Open adductor longus, gracilis and selective brevis tenotomy with iliopsoas lengthening via the medial groin approach · advanced
- Hip surveillance uses migration percentage (Reimers) measured on an AP pelvis radiograph with the hips in neutral — greater than 30 percent indicates risk of progression to dislocation; greater than 40 percent usually requires surgical intervention in non-ambulators.
- The functional abduction threshold is typically less than 20 to 30 degrees with the hip extended — this predicts inability to maintain seating and perineal hygiene and is a key surgical indication alongside radiographic migration.
- The anterior branch of the obturator nerve lies on adductor brevis and must be protected; deliberate anterior obturator neurectomy is avoided because it produces abduction contracture and impairs sitting balance.
- Complete release includes adductor longus, gracilis and selective adductor brevis fibres while preserving the posterior branch of the obturator nerve and the hip joint capsule — over-release leads to abduction contracture and loss of adductor power for transfers.
When & Why
Indication. Symptomatic, progressive hip displacement in a child with cerebral palsy, shown by a rising migration percentage (Reimers) on serial AP pelvis radiographs and/or loss of functional abduction, that has not responded to optimised tone management (oral baclofen, botulinum toxin). The classic trigger is a migration percentage greater than 30 to 40 percent, or functional abduction less than 20 to 30 degrees with the hip extended that compromises seating, perineal hygiene or transfers. Absolute indications
- Progressive hip subluxation with migration percentage greater than 30 to 40 percent on serial surveillance radiographs despite optimised tone management.
- Abduction less than 20 to 30 degrees with the hip extended, producing inability to maintain seating or perform perineal hygiene.
- Painful spastic hip with radiographic displacement that limits quality of life or nursing care.
- Established dislocation in a non-ambulatory patient when reduction and containment are still feasible, usually before skeletal maturity. Relative indications
- Borderline migration (25 to 35 percent) with rapidly increasing tone or loss of abduction on serial examinations.
- Ambulatory patient with deteriorating Trendelenburg gait and abduction less than 20 degrees.
- Pre-operative optimisation before planned femoral or pelvic osteotomy in a child with established displacement.
- Severe adductor spasticity interfering with orthotic wear or therapy participation. Contraindications. Absolute: a fixed abduction contracture greater than 30 degrees (release would worsen function); active infection or untreated pressure sores in the groin or perineum; a non-reducible dislocation with severe acetabular deficiency where containment is no longer possible. Relative: very young age (less than 3 to 4 years) unless migration is rapidly progressive — trial tone management first; severe osteopenia with high fracture risk during positioning; medical comorbidities that preclude safe anaesthesia for a combined procedure. The one decision that matters — soft tissue alone, or add bone? Every plan begins with the same medial groin release; the real choice is whether the displacement is advanced enough to need bony containment at the same sitting:
For migration 30 to 40 percent with abduction less than 20 to 30 degrees, ideally before 5 to 6 years. Reduces migration by 10 to 20 percent and gains 15 to 25 degrees of abduction in most early series.
Add iliopsoas lengthening when a flexion contracture greater than 15 to 20 degrees is present. In ambulatory patients recess at the lesser trochanter insertion (not over-the-brim tenotomy) to preserve hip flexion power.
For migration greater than 40 percent, acetabular index greater than 25 to 30 degrees, or age greater than 5 to 6 years with established displacement. Add femoral varus derotation osteotomy (20 to 30 degrees varus and derotation) plus a Dega, Salter or Pemberton pelvic osteotomy — redislocation falls below 15 percent at 10 years.
Consent specifically for incomplete abduction gain, over-release with abduction contracture, obturator or medial femoral cutaneous nerve injury, wound dehiscence, heterotopic ossification, recurrent subluxation needing bony reconstruction, and the frequent need for combined femoral and pelvic osteotomy in established displacement. Setup. Supine on a radiolucent table with both hips prepared and draped free (to compare abduction and allow bilateral release). A small sandbag under the ipsilateral buttoick opens the medial groin; the image intensifier is set for AP pelvis views to confirm migration percentage. General anaesthesia with muscle relaxation, with caudal or epidural analgesia for bilateral cases, and routine antibiotic prophylaxis.
The Operation
The goal is to restore a painless, stable hip with enough abduction for seating and hygiene by selectively releasing the spastic adductors and lengthening the iliopsoas through the medial groin approach — protecting the anterior obturator nerve, the medial femoral circumflex artery and the hip capsule throughout, and stopping the instant the target abduction is reached. The exposure is laid out in full as the first steps of the sequence below (and in depth on the medial approach to the hip page).
