Lateral · EDC–ECRB Interval · PIN at Risk · Pronation Protects the Nerve · Radial Head and Capitellum Access
- The EDC–ECRB interval is the key internervous plane — both extensor digitorum communis and extensor carpi radialis brevis are supplied by the posterior interosseous nerve distal to the interval, so no muscle is denervated.
- Full forearm pronation moves the posterior interosseous nerve (PIN) distally and medially by up to 2 cm, carrying it out of the operative field during radial head exposure.
- The approach gives direct access to the radial head, capitellum and lateral column and is more anterior than the Kocher approach, with superior visualisation of the anterior radial head.
- The Kocher approach (ECU–anconeus) is more posterior and safer for the PIN but gives less anterior access — choose Kaplan when anterior radial head and capitellar visualisation is needed.
- The lateral collateral ligament complex (LUCL) must be preserved or repaired: stay anterior to its origin on the lateral epicondyle to avoid posterolateral rotatory instability.
When & Why
What it exposes. The Kaplan approach gives direct lateral access to the radial head, the capitellum and the lateral column of the distal humerus through a true internervous plane. It is the workhorse exposure for radial head ORIF and replacement, capitellar fixation and lateral column plating. Why this approach. The Kaplan interval is more anterior than the Kocher approach, so it gives superior visualisation of the anterior half of the radial head and of the capitellum. Because both muscles of the interval are supplied by the posterior interosseous nerve distal to the plane, dissection here denervates neither muscle. Full pronation protects the PIN, making the approach safe when the technique is respected. Radial head fractures account for about 33 percent of all elbow fractures, and anatomic reduction of the capitellar articular surface demands the anterior exposure this approach provides. Primary indications: - Radial head fractures requiring ORIF or replacement (Mason II–IV)
- Capitellar fractures (coronal shear, Type I and II)
- Lateral column fractures and comminution requiring plating
- Combined radial head and capitellar pathology
- Elbow arthroscopy portal placement planning
- Revision surgery for malunited radial head fractures Contraindications and cautions: - Active infection over the lateral elbow
- Severe soft tissue compromise laterally (consider staged or alternative approach)
- Isolated medial pathology (use a medial approach)
- When posterior pathology is primary and a lower-PIN-risk Kocher exposure suffices Kaplan versus the alternatives. The Kaplan interval is the high-yield exam distinction — know how it differs from Kocher and when each lateral/medial route is preferred.
- Interval / route
- EDC–ECRB (more anterior)
- Best for
- Anterior radial head, capitellum, lateral column — needs pronation
- Interval / route
- ECU–anconeus (more posterior)
- Best for
- Posterior pathology, lower PIN risk, less anterior access
- Interval / route
- Olecranon-basing
- Best for
- Olecranon and distal humerus
- Interval / route
- Medial column
- Best for
- Medial column and coronoid
- Interval / route
- Along radial vessels
- Best for
- Anterior elbow and neurovascular structures
Position and landmarks. Supine on a radiolucent table, the arm across the chest or on a hand table with the elbow flexed 90 degrees. A high upper-arm tourniquet is applied; C-arm access is from the medial side or a ceiling mount. Before incision, mark the lateral epicondyle, the radial head (palpated anterior to the epicondyle during forearm rotation), the olecranon tip and the lateral supracondylar ridge (the line of proximal extension). The common extensor origin and the mobile wad (brachioradialis and ECRL) are the key soft-tissue landmarks. A standard radial-head exposure uses a 6–8 cm longitudinal or gently curved incision from the lateral epicondyle distally toward the radial neck.
