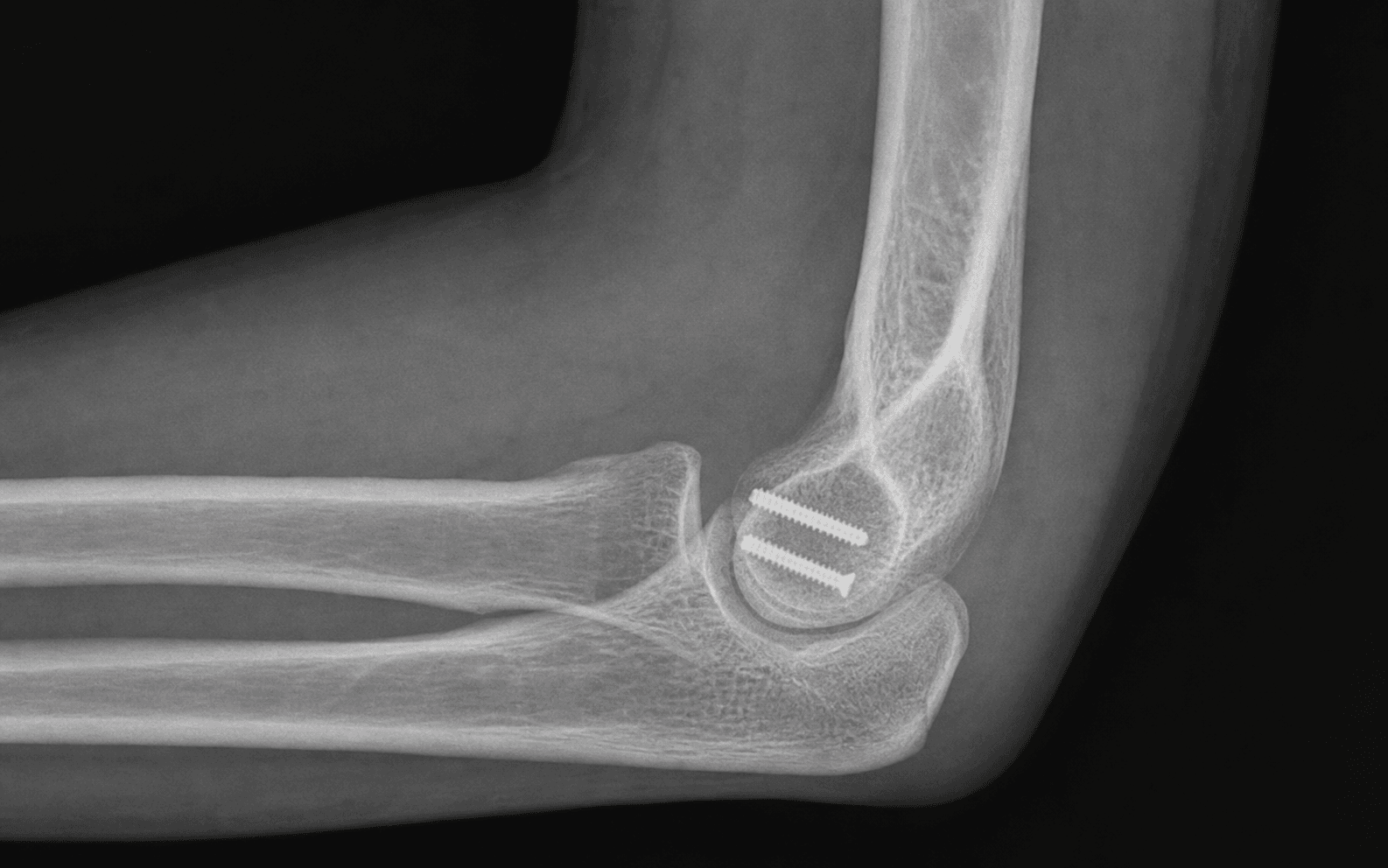
Lateral approach ORIF with headless compression screws for displaced capitellar and coronal shear fractures of the distal humerus | advanced
- The capitellum is an ANTERIOR structure. All displaced fractures sit anterior to the humeral shaft axis on a lateral radiograph and are exposed from a lateral (Kocher or extensile lateral column) approach, NOT a posterior approach. The posterior interosseous nerve is not normally at risk in isolated capitellar ORIF, but radial nerve branches and the lateral ulnar collateral ligament (LUCL) are.
- Lateral x-ray shows the DOUBLE ARC SIGN when the lateral trochlear ridge is involved (the capitellum and the lateral ridge of the trochlea produce two arcs) — this changes the classification (Bryan-Morrey type IV / Dubberley type B) and the approach: posterior trochlear comminution often requires a second medial or posterior exposure.
- Headless compression screws (Herbert / Acutrak / Mini-Acutrak) are the standard implant. Direction is FRAGMENT-SPECIFIC: anterior-to-posterior (AP) for Hahn-Steinthal whole-capitellum fragments where the posterior cortex is intact; posterior-to-anterior (PA) for fragments that have a posterior exit point. The thread pitch differential compresses the fragment against the intact condyle.
- Capitellar blood supply enters posteriorly from branches of the recurrent interosseous and radial collateral vessels. Dissection off the anterior capsule preserves the tenuous intra-osseous supply — minimise soft-tissue stripping. AVN rates of zero to twenty-five percent are reported in series; small-fragment excision is a deliberate option when the fragment is too thin to hold fixation.
