Ring finger axis incision | PCBMN + recurrent branch protection | TCL division under vision
- Incision ulnar to the thenar crease along the radial border of the ring finger axis protects the palmar cutaneous branch of the median nerve.
- Recurrent motor branch - identify and protect at the distal TCL edge (extraligamentous, subligamentous or transligamentous variants).
- Divide the TCL under direct vision from proximal to distal - never blindly; protect the median nerve and flexor tendons.
- Superficial palmar arch lies 1-2 cm distal to the TCL distal edge; identify it before any distal dissection.
- No true internervous plane - dissection passes between thenar and hypothenar territories, but both median and ulnar nerves supply the thenar muscles.
When & Why
What it exposes. The volar palmar (flexor) approach gives direct access to the carpal tunnel contents, the transverse carpal ligament (flexor retinaculum), the median nerve throughout its course in the hand, the flexor tendons in zones 3 and 4, and the mid-palmar space. It allows complete division of the flexor retinaculum under direct vision, inspection of the median nerve for hourglass constriction or tenosynovitis, and safe extension into the mid-palm while protecting the superficial palmar arch. No other single incision gives equivalent access to both the carpal canal and the mid-palmar flexor apparatus. Primary indications: - Open carpal tunnel release for idiopathic or secondary carpal tunnel syndrome
- Flexor tendon exploration and repair in zones 3 and 4 (mid-palm)
- Drainage of mid-palmar space infections and deep palmar abscesses
- Excision of mid-palmar masses (ganglia, lipomas, giant cell tumours of tendon sheath)
- Release of Dupuytren contracture involving the mid-palm
- Revision carpal tunnel surgery with nerve reconstruction or tenosynovectomy
- Combined procedures requiring access to both carpal tunnel and mid-palm Why this approach. It is the gold standard for open carpal tunnel release with direct nerve inspection, and it allows simultaneous access to carpal tunnel and mid-palmar pathology. The transverse carpal ligament is divided under direct vision, the median nerve is inspected, and the incision extends safely proximally into the forearm and distally along the flexor sheaths. Contraindications and alternatives. Active infection at the planned incision site, severe thenar wasting with fixed contracture, or a known high-risk transligamentous recurrent motor branch may favour an alternative strategy. Options include endoscopic carpal tunnel release (faster recovery, limited nerve visualisation, no mid-palm access), limited open (mini-incision) release (smaller scar, limited exposure for complex pathology), an extended carpal tunnel approach with forearm extension (for proximal median nerve pathology or Volkmann contracture), and combined volar and dorsal approaches for complex trauma involving both flexor and extensor surfaces. Position and landmarks. Supine, arm abducted 90 degrees on a hand table, upper-arm tourniquet at about 250 mmHg (or a forearm tourniquet for distal procedures), palm up, with loupe magnification (2.5x or 3.5x) and a headlight; a microscope is available if nerve reconstruction or complex tendon work is anticipated. WALANT (wide-awake local anaesthesia no tourniquet) allows intra-operative flexor tendon testing and is increasingly used globally. Palpable bony landmarks are the pisiform (TCL ulnar attachment), the hook of hamate (1 cm distal and radial to the pisiform), the scaphoid tubercle and the trapezium ridge (TCL radial attachments). Soft-tissue landmarks are the thenar crease (radial boundary - stay ulnar to it), the distal wrist crease (proximal limit), Kaplan cardinal line (hook of hamate to the radial border of the index MCP, near which the recurrent motor branch emerges), and the palpable flexor carpi radialis and palmaris longus tendons (palmaris longus is present in 80-85 percent of individuals).
Tourniquet time should be limited to less than 120 minutes when possible and always documented. The median nerve is already compressed in carpal tunnel syndrome, so minimise additional ischaemic time. In revision cases or severe compression, consider tourniquet-free WALANT surgery with local anaesthetic and adrenaline infiltration.
