Motion-preserving cervical total disc replacement via the Smith-Robinson anterior approach · advanced
- Indications require a preserved motion segment with minimal facet arthrosis, no significant instability or kyphosis, and soft-disc pathology rather than severe spondylosis or ankylosis.
- Smith-Robinson approach between the carotid sheath laterally and the visceral column medially protects the recurrent laryngeal nerve, oesophagus and sympathetic chain; thorough discectomy and endplate preparation are critical for implant stability.
- Midline placement of the mobile articulating implant is mandatory to restore physiologic motion and reduce the theoretical risk of adjacent-segment degeneration compared with fusion.
- Heterotopic ossification is the most common device-specific complication; incidence increases with time and may eliminate motion despite a technically successful arthroplasty.
- Patient selection is the single strongest predictor of durable motion preservation — greater than 5 degrees segmental motion on dynamic films and absence of significant facet degeneration are non-negotiable prerequisites.
When & Why
Indication. Symptomatic single- or two-level cervical radiculopathy or myelopathy from a soft-disc herniation (or spondylotic compression in a well-selected patient) that has failed at least six weeks of non-operative care — physiotherapy, NSAIDs and selective nerve-root blocks — where the motion segment is still worth preserving. Patient preference for motion preservation after an informed discussion of the adjacent-segment disease risk is itself a valid indication once the anatomical criteria are met. The ideal candidate is a young, active patient (typically less than 60 years) with a soft-disc herniation, preserved segmental motion (greater than 5 degrees on flexion-extension films), minimal facet arthrosis, no instability (translation less than 2 mm) and no significant segmental kyphosis, who understands that the goal is motion preservation rather than a guaranteed cure. Relative indications include two-level disease in which a fusion would create a long lever arm stressing adjacent segments, and a professional or recreational need to keep cervical rotation and flexion-extension. Contraindications.
- Factor
- Ankylosis or spontaneous fusion at the index level
- Why it matters
- No motion to preserve — arthroplasty is pointless
- Factor
- Severe spondylosis with greater than 50 percent disc-height loss or large posterior osteophytes
- Why it matters
- Cannot seat or move an implant
- Factor
- Osteoporosis (T-score less than -2.5) or metabolic bone disease
- Why it matters
- High subsidence risk
- Factor
- Active infection, tumour or inflammatory arthropathy
- Why it matters
- Standard contraindication to an implant
- Factor
- Greater than 2 mm translation on dynamic films (instability)
- Why it matters
- Motion preservation worsens an unstable segment
- Factor
- Significant cervical kyphosis (greater than 10 degrees segmental)
- Why it matters
- A mobile implant cannot restore lordosis
- Factor
- Previous anterior cervical surgery at the same level
- Why it matters
- Scarred tissue planes and re-operative risk
- Factor
- Severe facet arthropathy or disease needing posterior decompression
- Why it matters
- Facet disease defeats the goal of motion preservation
- Factor
- Multilevel disease (three or more levels)
- Why it matters
- Higher heterotopic ossification and motion loss
- Factor
- Smoking or systemic steroids impairing bone ingrowth
- Why it matters
- Poor implant fixation
Consent specifically for recurrent laryngeal nerve injury (1-3 percent hoarseness, higher on the right at C6-7), dysphagia (5-15 percent transient, less than 1 percent permanent), oesophageal perforation (less than 0.5 percent), vertebral artery injury (less than 0.5 percent), implant migration or subsidence (2-5 percent), heterotopic ossification (10-50 percent), persistent or new neurologic deficit (1-2 percent), and the possibility of conversion to fusion if intra-operative findings preclude arthroplasty. Setup. Supine on a radiolucent table, head in slight extension on a donut or Mayfield headrest, shoulders taped caudally so the lower cervical spine is visible on fluoroscopy, and a scapular roll to maintain lordosis. General endotracheal anaesthesia with MEP and SSEP neuromonitoring for myelopathy cases. Have a high-speed burr, Caspar distractor, radiolucent retractors, implant-specific trials and inserters, and biplanar C-arm fluoroscopy ready throughout.
The Operation
The goal is a complete discectomy and neural decompression through the Smith-Robinson anterior approach, then seating of a mobile disc prosthesis exactly in the midline so the segment keeps moving. The exposure — the avascular plane between the carotid sheath laterally and the visceral column medially — is the heart of the operation and is laid out as the first steps below (and in depth on the Smith-Robinson approach to the anterior cervical spine page).