- “On a lateral elbow x-ray, the capitellar fragment ALWAYS lies anterior and superior to the radial head (it is sheared upwards and forwards by the impact against the radial head). Posterior displacement is rare — think first of an alternative diagnosis (radial head / posterior Monteggia) if you see a posterior fragment.
- “Differentiate Hahn-Steinthal (whole capitellum with subchondral bone, fixable) from Kocher-Lorenz (thin cartilage flake, usually excised) on imaging and intraoperatively — this is the decision point that determines fixation versus fragment excision.
- “ALWAYS test for LUCL integrity after the lateral approach — the LUCL origin is on the lateral epicondyle and is at risk during the dissection. If the ligament has been detached, reattach it through bone tunnels before closure to prevent posterolateral rotatory instability.
- “Document the radial head BEFORE fixation: an associated radial head fracture is present in up to 30 percent of capitellar shear injuries (the same axial load that produces the shear also drives the radial head into the capitellum). Plan a single-stage approach if a Mason II-III radial head fracture needs treatment.
When & Why
Indication. A displaced capitellar or coronal shear fracture of the distal humerus that is reconstructable — an articular step greater than 2 mm, any rotational malalignment that blocks flexion or extension, or a rotated fragment impacted in the coronoid or radial fossa — in a patient who will benefit from a congruent radiocapitellar joint. A CT scan is mandatory before listing: it confirms the fragment size, the integrity of the posterior condyle, and any associated radial head or coronoid injury that changes the plan. Absolute indications for ORIF: - A displaced coronal shear fracture (articular step greater than 2 mm, or rotational malalignment that blocks motion) — the step-off at the radiocapitellar joint accelerates post-traumatic arthritis.
- Locking or blocking of flexion or extension by a rotated capitellar fragment impinging in the coronoid or radial fossa.
- A Hahn-Steinthal whole-capitellum fracture with a reconstructable fragment in any age group — fixation is preferred to excision because excision produces proximal radial migration and instability.
- Dubberley type A1, A2, B1 or B2 in the active patient — lateral approach ORIF is the standard of care.
- An open fracture — urgent irrigation, debridement and ORIF with antibiotic cover; assess for compartment syndrome. Relative indications. A small, non-reconstructable cartilage flake (Kocher-Lorenz) in a low-demand elderly patient is better served by fragment excision; a comminuted capitellum with extensive posterior wall involvement (Dubberley A3 or B3) may need staged ORIF versus primary fragment excision and early total elbow arthroplasty in the very low-demand elderly; and an associated elbow dislocation must have its ligamentous injury addressed, because fixing the fragment alone is insufficient. Assess the whole elbow, not just the capitellum. Before committing, exclude or plan for: - Lateral trochlear ridge involvement — the double arc sign on the lateral film (Dubberley type B). Posterior comminution (suffix 2 or 3) often needs a second medial or posterior exposure.
- An associated radial head fracture — present in up to 30 percent of capitellar shear injuries (the same axial load). A non-reconstructable Mason III head needs a metallic replacement in the same setting; never excise it in a high-demand patient.
- A coronoid fracture or elbow dislocation — the ligamentous injury and any coronoid fragment must be addressed for a stable elbow. The one decision that matters. Once you have decided the fragment is reconstructable, every pathway begins with the same lateral exposure of the anterior fragment. The choice is what you do with it:
The standard of care for the active patient. Headless compression screws restore radiocapitellar congruity, prevent proximal radial migration, and give good-to-excellent outcomes in 70 to 90 percent of modern series.
Reserved for the non-reconstructable fragment — a thin Kocher-Lorenz cartilage flake, or a comminuted fragment in a low-demand elderly patient. Acceptable outcomes; some loss of grip strength and radiocapitellar congruity.
A salvage option for the very low-demand elderly patient with a comminuted, unreconstructable capitellar and trochlear injury. Permanent lifting restriction of 5 kg; the patient must be counselled about activity limits.
Contraindications. Absolute: active elbow sepsis (clear the infection first, or convert to excision and antibiotic spacer), and a patient medically unfit for surgery. Relative: the very low-demand elderly patient with a comminuted unreconstructable injury (consider excision or TEA), established post-traumatic arthritis with loss of donor-condyle cartilage (fixation cannot restore a destroyed surface), and severe osteoporosis that will not hold screw purchase (consider suture fixation or excision). Consent specifically for avascular necrosis (zero to twenty-five percent reported, often asymptomatic), stiffness (10 to 30 percent have residual loss of motion; 5 to 10 percent need a capsular release), post-traumatic arthritis (20 to 40 percent radiographic at 5 years; symptomatic in 10 to 20 percent), fixation failure or screw prominence (5 to 10 percent), ulnar nerve symptoms (1 to 3 percent), and posterolateral rotatory instability if the LUCL is not preserved.
The Operation
The goal: expose the rotated anterior fragment through a lateral approach while protecting the LUCL and the capitellar blood supply, reduce it anatomically, and hold it with buried headless compression screws — then confirm a stable elbow and begin early motion. The exposure (positioning, the Kocher or Kaplan interval, identification of the LUCL, and the anterior capsulotomy) is the heart of the operation and is laid out step by step below.
