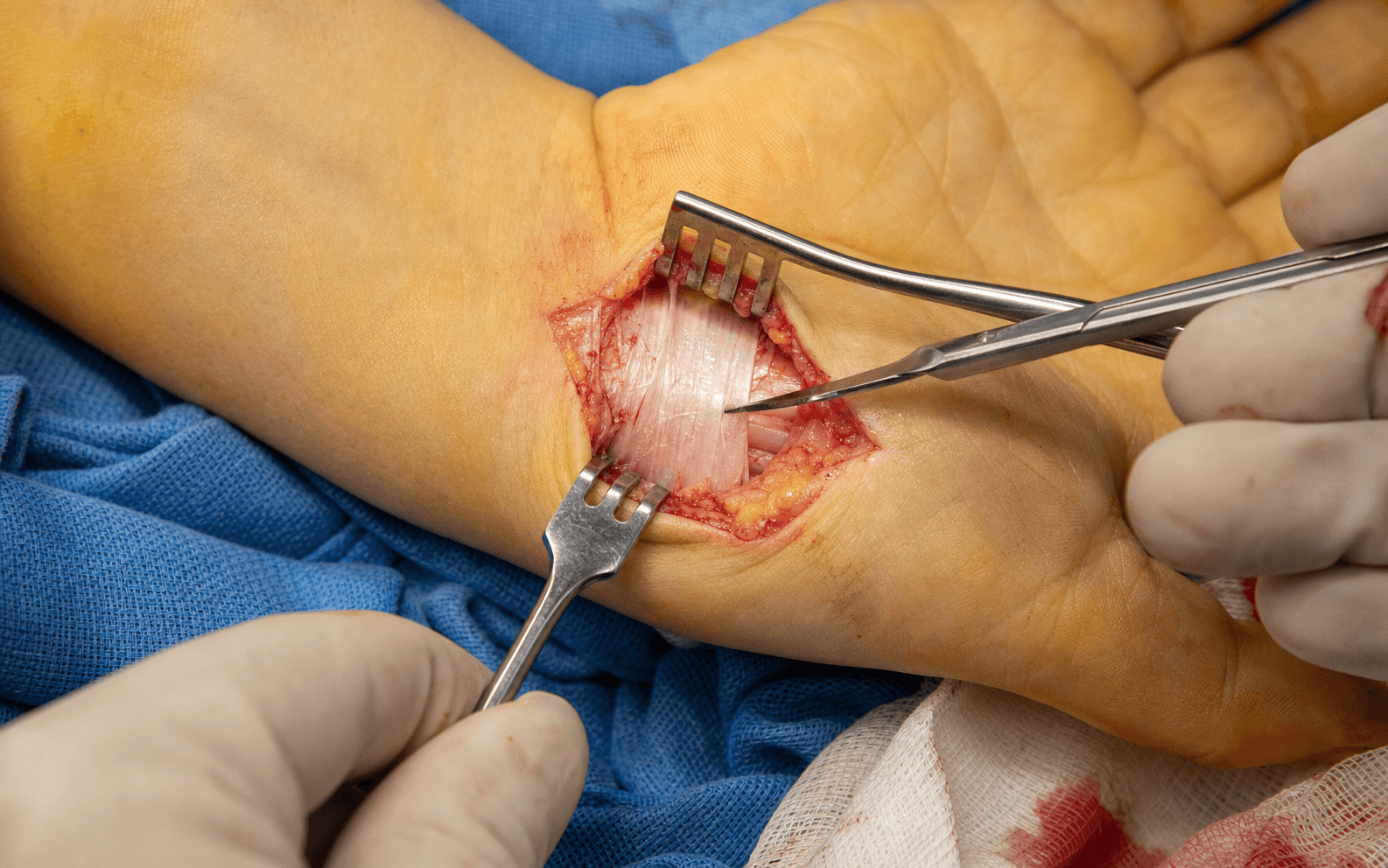
Division of the transverse carpal ligament through a ring-finger-axis palmar incision
- One incision line does most of the safety work: ring-finger axis, ULNAR to the thenar crease, from the distal wrist crease to Kaplan's cardinal line. This protects the palmar cutaneous branch, the thenar motor branch and the superficial palmar arch.
- Divide the transverse carpal ligament on the ULNAR side, 3-5mm from its radial edge, starting at the DISTAL edge (the fat pad) and working proximal over a grooved director. This protects the thenar motor branch in all three Lanz variants.
- Incomplete PROXIMAL release of the antebrachial fascia causes 30-40 percent of failures. Extend 1-2cm into the forearm and confirm the accordion sign of nerve expansion before closing.
- The TCL has TRANSVERSE fibres and the palmar aponeurosis has LONGITUDINAL fibres - two distinct layers divided sequentially. Never repair either, or you recreate the compression.
- Do NOT add internal neurolysis or epineurotomy. Mackinnon's 1991 randomised trial showed no benefit and potential harm from perineural scarring; simple division is sufficient.
- Pillar pain affects 30-40 percent of patients, peaks at 2-4 weeks and resolves in 90 percent by 3 months. It is self-limiting and must not push you toward repairing the TCL.