The Exposure
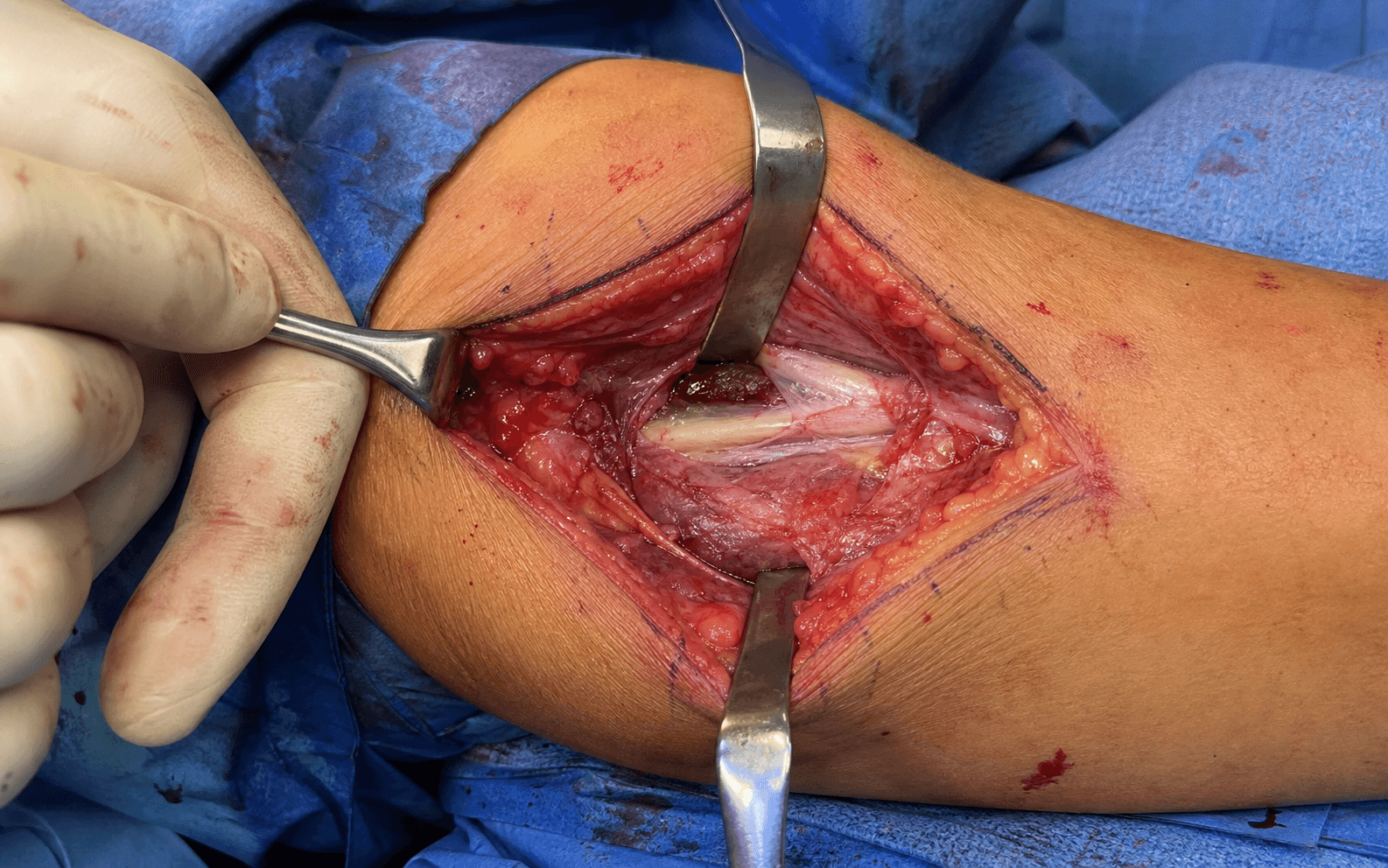
Work down through the layers on the lateral side, developing the EDC–ECRB interval, pronating to protect the PIN, and entering the joint anterior to the lateral collateral ligament.
Exposure sequence
- With the elbow flexed 90 degrees and forearm in neutral, mark the lateral epicondyle, the radial head (palpated during rotation) and the olecranon tip.
- A longitudinal or gently curved incision runs from the lateral epicondyle distally 6–8 cm toward the radial neck, passing just anterior to the lateral epicondyle prominence.
- For extensile work, plan the proximal extension along the lateral supracondylar ridge or the distal extension along the radial border at the outset.
- Incise skin and subcutaneous tissue and identify the interval between the mobile wad (brachioradialis and ECRL) anteriorly and the common extensor origin posteriorly.
- The Kaplan interval lies one layer deeper, between ECRB (anterior) and EDC (posterior).
- Develop this plane sharply, following the muscle-fibre orientation: ECRB fibres are more oblique and anterior, EDC fibres more longitudinal and posterior.
- Before any deep retraction, fully pronate the forearm and maintain it.
- The PIN enters the supinator about 3–4 cm distal to the lateral epicondyle; full pronation displaces the nerve distally and medially by up to 2 cm, carrying it out of the operative field.
- This manoeuvre must be performed and held before capsulotomy or any retraction against the supinator.
- With the forearm pronated, incise the fascia overlying the radial head and the joint capsule.
- The annular ligament is identified and preserved, or divided longitudinally only if exposure demands (it is repaired at closure).