Operative sequence
- Supine on a radiolucent table; both hips prepared and draped free to compare abduction and permit bilateral release.
- Small sandbag under the ipsilateral buttoick to open the medial groin; image intensifier positioned for AP pelvis views to confirm migration percentage.
- General anaesthesia with muscle relaxation; caudal or epidural analgesia for bilateral cases; routine antibiotic prophylaxis.
- Flex, abduct and externally rotate the hip; palpate the adductor longus tendon.
- Make a transverse or gently curved incision in the medial groin crease, 4 to 6 cm long, centred over adductor longus and staying within the crease to hide the scar.
- Deepen through subcutaneous fat, identifying and protecting the medial femoral cutaneous nerve branches.
- Adductor longus is the most prominent cord running from the pubic tubercle distally; incise the fascia longitudinally over the tendon.
- Pass a right-angle clamp beneath the tendon and divide it at the pubic insertion with cutting diathermy or scissors, leaving a 5 to 10 mm stump.
- Identify and protect the medial femoral circumflex artery branches at the distal margin before completing the tenotomy.
- Gracilis lies immediately posterior to longus; isolate it with a right-angle clamp and divide it at the same level.
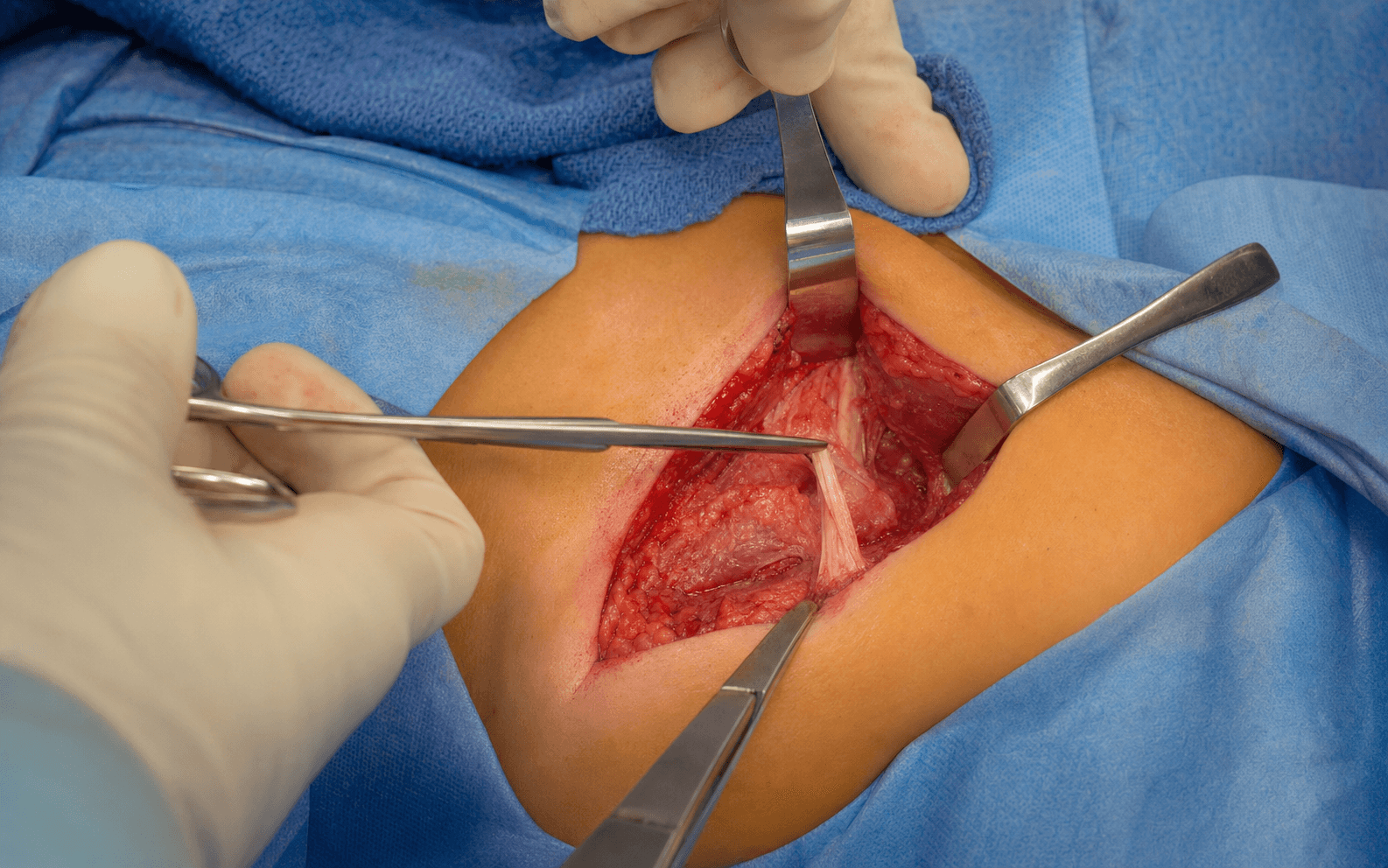
- The interval between adductor longus and brevis now opens; the anterior branch of the obturator nerve is seen lying on the surface of adductor brevis.