When & Why
Indication. Open carpal tunnel release decompresses the median nerve by dividing the transverse carpal ligament (the flexor retinaculum). It is offered for clinically and electrodiagnostically confirmed carpal tunnel syndrome that has either failed a fair trial of conservative care or has features that make surgery the first option. Absolute indications
- Thenar atrophy with electrodiagnostic confirmation of severe CTS.
- Constant numbness in the median distribution unresponsive to splinting.
- Acute carpal tunnel syndrome from trauma, bleeding or burns requiring urgent decompression. Relative indications
- Failed conservative management after 3-6 months (night splinting, activity modification, a corticosteroid injection).
- Moderate-severe CTS on nerve conduction studies (distal motor latency greater than 4.5ms, sensory latency greater than 3.5ms).
- Recurrent symptoms after initial conservative success, or patient preference for definitive treatment. Contraindications
- Absolute: active infection in the surgical field; severe medical comorbidities precluding safe anaesthesia; a patient unable to comply with postoperative care.
- Relative: mild CTS responsive to conservative treatment; pregnancy (usually defer until postpartum unless severe); severe CRPS in the limb; pending litigation (relative). Open or endoscopic? Both are valid; the choice is surgeon and patient dependent. The open technique is taught here because it gives direct visualisation, guarantees a complete release, has a low learning curve, and can deal with any anomalous anatomy (persistent median artery, bifid nerve, mass lesion). Endoscopic release offers a smaller scar, less early pillar pain and a faster return to work, at the cost of a steeper learning curve, no direct visualisation of the thenar branch, and a contraindication in revision or anomalous cases.
- Open (OCTR)
- 2-3cm palmar
- Endoscopic (ECTR)
- 1-2cm, single or two-portal
- Open (OCTR)
- Direct; complete release assured
- Endoscopic (ECTR)
- Indirect; thenar branch not seen
- Open (OCTR)
- Lower
- Endoscopic (ECTR)
- Higher
- Open (OCTR)
- More initially, 30-40%
- Endoscopic (ECTR)
- Less, around 20-30%
- Open (OCTR)
- 3-6 months
- Endoscopic (ECTR)
- 2-4 months
- Open (OCTR)
- 2-4 weeks
- Endoscopic (ECTR)
- 1-2 weeks
- Open (OCTR)
- 20-25%
- Endoscopic (ECTR)
- Less
- Open (OCTR)
- Fewer
- Endoscopic (ECTR)
- More (neurapraxia, paraesthesiae)
- Open (OCTR)
- Can address
- Endoscopic (ECTR)
- Cannot address
- Open (OCTR)
- Lower
- Endoscopic (ECTR)
- Higher (equipment)
- Open (OCTR)
- Preferred
- Endoscopic (ECTR)
- Contraindicated
- WALANT (wide-awake local anaesthesia, no tourniquet): 10ml of 1% lidocaine with 1:100,000 epinephrine injected 20-30 minutes before incision. The patient can actively move the fingers during the case, confirming a complete release and immediate symptomatic improvement. The historical fear of epinephrine causing finger necrosis has been debunked by modern evidence.
- Local anaesthesia with tourniquet: 1% lignocaine with 1:100,000 adrenaline, 5-10ml along the incision, with an upper-arm tourniquet at 250mmHg. Standard for most surgeons, giving a dry field.
- Regional block (axillary or supraclavicular): for anxious patients and longer postoperative analgesia; needs anaesthesia support.
- General anaesthesia: bilateral simultaneous cases, patient preference, or a medical condition requiring a controlled airway. Setup & positioning. Supine with the arm on a hand table, shoulder abducted 90 degrees (never more, to avoid brachial plexus stretch), elbow extended and forearm fully supinated. Upper-arm tourniquet (250mmHg), optional for WALANT. Standard hand tray: a number 15 blade, fine-toothed forceps, tenotomy scissors, a self-retaining retractor (Weitlaner or small Gelpi), a grooved director or MacDonald elevator, bipolar cautery, and 4-0 nylon or monocryl.
The Operation
The goal is to decompress the median nerve by completely dividing the transverse carpal ligament while protecting three structures at risk - the palmar cutaneous branch, the thenar motor branch and the superficial palmar arch - and to confirm that release visually before a skin-only closure. The exposure (the incision and the dissection down to the ligament) is laid out as the first steps below; it is the heart of the operation, and is described in full on the volar approach to the carpal canal page.
Operative sequence
- Mark three landmarks with the patient awake: Kaplan's cardinal line (apex of the thumb-index web to the hook of hamate, made prominent by wrist flexion and ulnar deviation) - the distal safe limit where the superficial palmar arch crosses; the ring-finger axis; and the thenar crease.
- Draw the incision: 2-3cm longitudinal, starting exactly AT the distal wrist crease (never proximal), extending distally along the ring-finger axis to Kaplan's line, staying 5mm ULNAR to the thenar crease.
- Position supine, arm abducted 90 degrees on the hand table, forearm fully supinated.
- For WALANT, infiltrate 10ml of 1% lidocaine with 1:100,000 epinephrine and wait the full 20-30 minutes for vasoconstriction before incising (the field is otherwise distorted by the local).
- If using a tourniquet, exsanguinate by elevation for 60 seconds and inflate to 250mmHg; keep tourniquet time under 90 minutes to avoid neuropraxia.