- Small branches of the radial recurrent artery in the superficial dissection are coagulated or ligated for haemostasis.
- Incise the joint capsule anterior to the lateral collateral ligament origin on the lateral epicondyle.
- Staying anterior to the LCL preserves the lateral ulnar collateral ligament (LUCL) — the primary restraint to posterolateral rotatory instability.
- Tag the capsular edges for later repair if the LCL complex has been disturbed.
- With the forearm pronated, the radial head is fully exposed and the capitellum is visualised anteriorly.
- Irrigate to clear haematoma and loose bodies; the fracture lines or coronal shear fragment are now ready for reduction and fixation.
- Protect the LCL throughout — if it has been divided for exposure it must be repaired anatomically at closure.
The posterior interosseous nerve enters the supinator 3–4 cm distal to the lateral epicondyle and is the most important structure at risk. Injury causes loss of finger and thumb extension (finger drop) with wrist extension preserved (ECRL intact). Prevention is a disciplined technique: fully pronate before any deep dissection, stay anterior to the supinator where possible, use only gentle retraction, and never place retractors deep to the supinator without protection. Document finger and thumb extension immediately after surgery.
The PIN-protection manoeuvre (full pronation) is the classic Kaplan viva question: state it, do it before deep dissection, and maintain it throughout. Equally exam-critical is the capsulotomy — incise anterior to the LCL origin so the LUCL and elbow stability are preserved; if the LCL is divided, repair it to the lateral epicondyle with transosseous sutures or anchors.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Lateral cutaneous nerve of the forearm
- Protection
- Identify and protect any branches encountered in the subcutaneous plane
- Structure at risk
- Posterior interosseous nerve (PIN) within supinator
- Protection
- Full pronation before deep dissection; stay anterior to supinator; gentle retraction only
- Structure at risk
- Radial recurrent artery
- Protection
- Coagulate or ligate small branches; preserve the major vessel
- Structure at risk
- Lateral collateral ligament (LUCL)
- Protection
- Capsulotomy anterior to LCL origin; repair with transosseous sutures or anchors if divided
- Structure at risk
- Annular ligament
- Protection
- Preserve if possible; repair if divided to maintain proximal radioulnar joint stability
Post-operative complications
- Rate
- 2–5%
- Prevention
- Pronation technique, gentle retraction
- Treatment
- Observe; wrist and finger extension splint; explore if no recovery by 3 months
- Rate
- 1–3%
- Prevention
- Antibiotics, sterile technique
- Treatment
- Irrigation and debridement, antibiotics
- Rate
- 10–30%
- Prevention
- Anatomic articular reduction
- Treatment
- Analgesia, eventual arthroplasty
- Rate
- 10–20%
- Prevention
- Early range of motion
- Treatment
- Physiotherapy, manipulation under anaesthesia
- Rate
- 1–2%
- Prevention
- LCL preservation or repair
- Treatment
- LCL reconstruction if symptomatic
PIN injury — recognition and management. PIN injury in lateral elbow approaches ranges from 2 to 10 percent depending on technique and fracture complexity; the Kaplan interval carries a higher theoretical risk than Kocher because it is more anterior, but with proper pronation the risk is comparable. Most injuries are neurapraxia recovering within 3–6 months; permanent finger drop occurs in less than 1 percent. Intra-operatively, a transected nerve is primarily repaired. Post-operative finger drop is worked up with EMG/NCS at 3 weeks (allowing Wallerian degeneration to declare axonal injury); if there is no clinical or EMG recovery by 3 months, explore the nerve. A permanent deficit is managed with tendon transfers (flexor carpi radialis to extensor digitorum communis, palmaris longus to EPL). Always exclude a correctable cause first — tight dressing or compartment syndrome. Extensile options. Extend proximally along the lateral supracondylar ridge, elevating the common extensor origin and brachioradialis anteriorly, to expose the capitellum and lateral column for capitellar fractures and lateral column plating (watch for radial nerve branches proximally). Extend distally along the radial border, partially releasing the supinator from the radius with the forearm pronated, to reach the radial neck and proximal shaft (the PIN remains at risk — maintain pronation). For complex bicondylar injuries, the Kaplan approach can be combined with a medial (Hotchkiss) approach, sometimes requiring lateral decubitus or staged positioning. Closure and aftercare. Copious irrigation and meticulous haemostasis of the radial recurrent branches. Repair the annular ligament and LCL (if divided) with absorbable and transosseous/anchor fixation respectively; close the fascia over the common extensors loosely and approximate skin over a posterior splint or hinged brace locked at 90 degrees. Rehabilitation: immobilise at 90 degrees for 0–2 weeks, begin active-assisted ROM aiming for 0–120 degrees by 6 weeks, progressive strengthening 6–12 weeks, and return to activity after 12 weeks; no weight bearing through the arm for 6 weeks after fracture fixation. Follow up radiographs at 2, 6 and 12 weeks, with a final review at 6 months.