Operative sequence
- Position. Two options. Supine with the arm on a hand table is most common — the arm is abducted and the elbow flexed over the table, giving easy AP and lateral fluoroscopy with the surgeon seated. Lateral decubitus with the arm over a padded bolster lets the elbow flex under gravity and is useful for combined or extensile approaches.
- Tourniquet. Upper-arm, inflated to 250 mmHg after exsanguination; keep tourniquet time under 90 to 120 minutes to avoid nerve compression.
- Anaesthesia. General anaesthesia with an interscalene block for post-operative analgesia. Examine under anaesthesia before draping — test varus, valgus and the lateral pivot-shift to assess stability.
- Fluoroscopy. Image intensifier on the opposite side from the surgeon. A true lateral of the elbow is critical; the radiocapitellar joint is best seen on a true lateral with the forearm in neutral rotation.
- Landmarks. Mark the lateral epicondyle, the radial head, the olecranon, the lateral border of the extensor mass, and the LUCL origin (the soft spot just proximal and posterior to the epicondyle). Plan a curved incision centred over the lateral epicondyle, 8 to 10 cm long, beginning 3 to 4 cm proximal to the epicondyle and extending distally over the radiocapitellar joint.
- Incise skin and subcutaneous fat. The fascia over the extensor mass and the anconeus is identified; the interval between the anconeus (posterior) and the extensor carpi ulnaris (anterior) is the Kocher interval and overlies the LUCL.
- Identify the LUCL as a discrete thickening on the deep surface of the fascia, from the lateral epicondyle to the supinator crest of the ulna. Put a stay suture in its origin now so it can be reattached anatomically at the end.
- Protect the cutaneous branch of the posterior antebrachial cutaneous nerve (a branch of the radial nerve) in the subcutaneous plane.
- Deepen through the Kocher interval, developing the plane between the anconeus (posterior) and the ECU (anterior); the LUCL lies in this plane. Reflect the anconeus posteriorly and the ECU anteriorly.
- Identify the annular ligament distally, encircling the radial head — it is usually intact in an isolated capitellar fracture but may be torn with an associated dislocation or radial head fracture.
- The anterior capsule is now visible deep to the extensor mass. The capitellar fragment lies anterior to the distal humerus, typically rotated and impacted in the coronoid or radial fossa.
- Incise the anterior capsule longitudinally in line with the skin incision, from just anterior to the lateral epicondyle distally to the radial head, and reflect it off the anterior humerus with a periosteal elevator to expose the anterior capitellum.
- The fragment is usually sitting in the coronoid fossa, rotated about 90 degrees with the articular surface facing anteriorly. Do not grasp it with a rongeur (it crushes the cartilage) — mobilise it gently with a dental pick or a fine K-wire joystick.
- Preserve every soft-tissue attachment on the deep (anterior) surface of the fragment — this is its only blood supply. Releasing the anterior capsule does not produce instability (it is not a primary restraint) but does allow earlier flexion.
- Irrigate the bed with saline; remove haematoma and tiny loose cancellous fragments that cannot be re-implanted, but keep all salvageable cancellous bone for grafting impacted defects.
- Inspect the donor site for size and shape, for posterior condylar integrity (Dubberley suffix 1, 2 or 3), and for any impaction that needs elevating.
- Gently elevate impacted subchondral bone with a fine curette or small osteotome to restore the normal capitellar contour.
- Reduce the capitellar fragment onto the donor bed using a dental pick and fine K-wire joysticks. For a Dubberley type B, reconstruct the larger piece first — whichever component (capitellum or lateral trochlear ridge) has the intact cortical reference.
- Judge reduction by the articular surface contour (a smooth, congruent radiocapitellar joint), palpation of the fracture line, and multi-plane fluoroscopy (AP, lateral, oblique).
- Provisionally fix with smooth 0.045 or 0.062 inch K-wires from anterior to posterior or from a non-articular margin — placed outside the planned screw trajectory so they do not interfere with the definitive screws.
- Choose screw size by fragment size: 2.0, 2.4, 2.7 or 3.0 mm headless compression screws (Herbert, Acutrak, Mini-Acutrak). Two to three screws are typical; pick a diameter less than one-third of the smallest fragment dimension to avoid splitting it.
- Anterior-to-posterior (AP) is the standard trajectory for a Hahn-Steinthal whole-capitellum fragment with an intact posterior cortex: entry on the anterior non-articular surface just proximal to the radial fossa, exiting through the posterior condyle, the threads engaging only posteriorly so the differential pitch compresses the fragment.
- Posterior-to-anterior (PA) is preferred when the fragment has a clean posterior exit point and the anterior condyle is the larger intact surface: entry through a small posterior cortical window.
- Place the guide wire under fluoroscopy, confirm position on AP/lateral/oblique, measure, drill with the cannulated drill, insert the screw, then add a second screw in a divergent trajectory to control rotation. The screw head must be buried beneath the articular cartilage, and the tip must not penetrate the posterior cortex into the olecranon fossa. Remove the guide wire and provisional K-wires.
- Take the elbow through a full range of motion under direct vision; the fragment should be stable with no motion at the fracture line.
- If motion remains, add a third screw, use a mini-fragment plate as a posterior buttress, or add a suture anchor / trans-osseous suture.