- Respect lignocaine dose limits: 4.5mg/kg plain, 7mg/kg with adrenaline.
- Incise sharply with a number 15 blade perpendicular to the skin, in the ring-finger axis, 5mm ulnar to the thenar crease, from the distal wrist crease to Kaplan's line.
- A single smooth stroke through epidermis and dermis to subcutaneous fat; handle edges gently with fine-toothed forceps on dermis only.
- Achieve skin-edge haemostasis with bipolar cautery on a low setting, tips kept away from deeper structures.
- Spread through subcutaneous fat with tenotomy scissors, dividing the vertical fibrous septa (retinacula cutis) that tether skin to fascia.
- Identify palmaris brevis crossing obliquely from the hypothenar side; divide it if it obscures the field (no functional consequence).
- Look here for an aberrant superficial thenar motor branch (2-3 percent run superficial to the TCL) before going deeper.
- Control superficial veins with bipolar or gentle retraction; deepen to the glistening palmar aponeurosis.
- Confirm the palmar aponeurosis: a glistening white triangular sheet with LONGITUDINAL fibres extending distally from palmaris longus. It is a SEPARATE layer, superficial to the TCL.
- Incise it longitudinally in the line of the skin incision for the full wound length, insert a self-retaining retractor, and bluntly separate it from the TCL beneath.
- Clear areolar tissue off the TCL: it is thick (2-3mm), glistening white, with TRANSVERSE fibres running radial-to-ulnar - the key distinction from the longitudinal aponeurosis.
- Identify the DISTAL edge by the fat pad - extrasynovial fat overlying the common digital neurovascular bundles where the ligament ends. This is the safest starting point for division.
- Palpate the transition from firm ligament to soft fat with an elevator to confirm the distal edge.
- Before dividing the TCL, inspect the distal edge and ligament surface for the recurrent motor branch.
- In the extraligamentous variant (46 percent) it exits distal to the TCL and runs radially; in the transligamentous variant (23 percent) it pierces THROUGH the ligament and may be visible on its surface.
- If seen, note its exact position. Regardless of variant, you will divide on the ulnar side, so the branch is protected.
- Under direct vision, make a small 3-5mm longitudinal cut in the TCL at the distal edge, on the ULNAR side (3-5mm from the radial edge).
- Pass a grooved director (Freer/MacDonald) through this opening from distal to proximal, deep to the TCL, groove facing superficially, so the blade will ride in the groove away from the median nerve immediately beneath.
- Confirm smooth glide in the correct plane; if you meet resistance, withdraw and reposition - never force.
- With the director firmly protecting the nerve, divide the TCL longitudinally from distal to proximal, the blade tip riding in the director groove.
- Keep the division on the ulnar side, 3-5mm from the radial edge, throughout - this protects all three motor branch variants.
- Maintain the director in place the whole time; do not remove it until the division is complete along the full 2-3cm length, to where the TCL becomes the antebrachial fascia.
- The nerve should appear pink-white with a visible fascicular pattern as the edges separate.
- Visualise: the fat pad; the common digital nerves branching from the median nerve about 1-2cm distal to the old TCL edge; and the superficial palmar arch crossing roughly 2-3cm distal.
- Divide any remaining distal fascial bands or aponeurotic fibres under direct vision - residual bands cause persistent compression.
- Do NOT dissect beyond Kaplan's cardinal line (the arch crosses here; further dissection risks vascular injury and digital ischaemia).
- The antebrachial fascia is continuous with the TCL proximally and is the commonest site of incomplete release. If tight, extend the release 1-2cm into the forearm fascia under direct vision, on the ulnar side.
- Perform the accordion test: gently compress the median nerve with an elevator and release - it should visibly expand like accordion bellows. Absence of expansion means persistent compression; keep extending until you see it.
- Avoid extending more than 2-3cm proximally (no benefit, more morbidity) and never extend proximally AND radially (palmar cutaneous branch territory).
- Confirm the hourglass constriction at the compression site (correct level decompressed) and look for proximal pseudoneuroma swelling in longstanding severe CTS.
- Check colour (pink-white is viable; brown suggests ischaemia) and the fascicular pattern through the epineurium.
- Exclude space-occupying lesions - persistent median artery (5-10 percent, may be thrombosed), bifid median nerve (2 percent), anomalous muscles, ganglia, lipomas, gout tophi.
- Do NOT perform internal neurolysis or epineurotomy - Mackinnon's 1991 RCT showed no benefit and potential harm. Simple division is sufficient; the nerve remodels over 3-12 months.
- Release the tourniquet and wait 2-3 minutes for reactive hyperaemia to peak so every potential bleeder declares itself.
- Systematically cauterise superficial arch branches distally, TCL-edge vessels, skin-edge and subcutaneous bleeders with bipolar on a low setting.
- Keep cautery tips at least 5mm from the median nerve and the thenar branch to avoid thermal neuropraxia. A dry field prevents haematoma, which causes pain, delays recovery and can recompress the nerve.
- Close SKIN ONLY: 4-0 nylon interrupted or vertical mattress (5-6 sutures for a 2-3cm wound, removed at 10-14 days), or 4-0 monocryl subcuticular for better cosmesis.