- Gently dissect the nerve free, loop it with a vessel loop and retract it medially for the rest of the procedure.
- Identify the anterior fibres of adductor brevis; release only the anterior 50 to 70 percent of fibres from the inferior pubic ramus, staying extra-capsular.
- Leave the posterior third intact to preserve residual adductor power and protect the posterior obturator branch; do not violate the hip joint capsule.
- With the hip flexed and externally rotated, palpate the iliopsoas tendon over the pelvic brim.
- In a non-ambulator, lengthen by fractional tenotomy or Z-lengthening over the brim (intra-pelvic); in an ambulator, recess at the lesser trochanter insertion to preserve hip flexion power.
- Confirm the hip now extends fully without residual flexion contracture.
- Re-check abduction with the hip extended — aim for 30 to 40 degrees of painless abduction.
- Irrigate the wound, achieve meticulous haemostasis, and close the fascia over the released tendons with absorbable suture and the skin with absorbable subcuticular suture.
- Apply a bulky dressing with an abduction pillow or brace; if a femoral osteotomy is to follow, close the medial incision first before turning to the lateral approach.
The anterior branch of the obturator nerve lies on the surface of adductor brevis in the longus-brevis interval. Identify it under direct vision, loop it with a vessel loop and retract it medially throughout the release. Deliberate anterior obturator neurectomy is avoided — it removes residual adductor power and produces an abduction contracture that destroys sitting balance and perineal hygiene. Watch at the deep dissection for the same injuries: mistaking gracilis for longus (gracilis lies posterior and is more tendinous); the medial femoral circumflex artery at the distal longus margin; over-lengthening the iliopsoas in an ambulator; and entering the hip capsule.
Ask the assistant to adduct against resistance — the longus tendon becomes rock-hard. Divide it about 5 mm from the pubic insertion to leave a cuff for potential repair and to stay clear of the obturator nerve origin, and identify the medial femoral circumflex artery just distal to this point before completing the tenotomy.
Release adductor brevis fibres progressively, re-checking abduction after each increment, and stop once 30 to 35 degrees of painless abduction with the hip extended is reached. Over-release is functionally worse than under-release, especially in a non-ambulatory child.
Location: on the surface of adductor brevis, in the longus-brevis interval. Risk: transection, or combined posterior-branch injury, causes complete adductor paralysis; deliberate neurectomy causes abduction contracture. Protection: identify under direct vision, loop and retract medially; selective partial neurectomy only in carefully selected non-ambulators after counselling.
Location: along the inferior border of the adductor longus insertion, passing between longus and magnus to supply the femoral head via the retinacular vessels. Risk: laceration causes brisk bleeding and potential femoral-head ischaemia. Protection: identify at the distal tendon edge before completing the tenotomy; ligate small branches only under direct vision.
Location: deep to adductor brevis and the iliopsoas tendon at the level of the lesser trochanter. Risk: violation causes instability, heterotopic ossification and potential septic arthritis; the capsule is often thickened and adherent in spastic hips. Protection: stay extra-capsular with blunt dissection under direct vision; repair any inadvertent entry.
Location: excessive brevis release or combined anterior neurectomy removes the last adductor power. Risk: abduction contracture greater than 30 to 40 degrees prevents comfortable seating, perineal care and transfers. Prevention: release only longus, gracilis and the anterior 50 to 70 percent of brevis; leave the posterior third of brevis and all of magnus; never perform complete anterior neurectomy.