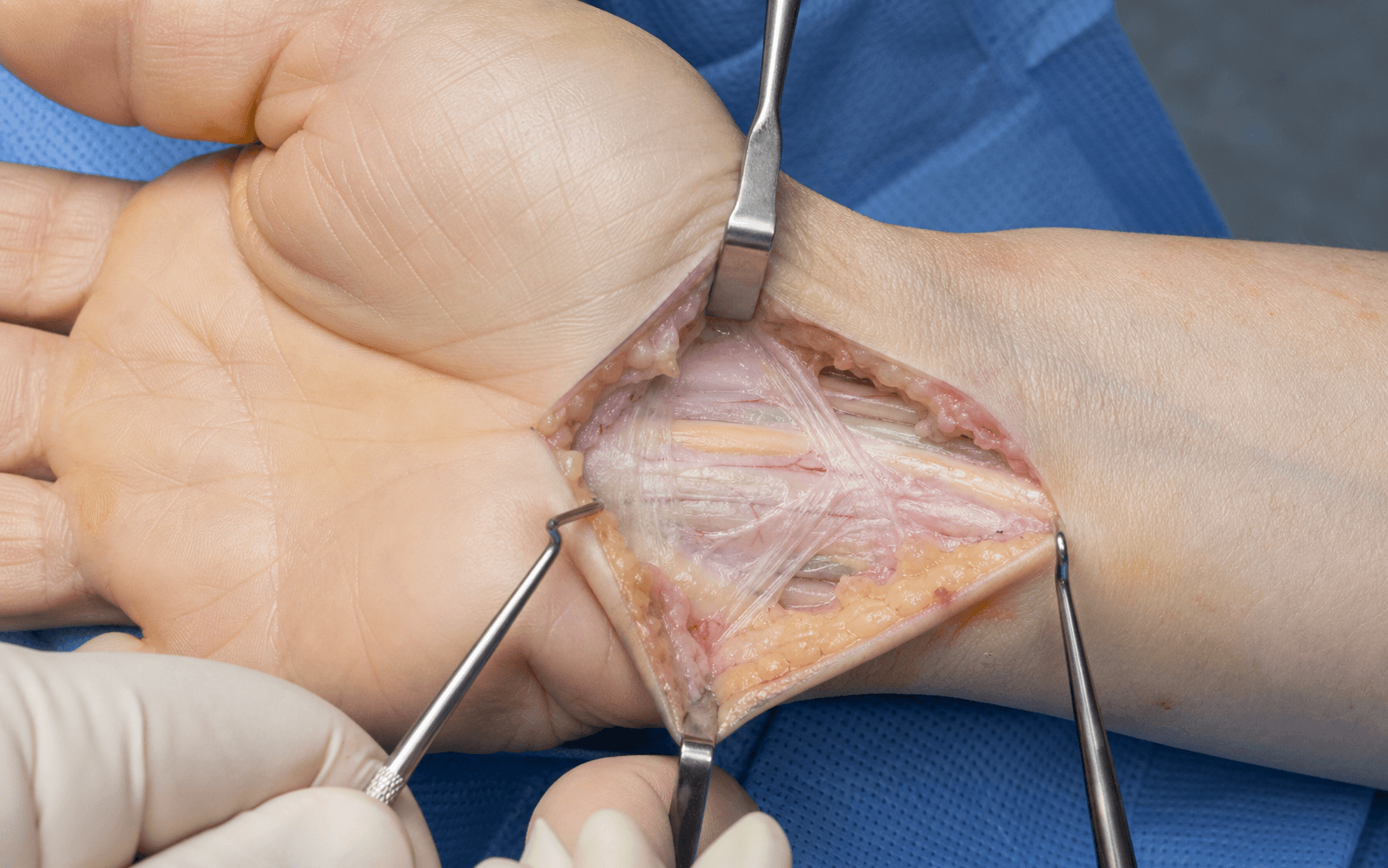
The Exposure
Work down through the layers along the radial border of the ring finger axis, protecting the palmar cutaneous branch and the recurrent motor branch, then divide the transverse carpal ligament under direct vision to deliver the median nerve. The superficial palmar arch is the gatekeeper to the mid-palm and must be visualised before any distal extension.
Exposure sequence
- A longitudinal incision along the radial border of the ring finger axis, beginning at the distal wrist crease and extending 4-6 cm distally into the mid-palm.
- Kept strictly ulnar to the thenar crease throughout to protect the palmar cutaneous branch of the median nerve; a gentle zig-zag at the wrist crease prevents contracture.