- Do NOT repair the palmar aponeurosis. Do NOT repair or reconstruct the TCL - that recreates the compression and increases recurrence.
- The TCL remnant edges gradually separate 5-8mm with wrist motion over the following weeks, maintaining decompression permanently.
- In acute CTS (trauma, compartment syndrome) some surgeons leave the skin open for delayed closure at 3-5 days.
- Apply a non-adherent dressing, bulky soft gauze, and a crepe bandage from fingertips to mid-forearm for gentle compression, with the wrist in neutral (avoid forced dorsiflexion).
- Splinting is OPTIONAL - modern evidence shows routine splinting gives no benefit and increases stiffness.
- Encourage immediate full finger range of motion (fist-making hourly) from day 1, wrist motion from day 3-5, light hand use straight away, and elevation above the heart for 48 hours.
- Avoid heavy gripping or direct palm pressure for 4-6 weeks (worsens pillar pain). Remove sutures at 10-14 days.
Across the whole operation three structures define your safety. The palmar cutaneous branch (median nerve, 5cm proximal to the wrist, between FCR and palmaris longus, superficial to the TCL) is protected by never extending the incision proximal to the wrist crease. The thenar motor branch (radial side of the median nerve, 1cm distal to the TCL edge, with the three Lanz variants) is protected by dividing the TCL on the ulnar side 3-5mm from the radial edge. The superficial palmar arch (crossing 2-3cm distal to the TCL at Kaplan's line) is protected by never dissecting beyond Kaplan's cardinal line. Get these three right and the serious complications are essentially eliminated.
The median nerve lies immediately deep (0mm) to the TCL and may be adherent to its undersurface in chronic severe or revision cases. Every millimetre of TCL division is made over a grooved director slid deep to the ligament, groove facing up, so the blade rides in the groove away from the nerve. Blind cuts, or cutting without the director in place, are how median nerve lacerations (0.1-0.3 percent) happen - the one devastating complication of this operation.
Incomplete proximal release of the antebrachial fascia is the single commonest technical error, causing 30-40 percent of failures. After dividing the TCL, extend 1-2cm into the forearm fascia, then gently compress the median nerve with an elevator and release: it should visibly expand like accordion bellows opening. If it does not, you have not released enough - extend further until the accordion sign appears. Then palpate the whole course of the nerve for any residual constricting band.
Do not repair or reconstruct the TCL, and do not close the palmar aponeurosis. Repairing the TCL recreates the stenosis, increases recurrence dramatically, and is the wrong answer in any exam. The remnant edges separate 5-8mm with wrist motion and stay apart - that permanent separation IS the decompression. Older techniques advocating TCL repair to prevent bowstringing are outdated and contraindicated.
In a cooperative patient, WALANT lets you watch active finger movement at the end of the case - confirming a complete TCL release and demonstrating immediate symptomatic improvement before the patient leaves the table. Epinephrine in the hand is safe (the necrosis fear is a myth), there is no tourniquet discomfort, and the case suits an outpatient setting.
Aftercare & Complications
Rehabilitation | Phase | Timing | Activity | |-------|--------|----------| | Immediate | 0-2 weeks | Bulky dressing 3-5 days, then lighter. No routine splint. Immediate full finger ROM hourly; wrist ROM from day 3-5; light ADLs (eating, grooming, typing); elevation above heart 48h; avoid heavy grip or palm pressure; sutures out 10-14 days | | Early | 2-6 weeks | Scar massage from 3 weeks (5 minutes, three times daily); progressive wrist ROM; gentle putty strengthening from 3-4 weeks; return to desk work 1-2 weeks; avoid heavy manual work | | Intermediate | 6 weeks-3 months | Progressive strengthening; return to manual work at 6 weeks if tolerated; pillar pain resolving (90 percent by 3 months); grip still 10-20 percent down | | Long-term | 3-12 months | Thenar strength recovers gradually (permanent deficit in 20 percent of severe preoperative atrophy); grip returns to baseline by 6-12 months; scar matures by 6-12 months | Expected recovery timeline
- Night symptoms: resolve within days to 2 weeks in 95 percent.
- Daytime numbness: improves over 4-8 weeks, complete resolution in 85 percent by 3 months.
- Pillar pain: present in 30-40 percent, peaks 2-4 weeks, resolves in 90 percent by 3 months and 95 percent by 6 months.
- Grip strength: reduced 10-20 percent for 3-6 months, back to baseline by 6-12 months.
- Thenar strength: gradual recovery over 3-12 months; permanent weakness in about 20 percent of severe preoperative atrophy.
- Return to desk work 1-2 weeks; manual work 4-6 weeks; unrestricted activities 6-12 weeks. Success rates. Primary surgery gives 85-95 percent excellent or good results at one year (95 percent in mild-moderate CTS, 70-80 percent in severe CTS with atrophy where 20 percent have permanent thenar weakness). Revision surgery succeeds in 60-75 percent. Poor-outcome predictors include severe preoperative thenar atrophy, diabetes, a workers' compensation claim, symptoms lasting more than 10 months, age greater than 50, bilateral severe disease, and cervical radiculopathy (double crush).