Aftercare & Complications
Rehabilitation | Phase | Timing | Weight-bearing | Therapy | |-------|--------|----------------|---------| | 1 | 0-2 weeks | As tolerated for isolated release; non or partial for 6 weeks if combined with femoral osteotomy | Abduction positioning 30 to 40 degrees at all times; finger active motion only | | 2 | 2-6 weeks | Continue | Gentle passive and active-assisted abduction and flexion within the safe range; wound check at 48 hours | | 3 | 6-12 weeks | Progress, or protected per fixation | Strengthening, gait training and sitting balance; transition to night abduction brace | | 4 | 3-6 months | Full | Return to therapy and orthotic programme; surveillance radiographs at 3, 6 and 12 months | Maintain 30 to 40 degrees of abduction with pillows or a brace whenever the child is not mobilising, but avoid forced abduction greater than 40 degrees — it risks obturator nerve stretch and wound dehiscence. Use multimodal analgesia (caudal or epidural infusion for 48 to 72 hours, paracetamol, NSAIDs if renal function permits, opioids as needed) and optimise nutrition early, especially in gastrostomy-dependent children. Continue surveillance radiographs every 6 months until skeletal maturity. Special cases. Perform bilateral release in a single sitting when the child is medically stable to avoid two anaesthetics; stage 2 to 4 weeks apart if there is significant respiratory or nutritional compromise. When bony reconstruction is combined, do the adductor release first to allow safe positioning, close the medial incision, then turn to the lateral approach for the femoral varus derotation osteotomy and pelvic osteotomy, and protect with a spica cast or abduction brace for 6 to 12 weeks depending on fixation stability. Complications
- Incidence
- 2-5 percent (higher with aggressive retraction)
- Recognition
- Loss of adductor power, abduction contracture greater than 30 degrees, poor sitting balance
- Prevention and management
- Prevention: identify and protect the nerve with a vessel loop throughout; limit brevis release to anterior 50 to 70 percent. Management: observation and aggressive therapy; abduction contracture may need further release or bracing; rarely nerve repair or grafting
- Incidence
- 5-10 percent (over-release or neurectomy)
- Recognition
- Hip abduction greater than 40 degrees at rest, inability to adduct for seating or perineal care, gait deterioration in ambulators
- Prevention and management
- Prevention: partial brevis release only; never complete anterior neurectomy. Management: serial abduction positioning; rarely adductor magnus transfer or posterior capsular release for severe cases
- Incidence
- 15-30 percent after isolated soft-tissue release when migration greater than 40 percent
- Recognition
- Progressive rise in migration percentage on surveillance radiographs, loss of abduction, pain or seating difficulty
- Prevention and management
- Prevention: combine soft-tissue release with varus derotation osteotomy and pelvic osteotomy when migration exceeds 40 percent. Management: revision to bony containment; salvage proximal femoral resection or arthrodesis for a painful dislocation in a non-ambulator
- Incidence
- 3-8 percent (higher in malnourished or gastrostomy-dependent children)
- Recognition
- Erythema, drainage or wound separation at 7 to 14 days, fever, raised CRP
- Prevention and management
- Prevention: optimise nutrition pre-operatively, meticulous layered closure, 24-hour antibiotics, delay aggressive abduction bracing 10 to 14 days. Management: local wound care, oral or IV antibiotics, surgical debridement if deep infection suspected
- Incidence
- 5-15 percent (higher with capsular violation or aggressive retraction)
- Recognition
- Painful swelling, limited motion, radiographic calcification at 4 to 12 weeks
- Prevention and management
- Prevention: extra-capsular dissection, gentle tissue handling, consider indomethacin prophylaxis in high-risk patients. Management: observation (most resolve); surgical excision after maturation (greater than 6 months) if symptomatic
- Incidence
- Less than 2 percent
- Recognition
- Intra-operative bleeding, post-operative haematoma, theoretical femoral head vascular compromise
- Prevention and management
- Prevention: identify the vessel at the distal adductor longus margin before completing tenotomy; ligate small branches only under direct vision. Management: intra-operative ligation or bipolar cautery; observe for femoral head changes on surveillance radiographs
- Incidence
- 5-10 percent in ambulatory patients
- Recognition
- Difficulty with transfers, rising from sitting and stair climbing; weakness on hip flexion testing
- Prevention and management
- Prevention: recess at the insertion rather than over-the-brim tenotomy in ambulatory children; avoid excessive lengthening. Management: strengthening therapy; rarely tendon repair or transfer for severe functional loss
Viva & Exam Focus
ADDUCTORADDUCTOR — surgical goals and limits
SPASTICSPASTIC — hip displacement monitoring in cerebral palsy
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 6-year-old non-ambulatory child with spastic quadriplegic cerebral palsy has a migration percentage of 38 percent on the right hip and 25 percent on the left. Abduction is 15 degrees on the right and 35 degrees on the left. The child has increasing difficulty with seating and perineal hygiene. What is your surgical plan?”