- Confirm stability with multi-plane fluoroscopy at the extremes of motion (full flexion, full extension, pronation and supination).
- Test varus and valgus under fluoroscopy for joint-space opening, and the lateral pivot-shift apprehension test under anaesthesia (forearm supinated, axial load, elbow brought from extension into flexion; a positive test gives a palpable clunk as the radius and ulna subluxate posteriorly).
- If the LUCL has been detached, reattach it through trans-osseous bone tunnels at the isometric point on the lateral epicondyle with a heavy non-absorbable suture. A medial collateral ligament injury (rare in isolated capitellar fractures) is addressed through a separate medial approach.
- Radial head fracture. A non-reconstructable Mason III head needs a metallic radial head arthroplasty in the same setting — do not excise it (excision produces proximal radial migration and wrist pain). A Mason II head greater than 2 mm displaced is fixed with mini-fragment screws.
- Coronoid fracture. A small Regan-Morley type I tip fragment can be left if the elbow is stable; larger type II-III fractures need fixation through a separate medial approach.
- Elbow dislocation. If the elbow was dislocated at presentation, the medial collateral ligament and anterior capsule are often torn and usually heal with functional bracing once the bony injury is stably fixed.
- Irrigate. Close the anterior capsule loosely with absorbable sutures (it is not a primary restraint). Reattach the LUCL to the lateral epicondyle if it was detached. Close the Kocher interval with absorbable sutures; insert a suction drain if dissection was extensive.
- Close the skin with non-absorbable sutures or staples. Apply a sterile dressing and a back-slab in 60 to 90 degrees of flexion with the forearm in neutral rotation.
A screw head left proud in the radiocapitellar joint destroys the radial head cartilage rapidly. Bury every screw head beneath the articular cartilage (countersunk) and keep the tip within the posterior condyle — a screw penetrating into the olecranon fossa impinges in extension. Confirm screw position on AP, lateral and oblique fluoroscopy before closing. If the fragment is too small or osteoporotic to bury a screw, the fragment may be too thin to fix — consider excision.
The LUCL is the primary restraint to posterolateral rotatory instability. It lies in the Kocher interval and is easily detached from the lateral epicondyle during exposure. Identify its isometric origin first, protect it throughout, and if it is detached reattach it through trans-osseous tunnels at the isometric point before closure. Test the lateral pivot-shift under anaesthesia at the end.
The capitellum is revascularised from posterior (radial collateral and recurrent interosseous vessels). The fragment is largely cartilaginous with a tenuous supply, so do not skeletonise it — reduce it with the attached anterior capsule as a hinge. If AVN occurs it is usually contained by the condylar shell and well tolerated.
Start the incision 3 to 4 cm PROXIMAL to the lateral epicondyle, curve it gently over the epicondyle, and extend it distally along the radiocapitellar joint. The proximal extension is what lets you place the screws and inspect the posterior condyle when you need to. Do not extend distally past the proximal radius — the posterior interosseous nerve is at risk there (pronate the forearm to move the PIN anteriorly and away if you must dissect past the radial neck).
The Kocher interval (anconeus versus ECU) overlies the LUCL and is preferred when the fragment is more posterolateral; the Kaplan interval (ECRB versus EDC) is anterior to the LUCL and spares the ligament, preferred when the fragment is more anterior. The choice is a viva favourite — know which structure each interval puts at risk.
Alternative approaches. When the pattern demands more than a single lateral exposure: the extensile lateral column (Kaplan) approach (ECRB versus EDC, anterior to the LUCL) suits a more anterior fragment and spares the ligament; a posterior approach (lateral decubitus or prone, midline incision, ulnar nerve protected, triceps reflected or olecranon osteotomy) is used for extensive posterior condylar comminution needing a buttress plate (Dubberley suffix 2 or 3), often combined with a separate lateral approach for the anterior shear fragment; and a medial approach (ulnar nerve identified and protected, MCL protected) exposes the coronoid or medial column when it needs fixation.