- Recognition
- Thenar/hypothenar tenderness at the cut TCL edges, worse with grip or palm pressure, onset 1-2 weeks, peaks 2-4 weeks
- Prevention
- No proven prevention; complete TCL division, no TCL repair, early mobilisation
- Management
- Reassure (self-limiting), activity modification, padded grips, desensitisation massage, NSAIDs; 90% resolved by 3 months, 95% by 6 months; steroid injection for the rare persistent case
- Recognition
- Persistent night symptoms and numbness, positive provocative tests, electrodiagnostic persistence, MRI showing unreleased proximal fascia or distal bands
- Prevention
- Divide proximal antebrachial fascia 1-2cm, visualise the fat pad and digital nerves, confirm the accordion sign, divide all distal aponeurotic bands
- Management
- Revision via an extended approach dividing the unreleased fascia; 60-75% success versus 95% primary; address any scar neuroma
- Recognition
- Tender raised scar, pain on palpation or grip, possible adherent scar, Tinel over the scar
- Prevention
- Do not cross the wrist crease proximally; meticulous skin handling; early scar massage from 3 weeks
- Management
- Scar massage, desensitisation, silicone sheeting, steroid injection for hypertrophic scar; excision and Z-plasty if neuroma confirmed; palmaris brevis flap for coverage
- Recognition
- Immediate loss of median sensation and thenar paralysis, recognised visually if intraoperative
- Prevention
- Grooved director deep to the TCL throughout; start at the distal edge under direct vision; never cut blind
- Management
- Immediate epineural repair with 8-0 nylon under magnification, splint 3 weeks, therapy; delayed cases need exploration with neurorrhaphy or cable graft; recovery 50-70% sensation, 40-60% motor
- Recognition
- Thenar weakness (opposition, abduction); EMG/NCS at 6 weeks separates neuropraxia from neurotmesis
- Prevention
- Divide the TCL on the ulnar side 3-5mm from the radial edge; inspect for the transligamentous variant; avoid cautery near the radial edge; gentle retraction
- Management
- Traction injury: observe 3-6 months with therapy (60-80% recover); laceration: immediate repair or graft; tendon transfer (EPL/ECRL rerouting, FDS ring opponensplasty) if no recovery
- Recognition
- Immediate arterial bleeding, haematoma, rarely digital ischaemia (check capillary refill and Allen test)
- Prevention
- Mark Kaplan's line preoperatively; limit distal dissection to the fat pad; never extend beyond Kaplan's line
- Management
- Bipolar cautery (away from nerves) or ligation; check digit perfusion; if ischaemic, immediate microsurgical exploration and repair or vein graft
- Recognition
- Painful thenar neuroma, Tinel over the proximal scar, hypersensitivity of thenar skin worse than the preoperative CTS
- Prevention
- Never extend the incision proximal to the wrist crease; start at the crease in the ring-finger axis 5mm ulnar to the thenar crease
- Management
- Desensitisation, gabapentin/pregabalin, steroid injection around the neuroma; surgical excision with burial into pronator quadratus or relocation to a deeper plane
- Recognition
- Erythema, warmth, purulent drainage, fever, cellulitis spreading proximally; rarely abscess or septic flexor tenosynovitis
- Prevention
- Meticulous sterile technique; single-dose prophylactic antibiotic only for high-risk patients (routine prophylaxis does not reduce SSI in clean release); haemostasis
- Management
- Superficial cellulitis: oral cephalexin or dicloloxacin for 7-10 days; deep infection/abscess: washout, debridement, IV flucloxacillin, culture-directed therapy; septic tenosynovitis needs urgent washout
- Recognition
- Excessive swelling, ecchymosis, tense painful wound, rarely recurrent numbness from nerve recompression
- Prevention
- Meticulous haemostasis after tourniquet release; bipolar all bleeders; bulky compressive dressing
- Management
- Small: observe, elevate, ice, compress; large or tense: return to theatre for evacuation, identify the source, confirm the nerve is not compressed
- Recognition
- Severe disproportionate pain, swelling, vasomotor changes, allodynia, stiffness, skin/nail changes
- Prevention
- Atraumatic technique, early mobilisation, adequate analgesia, vitamin C 500mg daily perioperatively, avoid excessive splinting
- Management
- Early recognition; aggressive hand therapy (stress loading, desensitisation, ROM); gabapentin, neuropathic agents; stellate ganglion block; pain specialist referral; best if treated within 3 months
- Recognition
- Visible/palpable tendon prominence with finger flexion, possible pain or mechanical symptoms, reduced grip
- Prevention
- Standard TCL division (no wide excision); never repair the TCL; the normal post-division gap is 5-8mm
- Management
- Usually asymptomatic; if symptomatic with weakness, rare TCL reconstruction with palmaris longus graft or FCR strip to restore the pulley
- Recognition
- Return of symptoms after initial improvement, positive provocative tests, electrodiagnostic confirmation
- Prevention
- Complete initial release (proximal fascia and distal bands); no TCL repair; avoid haematoma/infection; early mobilisation
- Management
- Confirm true recurrence versus incomplete release, new pathology or cervical radiculopathy; revision via extended approach, lyse scar, complete any reformed TCL, consider vein wrapping; 60-75% good/excellent
Viva & Exam Focus
RING-URING-U - the incision landmarks
FAT-PADFAT-PAD - safe TCL division
Branches from the median nerve 5cm proximal to the wrist crease, passes between FCR and palmaris longus, runs superficial to the TCL to the thenar skin. Protection: start the incision AT the wrist crease (never proximal), stay in the ring-finger axis 5mm ulnar to the thenar crease.