Operative sequence
- Supine on a radiolucent table, head in slight extension (10-15 degrees) on a donut or Mayfield headrest; shoulders taped caudally; scapular roll for lordosis.
- General endotracheal anaesthesia with MEP and SSEP neuromonitoring for myelopathy; a nasogastric tube helps identify the oesophagus in revision cases.
- Confirm the level with a needle in the disc space and a lateral fluoroscopic image before any deep dissection. A left-sided approach at C6-7 reduces recurrent laryngeal nerve risk; at C5-6 either side is acceptable.
- A transverse skin-crease incision at the level of the disc space (C5-6 at the cricoid cartilage, C6-7 about 2 cm above the clavicle).
- Divide the platysma in line with the skin and raise subplatysmal flaps superiorly and inferiorly.
- Retract the sternocleidomastoid laterally and the strap muscles medially. Palpate the carotid pulse and develop the avascular plane between the carotid sheath (laterally) and the visceral column (medially) with blunt finger dissection.
- This Smith-Robinson interval protects the recurrent laryngeal nerve in the tracheo-oesophageal groove and the oesophagus by medial retraction of the visceral column.
- Divide the prevertebral fascia in the midline.
- Elevate the longus colli from the anterior vertebral bodies with bipolar cautery and a Cobb elevator, exposing the disc space from uncinate to uncinate.
- Place self-retaining retractors with smooth blades UNDER the longus colli to shield the sympathetic chain, which lies on its lateral border about 10-15 mm from the midline; aggressive lateral retraction or monopolar cautery here causes Horner syndrome.
- Staying medial keeps the vertebral artery (in the transverse foramen, entering at C6) out of the field.
- Remove the anterior longitudinal ligament and anterior annulus; excise the disc with pituitary rongeurs and curettes.
- Resect the posterior annulus and posterior longitudinal ligament to expose the dura and nerve roots.
- The uncovertebral joints form the anterior boundary of the neural foramen; resect only the posterior third of the uncinate if foraminal stenosis is present — excessive lateral resection risks the vertebral artery within the transverse foramen.
- Burr down any uncovertebral osteophytes under loupe or microscope and confirm complete decompression of BOTH nerve roots with a 3 mm nerve hook.
- Remove the cartilaginous endplates with curettes and a high-speed burr but PRESERVE the dense subchondral bone — it gives immediate implant stability and resists subsidence. Cervical endplates are concave superiorly and convex inferiorly; match the implant footprint to this morphology.
- Shape the endplates to the implant footprint and resect anterior osteophytes flush with the vertebral body so they cannot seed heterotopic ossification or block range of motion.
- Partially resect the uncovertebral joints only if they contribute to foraminal stenosis.
- Distract the disc space with the Caspar system or implant-specific distractors, limiting distraction to about 2 mm above resting height to avoid cord contusion.
- Trial under fluoroscopy. The correct size restores disc height (usually 5-7 mm), segmental lordosis (about 5-7 degrees) and allows at least 5-10 degrees of flexion-extension on dynamic testing.
- The trial must sit exactly midline on the AP view and cover at least 80 percent of the endplate width.
- Insert the definitive implant under fluoroscopic control and engage the keel or fixation mechanism.