- Incise skin and subcutaneous fat and identify the palmar cutaneous branch of the median nerve (PCBMN) as it emerges 5-6 cm proximal to the wrist crease between palmaris longus and flexor carpi radialis.
- It travels superficial to the TCL - retract it radially and gently throughout; it is the structure most often injured.
- Incise the palmar aponeurosis longitudinally in line with the skin incision, exposing the FCR tendon radially and palmaris longus ulnarly.
- The TCL is now visible as a thick, glistening white structure.
- Identify the proximal edge of the TCL near the pisiform and gently define the distal edge to find the recurrent motor branch of the median nerve.
- Note its variant: extraligamentous (most common, 50-60 percent), subligamentous (30-40 percent), or transligamentous (20-30 percent, pierces the TCL - highest risk during division).
- Pass a small elevator or probe beneath the TCL from proximal to distal to protect the median nerve and flexor tendons.
- Divide the TCL from proximal to distal with the cutting edge directed dorsally and ulnarly - never blindly - and continue until the distal edge is completely released.
- Inspect the median nerve for hourglass constriction, tenosynovitis or residual compressive bands; perform tenosynovectomy if indicated.
- Confirm the nerve is completely free throughout the carpal tunnel and document its appearance.
- Before any distal extension, identify the superficial palmar arch approximately 1-2 cm distal to the TCL distal edge, usually a pulsating vessel that can be palpated.
- This is the critical distal danger structure - protect it before incising the palmar aponeurosis distally to enter the mid-palmar space.
The palmar cutaneous branch travels superficial to the TCL and produces a painful, hard-to-treat neuroma when injured (1-3 percent); staying ulnar to the thenar crease protects it. The recurrent motor branch is at highest risk in its transligamentous variant (20-30 percent) - always identify it at the distal TCL edge before dividing the ligament to avoid thenar paralysis.
The volar palmar approach has no classical internervous plane because the thenar muscles receive dual median and ulnar innervation. Safety rests on three things: staying ulnar to the thenar crease (PCBMN protection), identifying the recurrent motor branch at the distal TCL edge before division, and dividing the TCL under direct vision from proximal to distal with the cutting edge directed dorsally and ulnarly.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Palmar cutaneous branch of the median nerve (superficial to the TCL, 5-6 cm proximal to the wrist crease)
- Protection
- Stay ulnar to the thenar crease; identify early; gentle radial retraction
- Structure at risk
- Recurrent motor branch (extraligamentous, subligamentous or transligamentous)
- Protection
- Identify at the distal TCL edge before division, especially transligamentous variants
- Structure at risk
- Median nerve proper (immediately deep to the TCL)
- Protection
- Divide the TCL under direct vision; protect with a probe or vessel loop; document appearance
- Structure at risk
- Flexor tendons (FDS, FDP, FPL)
- Protection
- Retract gently; protect during TCL division; repair any iatrogenic injury
- Structure at risk
- Superficial palmar arch (1-2 cm distal to the TCL edge)
- Protection
- Identify before distal extension; ligate only small branches if bleeding
- Structure at risk
- Common digital nerves and vessels
- Protection
- Gentle retraction between the flexor sheaths; avoid excessive stretch
Complications
- Incidence
- 5-10 percent
- Prevention and treatment
- Complete division under vision; revision open release with neurolysis
- Incidence
- 10-20 percent
- Prevention and treatment
- Early mobilisation; avoid excessive thenar/hypothenar dissection; usually resolves by 3-6 months
- Incidence
- 1-3 percent
- Prevention and treatment
- Stay ulnar to the thenar crease; nerve transposition or capping if established
- Incidence
- 2-5 percent
- Prevention and treatment
- Zig-zag at the wrist crease; early mobilisation; scar massage, revision if severe
- Incidence
- 1-2 percent
- Prevention and treatment
- Meticulous closure; antibiotics; drainage if an abscess forms
- Incidence
- Less than 1 percent
- Prevention and treatment
- Identify and protect the recurrent branch; EIP-to-APB tendon transfer if permanent
Extensile options. Extend proximally across the wrist crease in zig-zag fashion into the forearm (zone 5 flexor tendons, proximal median nerve, Volkmann contracture release) by incising the antebrachial fascia and developing the plane between flexor digitorum superficialis and profundus; the anterior interosseous nerve branch can be identified if needed. Extend distally along the flexor tendon sheath axis into the mid-palm and digits (zones 2-4 tendon repair, mid-palmar abscess drainage, mass excision), using a Brunner zig-zag for digital extension while protecting the digital neurovascular bundles - always identifying the superficial palmar arch first. For complex trauma or infection involving both flexor and extensor surfaces, combine with a separate dorsal approach; staged surgery may be required for severe contamination. Closure