“During medial groin adductor release in a 5-year-old child you identify the anterior obturator nerve on the surface of adductor brevis. The assistant asks whether you should perform an anterior obturator neurectomy to improve the abduction gain. How do you respond and what is your rationale?”
“A 4-year-old ambulatory child with spastic diplegia has bilateral migration percentages of 32 percent, abduction of 18 degrees, and a 20-degree hip flexion contracture. The family reports deteriorating gait and increasing falls. Outline your surgical plan and the rationale for including or excluding iliopsoas lengthening.”
Hip surveillance thresholds
- Migration percentage (Reimers): greater than 30 percent triggers increased surveillance; greater than 40 percent is the surgical threshold in non-ambulators
- Abduction less than 20 to 30 degrees with the hip extended is the functional indication for release
- Pain, seating difficulty or perineal hygiene problems are absolute indications regardless of the exact migration value
- Ambulatory patients: deteriorating Trendelenburg gait or flexion contracture greater than 15 to 20 degrees prompts earlier intervention
Surgical anatomy
- Adductor longus: most superficial, primary release target; inserts on the linea aspera, leave a 5 to 10 mm stump
- Gracilis: posterior to longus; release in continuity for maximal abduction gain
- Adductor brevis: release only the anterior 50 to 70 percent; leave posterior fibres and magnus intact
- Anterior obturator nerve: lies on the brevis surface — protect with a vessel loop; never transect deliberately
- Iliopsoas: lengthen over the pelvic brim (non-ambulatory) or recess at the lesser trochanter (ambulatory)
- Medial femoral circumflex artery: at the distal adductor longus margin — identify before tenotomy
Indication — soft tissue alone vs combined bony
- Soft-tissue release alone: migration 30 to 40 percent with abduction less than 20 to 30 degrees; age less than 5 to 6 years
- Add iliopsoas lengthening when flexion contracture is greater than 15 to 20 degrees
- Combined bony reconstruction: migration greater than 40 percent, or acetabular index greater than 25 to 30 degrees, or age greater than 5 to 6 years
- Combined reconstruction = varus derotation osteotomy plus pelvic osteotomy (Dega, Salter or Pemberton)
Operative technique — key steps
- 1. Transverse medial groin crease incision over adductor longus
- 2. Isolate and divide adductor longus and gracilis at the pubic insertion; protect the medial femoral circumflex artery
- 3. Identify the anterior obturator nerve on the brevis surface and protect with a vessel loop
- 4. Release only the anterior 50 to 70 percent of adductor brevis — stay extra-capsular
- 5. Lengthen iliopsoas (recession at the insertion in ambulatory patients)
- 6. Verify 30 to 40 degrees of painless abduction with the hip extended before closure
- 7. Meticulous haemostasis and layered closure; abduction positioning immediately
Danger zones
- Anterior obturator nerve: transection or aggressive retraction produces abduction contracture
- Medial femoral circumflex artery: at the distal adductor longus margin — identify before completing tenotomy
- Hip joint capsule: violation risks instability and heterotopic ossification
- Over-release of brevis: abduction contracture greater than 40 degrees is functionally worse than the original deformity
Complications
- Anterior obturator nerve injury: 2 to 5 percent — abduction contracture, poor sitting balance
- Abduction contracture: 5 to 10 percent — avoid by partial brevis release and no neurectomy
- Recurrent subluxation: 15 to 30 percent after isolated release when migration is greater than 40 percent
- Wound dehiscence or infection: 3 to 8 percent — optimise nutrition, delay aggressive bracing
- Heterotopic ossification: 5 to 15 percent — extra-capsular dissection reduces risk
Post-operative protocol
- Abduction positioning or brace at 30 to 40 degrees for 6 to 12 weeks
- Immediate weight-bearing for isolated soft-tissue release
- Surveillance radiographs at 3, 6 and 12 months then every 6 months until skeletal maturity
- Combined bony reconstruction needs 6 to 12 weeks of protected weight-bearing depending on fixation
Special considerations
- Ambulatory patients: iliopsoas recession at the insertion (not over-the-brim) to preserve flexion power
- Bilateral release: single sitting when medically stable; staged if significant comorbidities
- Combined varus derotation osteotomy plus pelvic osteotomy once migration exceeds 40 percent or acetabular index greater than 25 to 30 degrees
- Nutrition and tone optimisation pre-operatively reduce wound and recurrence risk
Background & Evidence
Why the hip subluxes. Spastic hip displacement in cerebral palsy is driven by sustained adductor and flexor spasticity overpowering the immature acetabulum, with the femoral head migrating laterally and proximally. Early identification of a migration percentage greater than 30 percent allows soft-tissue release before irreversible acetabular dysplasia develops; delaying surgery until migration exceeds 50 percent or dislocation occurs significantly reduces the success of containment procedures.