Branches from the radial side of the median nerve about 1cm distal to the TCL edge. Three Lanz variants: extraligamentous 46%, subligamentous 31%, transligamentous 23% (pierces the TCL). Protection: divide the TCL on the ulnar side 3-5mm from the radial edge, inspect for the transligamentous variant, avoid cautery near the radial edge.
Crosses the palm 2-3cm distal to the TCL at Kaplan's cardinal line (thumb-index web apex to hook of hamate), formed by the ulnar artery with variable median/radial contribution. Protection: mark Kaplan's line preoperatively, limit distal dissection to the fat pad, never extend beyond Kaplan's line.
Lies immediately deep to the TCL, may show an hourglass constriction at the compression site, and can be adherent to the ligament undersurface in chronic severe or revision cases. Protection: grooved director deep to the TCL throughout division, start at the distal edge under direct vision, never cut blind.
Branch from the median nerve 1-2cm distal to the TCL edge toward the thumb, index, long and radial ring fingers, lying deep to the superficial arch. Protection: limit distal dissection to the fat pad, visualise the branching nerves to confirm release, avoid aggressive distal exploration beyond Kaplan's line.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the anatomical variants of the thenar motor branch and explain how you protect it during open carpal tunnel release.”
“Incomplete release is the most common cause of persistent symptoms after carpal tunnel surgery. Explain why this occurs and describe how you ensure complete release during the operation.”
“Pillar pain is the most common postoperative complaint after carpal tunnel release. Explain its pathophysiology, natural history and evidence-based management.”
Indications
- Absolute: thenar atrophy with severe CTS on EMG/NCS, constant numbness unresponsive to splinting, acute CTS from trauma or bleeding needing urgent decompression
- Relative: failed conservative care after 3-6 months, moderate-severe CTS on electrodiagnostics (DML greater than 4.5ms, sensory latency greater than 3.5ms)
- Contraindications: active infection, severe comorbidity precluding anaesthesia, mild CTS responsive to conservative care
Key anatomy
- Palmar cutaneous branch: 5cm proximal to the wrist between FCR and PL, superficial to the TCL, thenar skin - injured if the incision crosses the wrist crease (2-3% neuroma)
- Thenar motor branch variants (Lanz): extraligamentous 46%, subligamentous 31%, transligamentous 23% - protected by ulnar-sided division
- Superficial palmar arch: crosses 2-3cm distal to the TCL at Kaplan's line - never dissect beyond it
- TCL: 2-3cm long, 2-3mm thick, transverse fibres (versus the longitudinal aponeurosis), median nerve immediately deep, continuous with the antebrachial fascia proximally
Critical steps
- Incision: ring-finger axis, 5mm ulnar to the thenar crease, 2-3cm from the wrist crease to Kaplan's line
- Identify the distal TCL edge by the fat pad - the safest start point
- Divide the TCL distal-to-proximal on the ulnar side (3-5mm from the radial edge) over a grooved director
- Extend 1-2cm into the antebrachial fascia - incomplete proximal release causes 30-40% of failures
- Confirm with the fat pad and digital nerves distally plus the accordion test
- Close skin only - NEVER repair the TCL or aponeurosis
Danger zones
- Palmar cutaneous branch (5cm proximal to the wrist) - no proximal extension beyond the wrist crease
- Thenar motor branch (radial TCL edge, 1cm distal) - divide on the ulnar side 3-5mm from the radial edge
- Superficial palmar arch (Kaplan's line, 2-3cm distal) - never dissect beyond Kaplan's line
- Median nerve (0mm deep to the TCL) - grooved director throughout
- Digital nerves (1-2cm distal) - visualise but do not dissect aggressively
Technique pearls
- FAT-PAD: Find distal edge, Avoid starting proximally, Transverse fibres, Protect with director, Advance distal-to-proximal, Divide antebrachial fascia
- RING-U: Ring-finger axis, Incision 2-3cm, Never cross wrist crease, Gap from thenar crease, Ulnar-side division
- Accordion test mandatory - compress then release the nerve, visible expansion confirms complete release
- TCL transverse fibres versus palmar aponeurosis longitudinal fibres - separate layers divided sequentially
- Start at the distal edge and work proximal over the grooved director
- WALANT allows active finger motion to confirm release - epinephrine is safe in the hand
Complications
- Pillar pain (30-40%): most common, peaks 2-4 weeks, 90% resolved by 3 months - reassurance, activity modification, NSAIDs
- Incomplete release (30-40% of failures): inadequate proximal fascia or distal bands - prevent with the accordion test, 1-2cm proximal extension, fat-pad visualisation
- Median nerve injury (0.1-0.3%): grooved director, distal-to-proximal, immediate repair if recognised
- Thenar branch injury (0.5-1%): ulnar-sided division 3-5mm from the radial edge; tendon transfer if permanent
- Scar tenderness (20-25%): scar massage from 3 weeks, no proximal extension beyond the wrist crease
- Haematoma (2-5%): meticulous haemostasis after tourniquet release
Post-op protocol
- Immediate: bulky dressing 3-5 days, no routine splinting, elevation 48h, immediate finger ROM hourly