and post-operative care. Copious irrigation and meticulous haemostasis; document the median nerve appearance and the completeness of TCL release. Close the palmar aponeurosis loosely with absorbable suture (some surgeons leave it open), approximate the subcutaneous tissue, and close the skin with interrupted or running subcuticular sutures. Apply a bulky dressing with a plaster splint in neutral wrist position, elevate above heart level for 48 hours, and monitor median nerve sensation and motor function. Sutures are removed at 10-14 days with early scar massage from 3 weeks. Rehabilitation: splint and gentle finger range of motion for 0-2 weeks, active wrist and finger motion plus scar massage at 2-4 weeks, progressive strengthening at 4-6 weeks, and full activities by 6-12 weeks (desk job 2-4 weeks, manual work 6-12 weeks). Driving is usually safe at 2-4 weeks once grip is reliable.
Procedures Through This Approach
- Open carpal tunnel release - the principal operation through this exposure; allows direct median nerve inspection and tenosynovectomy.
- Flexor tendon repair (all zones) - zones 3 and 4 in the mid-palm and carpal tunnel through the extensile distal limb.
- Hand infection drainage - mid-palmar and deep palmar space abscesses.
- Mid-palmar mass excision (ganglia, lipomas, giant cell tumour of tendon sheath) and Dupuytren contracture release involving the mid-palm.
- Revision carpal tunnel surgery with neurolysis or nerve wrapping, and combined carpal tunnel decompression with zone 3 flexor tendon repair.
Viva & Exam Focus
RING SAFERING SAFE - safe incision and TCL division
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old woman with electrophysiologically confirmed carpal tunnel syndrome presents for surgical release. Describe your surgical approach and key steps.”
“A 40-year-old diabetic patient presents with a mid-palmar abscess after a penetrating injury. Describe your surgical approach for drainage and any additional considerations.”
“A 30-year-old man sustains a zone 3 flexor tendon laceration with associated carpal tunnel compression from swelling. How would you approach surgical exploration and repair?”
Incision landmarks
- Radial border of the ring finger axis from the distal wrist crease
- Strictly ulnar to the thenar crease throughout (PCBMN protection)
- 4-6 cm length for standard carpal tunnel release
- Extend proximally across the wrist crease (zig-zag) for forearm access
- Extend distally along the flexor sheath axis (Brunner zig-zag) for digits
Nerve protection sequence
- PCBMN: identify superficial to the TCL, stay ulnar to the thenar crease
- Recurrent motor branch: identify at the distal TCL edge before division
- Three variants: extraligamentous (50-60 percent), subligamentous, transligamentous (20-30 percent)
- Median nerve proper: protect with a probe during TCL division
- Common digital nerves: gentle retraction in the mid-palm
TCL division principles
- Divide under direct vision from proximal to distal
- Cutting edge directed dorsally and ulnarly
- Probe or elevator beneath the TCL to protect nerve and tendons
- Continue until the distal edge is completely released
- Inspect the median nerve and perform tenosynovectomy if indicated
Distal danger - superficial palmar arch
- Lies 1-2 cm distal to the distal edge of the TCL
- Identify before extending into the mid-palm
- Supplies the ulnar three digits - injury causes ischaemia
- Protect with gentle retraction during distal dissection
- Ligate only small branches if bleeding
Extensile options
- Proximal: across the wrist crease into the forearm (zone 5, Volkmann)
- Distal: along the flexor sheath axis (zones 3-4, mid-palmar infection)
- Digital: Brunner zig-zag for zone 2 tendon repair
- Combined: separate dorsal incision for extensor surface pathology
- Always identify the superficial palmar arch before distal extension
Key complications to mention
- PCBMN injury: painful thenar neuroma (1-3 percent)
- Recurrent motor branch injury: thenar paralysis (less than 1 percent)
- Incomplete TCL release: most common cause of recurrence (5-10 percent)
- Superficial palmar arch injury: digital ischaemia
- Pillar pain: 10-20 percent, usually resolves by 3-6 months
References
Global practice and registry evidence. The volar palmar approach is used worldwide for carpal tunnel release, flexor tendon surgery and hand infection drainage, with convergent principles across the contemporary practice systems. Open release with direct nerve inspection remains the gold standard for complex, revision or teaching cases, while endoscopic release is accepted for straightforward idiopathic carpal tunnel syndrome in experienced hands (faster return to work but a slightly higher transient nerve injury rate). Carpal tunnel syndrome prevalence is 3-5 percent in the general population, higher in women and manual workers. Open carpal tunnel release has a greater than 85 percent long-term success rate, and incomplete TCL division is the most common cause of recurrence. In resource-limited settings, open release with basic instruments is the standard and the same incision principles apply; WALANT is increasingly used globally to reduce cost and allow intra-operative tendon testing.
