preserving occiput-C1 motion (15° flexion-extension, 5° rotation).
- Pullout strength
- 700-900 N
- VA injury rate
- 4-8%
- Notes
- Cannot place bilaterally in 20%; needs perfect reduction before insertion
- Pullout strength
- 600-800 N
- VA injury rate
- 2-4%
- Notes
- Standard; allows reduction with screws as joysticks
- Pullout strength
- 550-700 N
- VA injury rate
- 0-1%
- Notes
- Avoids VA entirely; equivalent fusion; needs intact lamina
- Pullout strength
- 200-300 N
- VA injury rate
- 0%
- Notes
- Weaker; osteoporosis or supplement only
- Pullout strength
- 300-400 N
- VA injury rate
- 2-4%
- Notes
- VA 2-3 mm lateral; probe the lateral wall
- Pullout strength
- 150-250 N
- VA injury rate
- —
- Notes
- Sublaminar wire, cord risk; 85-90% fusion; halo 3 months
Fusion rates and biomechanics. In the pooled Elliott meta-analysis (2012), screw-rod constructs fused in about 97% (97.4% with bracing versus 97.9% without — no significant benefit from a postoperative collar), against 94-95% for transarticular screws. The Harms construct reduces flexion-extension motion by 95% and rotation by 88% (Melcher 2002; Gorek 2005), versus 65%/55% for Gallie wiring. Intraoperative fluoroscopy materially under-detects vertebral artery violations: Yeom (2008) found 21% of C2 pedicle screws caused vertebral artery groove violations on postoperative CT and one C1 screw caused arterial occlusion — none detected intraoperatively or on plain films — which is why a low threshold for postoperative CT is advised. Vertebral artery anatomy is the whole game. Anomalies are common and significantly more so in atlantoaxial instability: a high-riding vertebral artery (present in about 20% of CT scans, and narrowing the mean C2 pedicle width to only 2.53 mm versus 5.83 mm in controls, Kothari 2019), fenestration (2-3%), a persistent first intersegmental artery (1-2%), and a dominant vertebral artery (10%). Byun (2022) confirmed these anomalies are significantly more frequent in patients with atlantoaxial instability, with a correspondingly narrower C2 safe zone — reinforcing the rule of a mandatory preoperative CT angiogram before any screw-rod fixation.
References
Posterior C1-C2 fusion with polyaxial screw and rod fixation
- Original description of the screw-rod technique: bilateral 3.5 mm polyaxial screws in the C1 lateral mass and through the C2 pars into the pedicle, connected by rods after fluoroscopic reduction
- 37 patients treated; solid fusion in all on early clinical and radiographic follow-up with no neural or vascular damage related to the technique
- Independent C1 and C2 fixation allows reduction by manipulating the implants AFTER screw insertion — usable even when fixed subluxation or aberrant vertebral artery precludes transarticular screws
Plate and screw fixation for atlanto-axial subluxation
- 30 cases of atlanto-axial dislocation treated with lateral mass plate-and-screw fixation of the atlas and axis, achieving 100% union with no morbidity, mortality, or instrument failure
- Direct screw purchase in the thick corticocancellous C1 and C2 lateral masses provides immediate rigid segmental fixation, permitting early mobilisation with minimal external support
- Described independently of and before Harms, establishing the conceptual basis of the Goel-Harms technique
Posterior C2 fixation using bilateral, crossing C2 laminar screws: case series and technical note
- Anatomic variability of the C2 transverse foramen precludes safe transarticular or pedicle screw placement in up to 20% of patients, placing the vertebral artery at risk
- Bilateral crossing C2 translaminar screws capture the axis without placing the vertebral artery at risk — the screw stays within the lamina, lateral to the canal and medial to the artery
- Successfully used in trauma, neoplasm, pseudarthrosis and degenerative disease as part of atlantoaxial and craniocervical constructs
Undetected vertebral artery groove and foramen violations during C1 lateral mass and C2 pedicle screw placement
- Postoperative thin-cut CT and CT angiography of 85 screws (39 C1 lateral mass, 39 C2 pedicle, 7 C2 laminar) placed under fluoroscopy
- 8 of 39 C2 pedicle screws (21%) caused vertebral artery groove violations and 1 C1 screw breached the foramen causing arterial occlusion on CTA
- NONE of the violations — including the arterial occlusion — were detected intraoperatively or on plain radiographs
Is external cervical orthotic bracing necessary after posterior atlantoaxial fusion with modern instrumentation: meta-analysis and review of literature
- Pooled 947 screw-rod construct patients (18 studies) and 1424 transarticular screw patients (33 studies)
- Fusion rates: screw-rod 97.4% with bracing versus 97.9% without; transarticular 93.6% with bracing versus 95.3% without — screw-rod constructs achieve the highest fusion rates
- No significant difference in fusion with versus without a postoperative external cervical orthosis, and no dose effect of brace duration
The C2 pedicle width, pars length, and laminar thickness in concurrent ipsilateral ponticulus posticus and high-riding vertebral artery: a radiological CT study
- High-riding vertebral artery present in about 20% of CT scans
- With a concurrent ponticulus posticus and high-riding VA the mean C2 pedicle width was only 2.53 mm versus 5.83 mm in controls, while laminar thickness remained safe (4.92 mm)
- Supports C2 translaminar screws when the pedicle is narrow and a high-riding VA is present
The association between atlantoaxial instability and anomalies of the vertebral artery and axis
- Vertebral artery anomalies and high-riding vertebral arteries are significantly more common in patients with atlantoaxial instability
- The C2 safe zone is correspondingly narrower in these patients
- Reinforces the need for mandatory preoperative CT angiography before screw-rod fixation