Aftercare & Complications
Rehabilitation. Stiffness is a greater threat than fixation failure, so motion starts early. | Phase | Timing | Programme | Milestone | |-------|--------|-----------|-----------| | 1 | Day 0 to 14 | Back-slab in near-full extension for 24 to 48 hours to control swelling; active assisted ROM from day 2; elevation; paracetamol and NSAIDs, opioids as needed | Wound check at 48 hours and 10 to 14 days; sutures out at 10 to 14 days | | 2 | Week 2 to 6 | Progressive active assisted and passive ROM supervised by a hand or upper-limb therapist; gentle isometric strengthening from 4 to 6 weeks; static progressive (turnbuckle) splint if motion plateaus | Functional arc of 30 to 130 degrees by 6 weeks | | 3 | Week 6 to 12 | Resistive exercises from 6 to 8 weeks; AP and lateral x-rays at 2, 6 and 12 weeks | About 80 percent of final motion by 3 months | | 4 | Month 3 to 12 | Graded return to function; x-ray at 6 months | Motion plateaus by 6 months; end-result by 12 months | Return to function. Light activities from week 2 to 3; driving once grip is safe (typically 4 to 6 weeks); sedentary work at 2 to 4 weeks; heavy manual work at 3 to 6 months; non-contact sport at 4 to 6 months and contact or overhead sport at 6 to 9 months. A residual loss of 10 to 30 degrees of terminal flexion or extension is common at one year. Heterotopic ossification prophylaxis. Indomethacin 25 mg three times daily for 3 to 6 weeks in high-risk patients (head injury, burn injury, recurrent surgery, severe soft-tissue injury, combined injuries). Single-dose radiation therapy (700 to 800 cGy) within 72 hours of surgery is an alternative for high-risk patients. Complications
- Incidence
- Zero to 25 percent across series; clinically significant less than 5 percent
- Recognition
- Increased radiographic density of the fragment, then collapse of subchondral bone; usually asymptomatic because the condylar shell contains the fragment
- Prevention and management
- Prevention: preserve the soft-tissue hinge, minimise stripping, use a single lateral approach when possible. Management: observe — AVN alone is usually well tolerated; revise to arthroplasty only if collapse is symptomatic
- Incidence
- 20 to 40 percent radiographic at 5 years; symptomatic in 10 to 20 percent
- Recognition
- Progressive loss of motion, crepitus, pain with loading; joint-space narrowing, sclerosis and osteophytes on x-ray
- Prevention and management
- Prevention: anatomic reduction with articular step less than 2 mm and stable fixation permitting early motion. Management: NSAIDs, activity modification, injection; arthroscopic debridement for symptomatic spurs; total elbow arthroplasty for end-stage disease in older patients
- Incidence
- 10 to 30 percent have residual loss of motion greater than 30 degrees; 5 to 10 percent need a capsular release
- Recognition
- Loss of terminal flexion or extension despite rehab; mature anterior capsular scar; heterotopic ossification
- Prevention and management
- Prevention: early motion after 24 to 48 hours of splinting, NSAIDs or indomethacin for HO prophylaxis in high-risk patients, adequate analgesia. Management: intensive therapy, dynamic splinting, capsular release or arthrolysis at 6 to 9 months if motion plateaus
- Incidence
- 5 to 10 percent
- Recognition
- Recurrent pain, mechanical catching, loss of motion, screw back-out or penetration of the radiocapitellar joint on x-ray
- Prevention and management
- Prevention: bury the screw head beneath cartilage, choose a screw less than one-third of the fragment dimension, use divergent screws for rotational control. Management: revision for prominent or loose screws
- Incidence
- Less than 5 percent if the LUCL is preserved; up to 15 percent if detached and not repaired
- Recognition
- Positive lateral pivot-shift; apprehension with forearm supination and axial load in extension; recurrent subluxation
- Prevention and management
- Prevention: identify and preserve the LUCL, reattach it trans-osseously if detached. Management: LUCL reconstruction with a palmaris or tendon graft if symptomatic — secondary repair alone has poor outcomes
- Incidence
- 10 to 20 percent radiographic; symptomatic less than 5 percent
- Recognition
- Loss of motion despite adequate rehab; calcified mass in the anterior capsule or around the collaterals, mature on x-ray by 6 to 8 weeks
- Prevention and management
- Prevention: indomethacin 25 mg three times daily for 3 to 6 weeks, or single-dose radiation, in high-risk patients. Management: observe if asymptomatic; excise once mature (6 to 9 months) with prophylaxis to prevent recurrence
- Incidence
- 1 to 3 percent
- Recognition
- Paraesthesia in the ulnar distribution, intrinsic weakness in severe cases, positive Tinel at the cubital tunnel
- Prevention and management
- Prevention: avoid prolonged elbow flexion post-operatively; identify the ulnar nerve in any medial approach. Management: activity modification and splinting; release or transposition if symptoms persist beyond 3 to 6 months
- Incidence
- Rare in isolated capitellar ORIF; up to 5 percent in combined radial head procedures
- Recognition
- Weakness of finger and thumb extension post-operatively; usually a neuropraxia
- Prevention and management
- Prevention: pronate the forearm during any posterior dissection past the radial neck; avoid retractors on the dorsal proximal radius. Management: expectant — most resolve within 3 to 6 months; EMG at 6 weeks if not improving; explore if no recovery by 4 to 6 months
Special case — Dubberley type 2 or 3 (posterior comminution). When the posterior condyle is comminuted (suffix 2) or split (suffix 3) it cannot be relied on for screw purchase or to contain the anterior fragment, and the injury is at high risk of fixation failure, re-displacement and AVN. Use a two-incision approach — lateral for the anterior shear fragment, medial or posterior for the posterior condyle, which is fixed with a buttress plate (mini-fragment or precontoured distal humeral plate) and bone-grafted for structural support. Counsel the patient pre-operatively about the more guarded prognosis (higher re-operation and arthritis rates). Special case — capitellar fracture with an associated radial head fracture. The same axial load that produces the shear often drives the radial head into the capitellum (a Mason II or III head fracture, sometimes called a Mason IV pattern with dislocation). Plan a single-stage lateral approach for both: fix the capitellum first (the larger reconstructable surface), then address the radial head — ORIF for a Mason II fragment greater than 2 mm displaced, or a metallic radial head arthroplasty for a non-reconstructable Mason III (never excise in a high-demand patient). Assess stability at the end and repair the lateral collateral ligament, adding a medial repair or hinged external fixator in severe cases. Combined injuries carry more post-traumatic arthritis, stiffness and heterotopic ossification. Special case — the low-demand elderly patient with a comminuted non-reconstructable fracture. For a patient older than 70, low-demand, with a comminuted capitellar and trochlear fracture that cannot be reconstructed, consider acute fragment excision with early mobilisation, or acute total elbow arthroplasty for extensive comminution (a salvage option with a permanent 5 kg lifting restriction). The goal here is a painless, stable, functional arc (30 to 130 degrees), not anatomic restoration of the articular surface.