Long-term analysis of patients having surgical treatment for carpal tunnel syndrome
- Long-term follow-up of open carpal tunnel release showed high rates of good to excellent results
- Incomplete TCL release was the most common cause of recurrent symptoms requiring revision
- Palmar cutaneous branch neuroma occurred in a small percentage and was difficult to treat
- Early mobilisation reduced pillar pain and improved functional recovery
Ultrasound validation of surface localization for the recurrent motor branch of the median nerve: a cadaveric study
- Cadaveric validation confirms reliable surface landmarks for identifying the recurrent motor branch during open carpal tunnel release
- Transligamentous variants require careful identification at the distal TCL edge before division
- Ultrasound can assist pre-operative planning but intra-operative direct visualisation remains essential
Anatomical Variations of the Neurovascular Structures of the Hand and the Clinical Significance
- Documents frequent anatomic variations in the superficial palmar arch and palmar cutaneous branch relevant to the volar approach
- Superficial palmar arch lies 1-2 cm distal to the TCL in the majority of hands and must be identified before distal extension
- Palmar cutaneous branch injury risk is minimised by staying ulnar to the thenar crease
Time to recovery following open and endoscopic carpal tunnel decompression: meta-analysis
- Meta-analysis comparing recovery after open versus endoscopic carpal tunnel release
- Open release allows direct nerve inspection and extensile access for complex pathology at the cost of longer initial recovery
- Open technique remains preferred when mid-palmar extension or revision surgery is anticipated
Anatomic Variations of the Recurrent Motor Branch of the Median Nerve
- Classic anatomic study describing three variants of the recurrent motor branch: extraligamentous (most common), subligamentous and transligamentous (20-30 percent)
- The transligamentous variant pierces the TCL and is at highest risk during blind division
- Surgeons must identify the branch at the distal TCL edge before ligament division
- This anatomic knowledge remains fundamental to safe open carpal tunnel release technique
Superficial Palmar Arch: Anatomic Study and Clinical Relevance
- Classic anatomic study of superficial palmar arch variations in 200 hands
- Complete arch present in 78 percent, incomplete arch in 22 percent
- The arch lies 1-2 cm distal to the distal edge of the TCL in the majority of specimens
- Ulnar artery contribution dominant in most hands; radial artery contribution variable
Endoscopic versus Open Carpal Tunnel Release: Systematic Review
- Meta-analysis of 21 randomised trials comparing endoscopic and open carpal tunnel release
- Endoscopic release had faster return to work and less scar tenderness but a higher risk of transient nerve injury
- Open release had a lower reoperation rate and allowed direct nerve inspection and tenosynovectomy
- No significant difference in long-term symptom relief or patient satisfaction
Mid-Palmar Space Infections: Surgical Anatomy and Drainage
- Classic description of mid-palmar space anatomy and pathways of infection spread
- The mid-palmar space lies between the flexor tendons and metacarpals, bounded by the thenar and hypothenar septa
- Infection spreads from the flexor tendon sheaths or penetrating injuries
- Adequate drainage requires an extensile volar approach with identification of the superficial palmar arch