- Course / location
- Most superficial; pubic tubercle to the linea aspera
- Surgical relevance
- Primary target of release; divide at the pubic insertion leaving a 5 to 10 mm stump
- Course / location
- Immediately posterior to longus; inferior pubic ramus to the pes anserinus
- Surgical relevance
- Released in continuity with longus for maximal abduction gain
- Course / location
- Deep to longus and gracilis
- Surgical relevance
- Release only the anterior 50 to 70 percent; the anterior obturator nerve lies on its surface
- Course / location
- Most posterior and largest adductor
- Surgical relevance
- Preserved to maintain residual adductor power and protect the posterior obturator branch
- Course / location
- On the surface of brevis, in the longus-brevis interval
- Surgical relevance
- Protect with a vessel loop throughout; never transect deliberately
- Course / location
- Deep to adductor brevis
- Surgical relevance
- Preserved by limiting the depth of brevis release
- Course / location
- Over the pelvic brim, anterior to the capsule, to the lesser trochanter
- Surgical relevance
- Lengthen over the brim (non-ambulatory) or recess at the insertion (ambulatory)
- Course / location
- Along the distal margin of adductor longus
- Surgical relevance
- Supplies the femoral head; identify and protect before completing tenotomy
- Course / location
- Deep to adductor brevis and iliopsoas
- Surgical relevance
- Stay extra-capsular; often thickened and adherent in spastic hips
- Meaning
- Risk of progression to dislocation
- Action
- Increase surveillance frequency; consider soft-tissue release
- Meaning
- Established displacement in non-ambulators
- Action
- Surgical intervention — combine soft-tissue release with bony reconstruction
- Meaning
- Functional loss — seating and perineal hygiene compromised
- Action
- Indication for release regardless of the exact migration value
- Meaning
- Established acetabular dysplasia
- Action
- Add pelvic osteotomy at the index procedure
- Meaning
- Iliopsoas tightness impairing gait and transfers
- Action
- Lengthen iliopsoas at the time of adductor release
Evidence for soft-tissue release. Isolated adductor release reduces migration percentage by 10 to 20 percent in early subluxation (less than 40 percent) and improves abduction by 15 to 25 degrees in most series; success is highest when performed before 5 to 6 years of age and when combined with iliopsoas lengthening and post-operative abduction positioning. In established displacement greater than 40 percent, soft-tissue release alone fails to maintain containment in greater than 60 percent of cases at 5 years, so bony reconstruction is required. Adding femoral varus derotation osteotomy achieves stable containment in 70 to 85 percent of children with migration 40 to 60 percent, and adding a pelvic osteotomy (Dega, Salter or Pemberton) further improves acetabular coverage and reduces the redislocation risk to less than 15 percent at 10 years. The consistent message across series — release early, release selectively, preserve the anterior obturator nerve, and add bone when displacement is established — is why nerve-sparing selective release is the standard and a perennial viva favourite.
References
Soft-tissue release for spastic hip subluxation in cerebral palsy
- Retrospective review of soft-tissue release outcomes in spastic hip subluxation
- Isolated soft-tissue release maintained containment in the majority of early cases at 5 years
- Anterior obturator neurectomy was associated with a higher abduction contracture risk
Soft-tissue releases to treat spastic hip subluxation in children with cerebral palsy
- Soft-tissue releases achieved stable containment in 65 percent of hips with migration less than 40 percent
- Abduction gain averaged 18 degrees with selective release
- Neurectomy was linked to a 12 percent abduction contracture rate
Prevention of spastic paralytic dislocation of the hip
- Review of adductor release with and without neurectomy in cerebral palsy
- The neurectomy group had a 22 percent incidence of abduction contracture versus 4 percent in the nerve-sparing group
- Nutrition status influenced wound and heterotopic ossification rates
Management of hip disorders in patients with cerebral palsy
- Comprehensive review of hip surveillance and surgical indications in cerebral palsy
- Migration percentage greater than 30 percent triggers increased surveillance and consideration of release
- Early soft-tissue intervention before 40 percent migration improves long-term containment