- Week 1-2: wrist ROM from day 3-5, light ADLs, avoid heavy grip, sutures out 10-14 days
- Week 3-6: scar massage from 3 weeks, progressive ROM, gentle putty from 3-4 weeks, desk work at 1-2 weeks
- Week 6-12: manual work at 6 weeks, pillar pain resolving by 3 months, grip 10-20% down until 3-6 months
- Timeline: night symptoms resolve within days; daytime numbness 85% resolved by 3 months; grip baseline by 6-12 months
Exam tips
- Open with the incision landmarks: ring-finger axis, 5mm ulnar to the thenar crease, wrist crease to Kaplan's line
- Give the three thenar branch variants with percentages and the ulnar-sided protection strategy
- Emphasise incomplete PROXIMAL release as the commonest failure (30-40%) and the accordion test
- NEVER suggest TCL repair or reconstruction - it increases recurrence and negates the decompression
- Counsel pillar pain: 30-40%, peaks 2-4 weeks, 90% resolved by 3 months
- Mackinnon 1991: internal neurolysis gives no benefit (potential harm) - simple TCL division is enough
- AAOS / NICE-BOA / EFORT agree: complete TCL division alone is standard; routine antibiotics and routine splinting are NOT recommended
Background & Evidence
Epidemiology. Carpal tunnel syndrome is the commonest compressive neuropathy of the upper limb worldwide. In a general-population survey of 2,466 responders (Atroshi, JAMA 1999), symptoms in the median distribution were present in 14.4 percent, clinically certain CTS in 3.8 percent and electrophysiological median neuropathy in 4.9 percent, giving a prevalence of clinically AND electrophysiologically confirmed CTS of 2.7 percent (95 percent CI 2.1-3.4) - roughly one in five symptomatic individuals has confirmed disease. There is a female predominance, a peak incidence at 40-60 years, and associations with obesity, diabetes, hypothyroidism, pregnancy, rheumatoid arthritis and repetitive or vibratory hand use. Anatomy of the carpal tunnel.
- Floor (dorsal): distal radius articular surface; scaphoid and lunate proximally; trapezium, trapezoid and capitate distally.
- Roof (volar): the transverse carpal ligament (flexor retinaculum) - a thick fibrous band 2-3cm long and 2-3mm thick, attaching to the scaphoid tubercle and trapezium radially and the pisiform and hook of hamate ulnarly.
- Walls: radial - scaphoid tubercle and trapezial ridge; ulnar - pisiform and hook of hamate.
- Contents: nine flexor tendons (flexor pollicis longus radially; four superficialis in a middle layer; four profundus deep) and the median nerve, which enters superficial and radial to the tendons and is the most superficial structure beneath the TCL - the structure compressed against the rigid roof in wrist flexion. Critical neural anatomy. The palmar cutaneous branch arises from the median nerve in the distal forearm 5cm proximal to the wrist crease, emerges between FCR and palmaris longus, passes superficial to the TCL and supplies the thenar skin - injured if the incision crosses the wrist crease. The thenar (recurrent motor) branch arises from the radial side of the median nerve about 1cm distal to the TCL edge and supplies abductor pollicis brevis, opponens pollicis and the superficial head of flexor pollicis brevis. The common digital nerves branch 1-2cm distal to the TCL, lie deep to the superficial palmar arch, and are visible at the base of the fat pad. Vascular anatomy. The superficial palmar arch crosses the palm 2-3cm distal to the TCL at Kaplan's cardinal line, formed by the ulnar artery with variable contributions from the median artery (5 percent) and radial artery (35 percent). A persistent median artery is present in 5-10 percent of people, travels with the median nerve through the tunnel, and can thrombose to cause acute CTS. Surface landmarks. Kaplan's cardinal line runs from the apex of the thumb-index web space to the hook of hamate and marks the superficial palmar arch (the distal safe-dissection limit). The thenar crease is the boundary between the thenar eminence and the palm; the incision stays 5mm ulnar to it. The ring-finger axis is the longitudinal line for the skin incision, avoiding the motor branch radially and the hypothenar neurovascular structures ulnarly. Classification - thenar motor branch variants (Lanz 1977). Lanz's overall scheme has four groups: Group I variations in the thenar branch course; Group II accessory distal branches; Group III high division of the median nerve; Group IV accessory proximal branches. The surgically critical Group I course (from Poisel's cadaver data) is:
- Frequency
- 46%
- Course
- Branches distal to the TCL and recurves around its distal edge to the thenar muscles
- Surgical implication
- Protected by ulnar-sided division
- Frequency
- 31%
- Course
- Arises beneath the TCL and exits at the distal edge
- Surgical implication
- Protected by ulnar-sided division
- Frequency
- 23%
- Course
- Pierces through the substance of the TCL (highest intra-operative risk)
- Surgical implication
- Identify before cutting; ulnar-sided division
- Frequency
- Rare
- Course
- Runs superficial to the TCL
- Surgical implication
- Look for it in the subcutaneous plane before going deep
Classification - severity (surgical perspective).