Procedures Through This Approach
- Radial head ORIF — the principal operation: reduce split fragments with pointed clamps, provisional K-wires, then 1.5 mm or 2.0 mm countersunk or headless screws; a buttress or locking radial head plate for comminution. Check forearm rotation under direct vision and fluoroscopy to ensure no mechanical block.
- Radial head replacement — for comminuted Mason III/IV fractures not amenable to fixation: measure diameter and height accurately, insert with the forearm pronated, and repair the annular ligament around the prosthetic neck.
- Capitellar fixation — reduce the coronal shear fragment anatomically and fix with headless compression screws inserted anterior-to-posterior, countersunk beneath the articular surface; add a lateral column plate for lateral column comminution.
- Lateral column plating — via the proximal extension along the supracondylar ridge for distal humerus fractures involving the lateral column.
- Elbow arthroscopy portal placement planning and exposure for combined radial head and capitellar pathology.
Viva & Exam Focus
KAPLANKAPLAN — the lateral elbow exposure
PRONATEPRONATE — protecting the posterior interosseous nerve
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old falls onto an outstretched hand and sustains a displaced radial head fracture (Mason II). CT confirms a split fracture with greater than 2 mm displacement. How would you approach this?”
“A 28-year-old sustains a coronal shear capitellar fracture (Type I) after a fall. How would you approach this and what are the key technical points?”
“You perform a Kaplan approach for radial head ORIF. Post-operatively the patient has finger and thumb drop but intact wrist extension. What is your assessment and management?”
Position and landmarks
- Supine with arm on a hand table or across the chest, elbow flexed 90 degrees
- Landmarks: lateral epicondyle, radial head (palpated in rotation), olecranon tip
- Incision: 6–8 cm from the lateral epicondyle distally toward the radial neck
- High upper-arm tourniquet; C-arm from the medial side
Internervous plane
- EDC (PIN) and ECRB (PIN) — a true internervous plane
- EDC fibres more longitudinal, ECRB more oblique
- Develop the plane sharply following fibre orientation
- No muscle denervation occurs
PIN protection (critical)
- PIN enters the supinator 3–4 cm distal to the lateral epicondyle
- FULL FOREARM PRONATION before deep dissection
- Pronation moves the PIN distally and medially by up to 2 cm
- Maintain pronation throughout radial head exposure; stay anterior to the supinator
Kaplan versus Kocher
- Kaplan: EDC–ECRB interval, more anterior, better radial head and capitellum access
- Kocher: ECU–anconeus interval, more posterior, safer for the PIN
- Kaplan requires pronation for PIN protection
- Choose Kaplan when anterior access is needed
LCL and stability
- LCL origin on the lateral epicondyle must be preserved or repaired
- Stay anterior to the LCL during capsulotomy
- Repair the LCL with transosseous sutures or anchors if divided
- Annular ligament repair maintains proximal radioulnar joint stability
- Failure leads to posterolateral rotatory instability
Extensile options
- Proximal: along the lateral supracondylar ridge for the capitellum and lateral column
- Distal: along the radial border, partial supinator release (pronated) for the radial neck
- Combine with a medial approach for bicondylar elbow fractures
- Lateral decubitus or staged positioning for combined approaches
References
Comparison of Exposure in the Kaplan Versus the Kocher Approach in the Treatment of Radial Head Fractures
- Cadaveric comparison demonstrated significantly greater anterior radial head exposure with the Kaplan (EDC–ECRB) approach versus Kocher
Location of the posterior interosseous nerve in relation to common lateral approaches to the elbow
- Precise anatomic mapping confirmed that forearm pronation displaces the PIN medially and distally away from both the Kaplan and Kocher intervals
Comparative evaluation of posterior interosseous nerve strain in lateral approach to radial head fixation: a cadaveric study
- Cadaveric strain analysis showed reduced PIN strain during radial head fixation when using the Kaplan interval with pronation positioning
The supinator approach to the lateral elbow: a technique description and literature review
- Describes a supinator-splitting modification of the lateral approach and reviews PIN safety data across Kaplan-type exposures