Viva & Exam Focus
CAPITCAPIT — capitellar anatomy and the surgical window
REDUCEREDUCE — operative sequence for coronal shear ORIF
The trap. Treating the anterior fragment like cortical bone that can be freely debrided and mobilised. The supply enters posteriorly (radial collateral and recurrent interosseous vessels); the fragment is largely cartilaginous and depends on its soft-tissue hinge. The fix. Reduce the fragment with the attached anterior capsule as a hinge, never skeletonise it, and place screws without circumferential stripping. AVN is usually contained by the condylar shell and well tolerated.
The trap. Detaching the LUCL origin from the lateral epicondyle for exposure and not repairing it. Loss of the LUCL produces a pivot shift under anaesthesia and a chronically unstable elbow. The fix. Identify the isometric origin, protect it, and if detached reattach it through bone tunnels or suture anchors at the isometric point before closure; test the pivot-shift at the end.
The trap. Always drilling anterior-to-posterior. Trajectory depends on fragment geometry and posterior wall integrity; AP insertion risks intra-articular prominence when there is a posterior exit point or comminution. The fix. Trace the fracture line on CT pre-operatively. Use PA insertion when the fragment has a clean posterior exit point and the anterior condyle is the larger intact surface. Confirm every screw is buried beneath cartilage on fluoroscopy.
The trap. Calling it a capitellar fracture and missing the lateral trochlear ridge component. On a true lateral, two parallel arcs (outer = capitellum, inner = lateral trochlear ridge) mean a Bryan-Morrey type IV / Dubberley type B. The fix. Obtain a CT for every coronal shear fracture. Look for trochlear involvement and posterior comminution (Dubberley suffix 2 or 3), which often requires a medial or posterior approach and a second incision.
The trap. Treating the capitellar fragment in isolation and missing the radial head fracture, coronoid fracture or LCL injury (the terrible triad or Mason IV pattern). The fix. Examine the radial head and coronoid on CT and the ligaments under anaesthesia before planning fixation. A non-reconstructable Mason III head (greater than 3 fragments) needs replacement, not excision; an unstable elbow needs LCL repair.
The trap. Trying to screw or wire a thin Kocher-Lorenz cartilage flake. It is essentially cartilage with a wafer of subchondral bone and will fragment further on attempted fixation. The fix. When the fragment is non-reconstructable (Kocher-Lorenz, Dubberley A2 in an elderly patient), excise it and treat the donor bed; outcomes in low-demand patients are acceptable. The decision is made intra-operatively after visual inspection.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old right-hand-dominant woman falls on an outstretched hand and presents with a painful, swollen elbow. Imaging shows a displaced capitellar fracture with the lateral trochlear ridge involved. CT confirms a Hahn-Steinthal fragment with the posterior condyle intact. Walk me through your management plan.”
“A 58-year-old man presents 4 weeks after a fall with a missed capitellar fracture. He has 30 degrees of fixed flexion deformity and pain on attempted flexion beyond 90 degrees. CT shows a healed, displaced capitellar fragment. He is low-demand (office worker, no sport). What are your options?”
“A 24-year-old competitive rugby player presents with a coronal shear fracture and an associated Mason III radial head fracture with 4 fragments. The elbow is stable under anaesthesia. What is your surgical plan?”