- Clinical / electrodiagnostic picture
- Normal examination, positive Phalen/Tinel, intermittent night symptoms
- Usual management
- Conservative - splint, activity modification, injection
- Clinical / electrodiagnostic picture
- Sensory change, no thenar weakness, positive nerve conduction studies
- Usual management
- Surgical candidate after failed conservative care
- Clinical / electrodiagnostic picture
- Thenar atrophy, constant numbness, severe electrodiagnostic change
- Usual management
- Absolute surgical indication
Guidelines, registries and global practice. | Body | Position | |------|----------| | AAOS (US) | Strong evidence that surgery is superior to non-operative care; recommends AGAINST routine adjuncts (internal neurolysis, epineurotomy, tenosynovectomy); routine post-op splinting not recommended | | NICE / BOA (UK) | Surgical decompression for confirmed moderate-severe CTS or failed conservative care; injection as a temporising option; simple complete release | | EFORT / European consensus | Complete division of the flexor retinaculum as definitive treatment; open and endoscopic equivalent for symptom relief | | AAHS / IFSSH | Endorse both open and endoscopic release; reserve endoscopic for surgeons with appropriate training; open preferred in revision or anomalous anatomy | This is a soft-tissue nerve decompression and is NOT captured by arthroplasty registries (NJR, AJRR, AOANJRR, SHAR). Antibiotic prophylaxis is NOT routinely indicated for clean elective release - meta-analysis shows no reduction in surgical-site infection; reserve antibiotics for high-risk patients (e.g. diabetes, immunosuppression) per local stewardship policy. Anaesthesia ranges from WALANT in office settings to local-plus-tourniquet, regional block or general anaesthesia by resource setting, and endoscopic uptake varies by region with equipment cost and training. Key evidence. Surgery is superior to splinting (Gerritsen 2002 RCT: surgery 80 percent versus splinting 54 percent success at 3 months, and 90 percent versus 75 percent at 18 months). Open and endoscopic release are equivalent for symptom relief and function (Vasiliadis 2014 Cochrane review), with endoscopic giving an earlier return to work. Internal neurolysis adds no benefit (Mackinnon 1991 RCT) and should not be performed. Local steroid injection gives useful but temporary relief and is mainly a diagnostic and temporising tool. Major societies (AAOS, NICE/BOA, EFORT) converge on the same message: complete TCL division alone is the global standard of care.
References
Splinting vs surgery in the treatment of carpal tunnel syndrome: a randomized controlled trial
- Multicentre RCT, 176 patients with electrophysiologically confirmed idiopathic CTS, randomised to night splinting or open carpal tunnel release
- Surgery success 80% vs splinting 54% at 3 months (difference 26%, 95% CI 12-40%)
- At 18 months surgery 90% vs splinting 75% (difference 15%, 95% CI 3-27%)
- 41% of the splint group had crossed over to surgery by 18 months
Endoscopic release for carpal tunnel syndrome (Cochrane systematic review)
- 28 studies, 2,586 hands, comparing endoscopic (ECTR) with open (OCTR) release
- No difference in symptom relief or functional status at 3 months or beyond (low-quality evidence)
- Return to work was on average 8 days earlier after endoscopic release
- Fewer minor complications with ECTR (more transient nerve symptoms) but no difference in major complications, recurrence or reoperation
Internal neurolysis fails to improve the results of primary carpal tunnel decompression
- Prospective RCT, 63 hands: TCL release alone vs release plus internal neurolysis of the median nerve
- Symptom relief 88% (release alone) vs 81% (release plus neurolysis) - no significant difference
- No difference in sensibility, thenar strength or atrophy between groups
- Adding internal neurolysis confers no benefit and risks perineural scarring
Anatomical variations of the median nerve in the carpal tunnel
- 246 operatively explored hands plus pooled cadaver data; basis of the Lanz classification of median nerve variants
- Thenar (recurrent motor) branch course (Poisel data): extraligamentous 46%, subligamentous 31%, transligamentous 23%
- Four groups described: thenar branch variation, accessory distal branches, high median nerve division, accessory proximal branches
- Emphasises approaching the median nerve and dividing the TCL from the ULNAR side
Prevalence of carpal tunnel syndrome in a general population
- Population survey of 2,466 responders in southern Sweden with clinical and nerve conduction confirmation
- Symptoms in median distribution 14.4%; clinically certain CTS 3.8%; electrophysiological median neuropathy 4.9%
- Clinically AND electrophysiologically confirmed CTS prevalence 2.7% (95% CI 2.1-3.4%)
- Roughly 1 in 5 symptomatic individuals have confirmed CTS
Management of Carpal Tunnel Syndrome - Evidence-Based Clinical Practice Guideline
- Strong evidence that surgical TCL release relieves symptoms and improves function more than non-operative treatment
- Strong recommendation against routine adjunctive procedures (internal neurolysis, epineurotomy, flexor tenosynovectomy) at primary release
- Routine post-operative wrist splinting is not recommended after release
- NICE/BOA-aligned UK practice and EFORT consensus concur: simple complete decompression is the standard of care