Key diagnosis points
- The capitellum is an anterior structure — displaced fragments lie anterior and superior on a lateral radiograph
- Double arc sign on lateral x-ray equals capitellum plus lateral trochlear ridge involvement (Dubberley type B)
- CT is mandatory for all coronal shear fractures — fragment size, posterior condyle integrity, associated radial head or coronoid injury
- Hahn-Steinthal equals whole capitellum with subchondral bone (fixable); Kocher-Lorenz equals thin cartilage flake (usually excised)
- An associated radial head fracture is present in up to 30 percent — the same axial-load mechanism (Mason IV pattern)
Classification — Dubberley
- Type A: capitellum only. Type B: capitellum plus trochlea (lateral ridge). Subdivided by posterior wall: 1 intact, 2 comminuted, 3 fracture line through posterior condyle
- Type A1: lateral approach, AP screws. Types A2-3 and B2-3: consider a dual approach (lateral plus medial or posterior)
- Bryan-Morrey: I Hahn-Steinthal, II Kocher-Lorenz, III comminuted, IV coronal shear with posterior extension (double arc)
Surgical anatomy
- The capitellum lies entirely anterior to the humeral shaft axis on a true lateral radiograph
- Blood supply is posterior, from the radial collateral and recurrent interosseous vessels — preserve the soft-tissue hinge
- LUCL origin: the isometric point on the lateral epicondyle, just proximal to the capitellar fragment — the primary restraint to PLRI
- The anterior capsule is not a primary restraint and can be released for exposure without producing instability
- The radial nerve and PIN are at risk in proximal-radius dissection — pronate the forearm to protect the PIN
Indications for ORIF
- A displaced fragment (step greater than 2 mm) — an absolute indication
- A mechanical block to motion (rotated fragment in the coronoid or radial fossa)
- A Hahn-Steinthal whole-capitellum fracture in any active patient
- Dubberley type A1, A2, B1 or B2 in the active patient
- An open fracture — urgent ORIF with antibiotic cover
Contraindications to ORIF
- Active elbow sepsis
- A patient medically unfit for surgery
- The very low-demand elderly patient with a comminuted non-reconstructable fracture (consider excision or TEA)
- Established post-traumatic arthritis with loss of donor cartilage
- Severe osteoporosis precluding screw purchase
Operative technique — key steps
- Position supine with the arm on a hand table; tourniquet; image intensifier on the opposite side
- Examine under anaesthesia for stability (varus, valgus, pivot-shift)
- Mark the LUCL origin on the lateral epicondyle; plan a Kocher or Kaplan approach
- Identify and protect the LUCL throughout — reattach it at the end if detached
- Develop the Kocher interval (anconeus versus ECU) or Kaplan interval (ECRB versus EDC)
- Anterior capsulotomy to expose the rotated anterior fragment
- Reduce the fragment with a dental pick; provisional K-wire fixation outside the screw trajectory
- Fix with 2 to 3 headless compression screws (2.0 to 3.0 mm Acutrak or Herbert); trajectory per fragment geometry (AP for Hahn-Steinthal; PA for a posterior exit fragment)
- Multi-plane fluoroscopy to confirm reduction and screw position — heads buried beneath cartilage
- Test stability and range of motion under direct vision
- Reattach the LUCL trans-osseously at the isometric point if detached
- Back-slab in extension for 24 to 48 hours; indomethacin for HO prophylaxis in high-risk patients
Danger zones
- LUCL origin at the lateral epicondyle — must be identified, protected and reattached to prevent PLRI
- Capitellar blood supply is posterior — dissect off the capsule and preserve the soft-tissue hinge
- A proud screw in the radiocapitellar joint destroys radial head cartilage — bury the head beneath cartilage
- Radial nerve and PIN are at risk with proximal-radius dissection — pronate the forearm to move the PIN anteriorly
- Recurrent interosseous and radial collateral vessels — preserve soft tissue to the fragment
Complications
- Avascular necrosis: zero to 25 percent in series; usually contained by the condylar shell and often asymptomatic
- Post-traumatic arthritis: 20 to 40 percent radiographic at 5 years; symptomatic in 10 to 20 percent
- Stiffness: 10 to 30 percent have residual loss of motion greater than 30 degrees; 5 to 10 percent need a capsular release
- Fixation failure: 5 to 10 percent; usually related to screw prominence or poor bone quality
- Posterolateral rotatory instability: less than 5 percent if the LUCL is preserved; up to 15 percent if detached and not repaired
- Heterotopic ossification: 10 to 20 percent radiographic; symptomatic less than 5 percent; indomethacin prophylaxis in high-risk patients
Special cases
- Dubberley type 2-3 (posterior comminution): dual approach; posterior buttress plate; bone graft for comminution
- Capitellum plus Mason III radial head: fix the capitellum first; replace the radial head (metallic arthroplasty) if non-reconstructable
- Low-demand elderly with comminution: fragment excision or acute total elbow arthroplasty
- Paediatric capitellar fracture (rare): fragment excision typically preferred; ORIF in older children with a reconstructable fragment
- Missed, malunited fragment at greater than 4 weeks: late ORIF if active; fragment excision if low-demand; salvage procedures for established arthritis
Background & Evidence
Why a lateral approach. The capitellum is the anterior and inferior articular surface of the lateral column of the distal humerus and articulates only with the radial head; it lies entirely anterior to the humeral shaft axis, so the sheared fragment sits anteriorly and is reached from the lateral side. The trochlea is the medial counterpart, more posterior, with a central groove and medial and lateral ridges; involvement of the lateral trochlear ridge produces the double arc sign on the lateral film. Blood supply. The capitellum is supplied by the radial collateral and recurrent interosseous arteries, which enter posterolaterally through the lateral epicondylar soft-tissue attachments. The intra-osseous supply to the anterior cartilaginous portion is tenuous — which is why anterior dissection and stripping risk AVN, and why a soft-tissue hinge must be preserved. Lateral ligamentous anatomy. The LUCL (origin at the isometric point on the lateral epicondyle, insertion on the supinator crest of the ulna) is the primary restraint to posterolateral rotatory instability and the most posterior part of the lateral complex; it lies in the Kocher interval. The radial collateral ligament is more anterior and inserts on the annular ligament, which encircles the radial head. The anterior capsule inserts just proximal to the coronoid fossa and is not a primary restraint, so releasing it for exposure does not destabilise the elbow. Classification. Two systems are used together. The Bryan-Morrey modification describes the morphology; the Dubberley system guides the approach.
- Name
- Hahn-Steinthal
- Description
- A large fragment of the whole capitellum with subchondral bone — reconstructable, the usual candidate for ORIF
- Name
- Kocher-Lorenz
- Description
- A thin shell of articular cartilage with minimal bone — usually too thin to fix, so excised
- Name
- Comminuted
- Description
- A comminuted capitellar fracture — fixation versus excision decided intra-operatively
- Name
- Coronal shear
- Description
- A coronal shear extending posteriorly into the trochlea (the double arc sign) — often needs a broader or dual approach
- Definition
- Capitellum only
- Surgical implication
- Single lateral approach usually suffices
- Definition
- Capitellum plus trochlea (lateral ridge) — the double arc sign
- Surgical implication
- Assess and reduce the trochlear component; a broader exposure may be needed
- Definition
- Posterior condyle intact
- Surgical implication
- Single lateral approach with headless screws
- Definition
- Posterior condyle comminuted
- Surgical implication
- Consider a dual approach plus a posterior buttress plate
- Definition
- Fracture line through the posterior condyle
- Surgical implication
- Dual approach (lateral plus medial or posterior); bone graft for comminution
Outcomes of ORIF. Modern series restore a congruent radiocapitellar joint in the majority, with Broberg-Morrey good-to-excellent scores in approximately 70 to 90 percent. A functional arc is restored, though the mean flexion-extension arc is typically 10 to 30 degrees less than the uninjured side. The strongest predictor of outcome is the quality of the initial reduction — an articular step greater than 2 mm correlates strongly with post-traumatic arthritis. AVN is reported in zero to 25 percent of cases but is clinically significant in fewer than 5 percent, because the condylar shell contains the fragment. Why headless compression screws. The differential thread pitch produces interfragmentary compression and the screws can be buried beneath the articular cartilage, avoiding intra-articular prominence — the reason they have displaced K-wires and bioabsorbable pins as the implant of choice. Two to three screws are typical, the trajectory (AP versus PA) set by fragment geometry and posterior cortex integrity. For very small or osteoporotic fragments, supplementary mini-fragment plates, suture anchors or bioabsorbable pins have been described with more variable outcomes. ORIF versus fragment excision. Modern series favour ORIF for every reconstructable fragment because it restores radiocapitellar congruity and prevents proximal radial migration. Excision is reserved for the non-reconstructable fragment (a thin Kocher-Lorenz flake, or severe comminution in a low-demand patient). Long-term follow-up shows progressive post-traumatic arthritis in a subset of patients, which appears more closely related to the initial cartilage injury at impact than to the fixation technique.
- ORIF (reconstructable fragment)
- 70 to 90 percent in modern series
- Excision (non-reconstructable / low demand)
- 60 to 80 percent in low-demand elderly patients
- ORIF (reconstructable fragment)
- 100 to 130 degrees
- Excision (non-reconstructable / low demand)
- 90 to 120 degrees
- ORIF (reconstructable fragment)
- 20 to 40 percent
- Excision (non-reconstructable / low demand)
- 30 to 50 percent
- ORIF (reconstructable fragment)
- 0 to 25 percent (usually contained, often asymptomatic)
- Excision (non-reconstructable / low demand)
- Not applicable
- ORIF (reconstructable fragment)
- 5 to 15 percent (stiffness release, hardware removal)
- Excision (non-reconstructable / low demand)
- Low for excision alone
- ORIF (reconstructable fragment)
- Active patients, Hahn-Steinthal, reconstructable fragments
- Excision (non-reconstructable / low demand)
- Thin cartilage flake, elderly low-demand, comminuted non-reconstructable
References
Outcome after open reduction and internal fixation of capitellar and trochlear fractures
- Original description of the Dubberley classification of capitellar and trochlear fractures, subdividing by capitellum alone versus capitellum plus trochlea and by the integrity of the posterior condyle
- A cohort managed with ORIF for coronal shear fractures reported good-to-excellent functional outcomes in the majority, with the classification guiding the surgical approach
- Posterior condylar comminution (Dubberley type 2 or 3) is associated with a higher re-operation rate and a more guarded prognosis
Open reduction and internal fixation of capitellar fractures with headless screws
- Technique paper describing Herbert and Acutrak headless compression screws for displaced capitellar fractures, with the screws buried beneath the articular cartilage
- Anterior-to-posterior trajectory is preferred for whole-capitellum fragments with an intact posterior cortex; posterior-to-anterior is described for fragments with a posterior exit point
- Good-to-excellent functional outcomes in the majority, with restoration of a functional arc of motion in most
Coronal shear fractures of the distal humerus
- A descriptive series of coronal shear fractures of the distal humerus, characterising the fracture pattern and the role of ORIF
- Highlights the importance of a CT scan to assess for lateral trochlear ridge involvement (the double arc sign) and posterior condylar comminution
- Restoration of articular congruity with stable fixation allowing early motion is the key surgical goal
Large coronal shear fractures of the capitellum and trochlea treated with headless compression screws
- A cohort with large coronal shear fractures extending to the trochlea treated with headless compression screws through a lateral approach
- Good-to-excellent functional outcomes in the majority, with restoration of a functional motion arc
- Re-operation for stiffness (capsular release, hardware removal) was the most common secondary procedure
Fractures of the capitellum and trochlea: long-term outcome
- A long-term follow-up cohort of coronal shear fractures managed with ORIF
- Functional outcomes remain good at medium-term follow-up, with a progressive risk of post-traumatic radiographic arthritis that does not always correlate with symptoms
- ORIF is preferred over excision for reconstructable fragments because of the risk of proximal radial migration and instability after excision