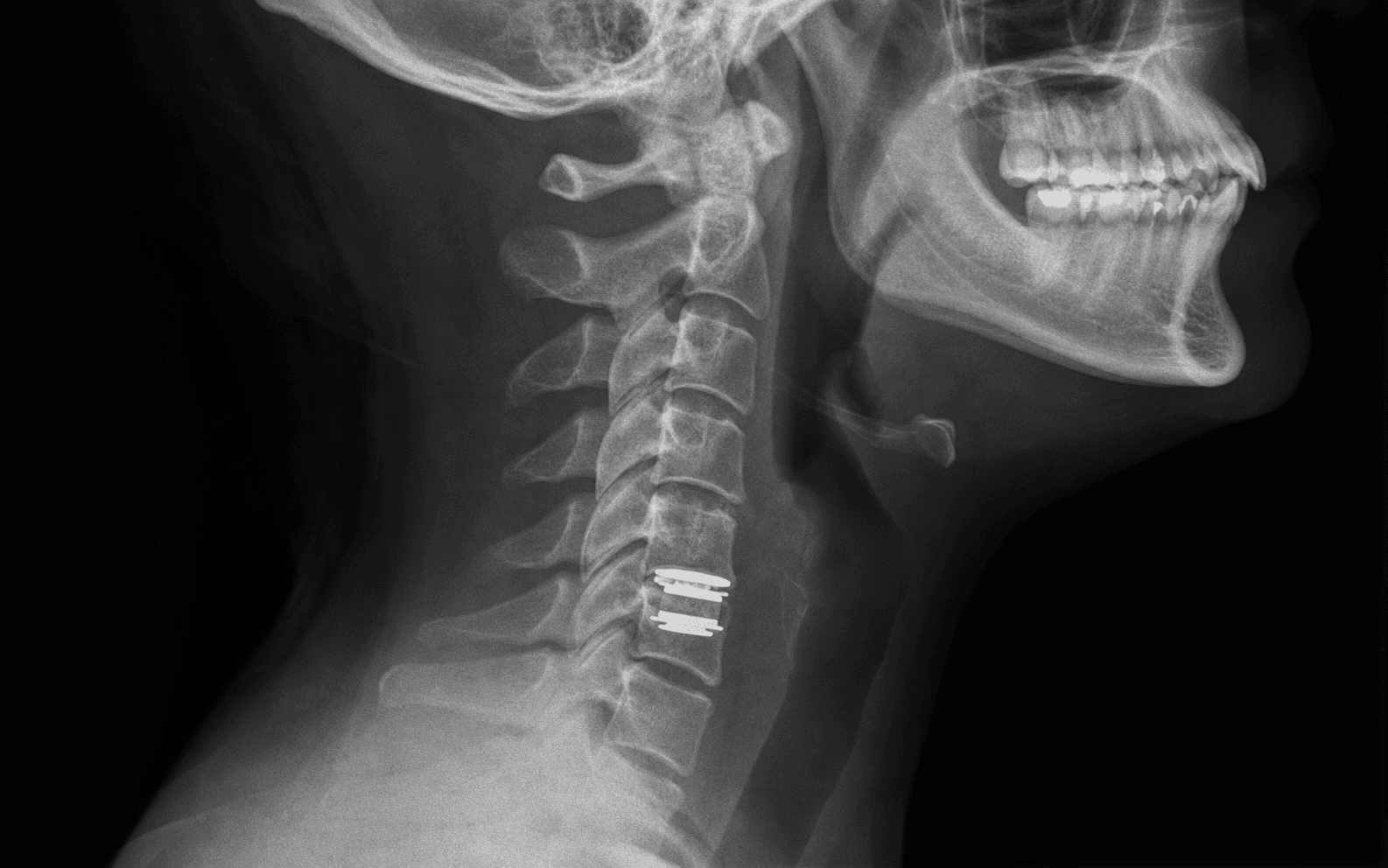
- Remove the inserter and confirm midline placement, correct height and no anterior or posterior migration on final AP and lateral radiographs.
- Irrigate and secure haemostasis.
- Close the platysma with absorbable suture and the skin with subcuticular absorbable suture or clips. No drain is routinely required.
- A soft collar is optional for comfort only — most patients are mobilised immediately without immobilisation.
The right recurrent laryngeal nerve loops under the subclavian and is more oblique and superficial at C6-7, where it is most vulnerable; the left loops under the aortic arch and is safer low down. Most surgeons therefore choose a left-sided Smith-Robinson approach for C6-7 arthroplasty. Document the side and the rationale, and assess vocal-cord function pre-operatively in revision cases. Hoarseness occurs in 1-3 percent and usually resolves.
Persistent radiculopathy after arthroplasty is usually an incomplete foraminal decompression, not the implant. Remove the entire disc including the posterior annulus and any calcified ligament before endplate preparation — residual disc prevents the implant seating fully and creates a mobile segment that subsides. Check both foramina with a 3 mm nerve hook before trialling, limit Caspar distraction to about 2 mm above resting height to avoid cord contusion, and use cotton patties rather than suction directly on a thin dura.
The implant must sit exactly in the midline on the AP view to restore physiologic motion and unload the facets. If the trial is off midline, re-seat it before the final implant — an off-centre device fails early. Confirm it covers at least 80 percent of the endplate width and restores 5-7 mm of height with about 5-7 degrees of lordosis.
The right recurrent laryngeal nerve loops under the subclavian, the left under the aortic arch. At C6-7 the right nerve is more oblique and superficial, so most surgeons use a left-sided Smith-Robinson approach there. Hoarseness is 1-3 percent and usually resolves; document the side and rationale in the operative note.
The sympathetic chain lies on the longus colli about 10-15 mm lateral to the midline. Aggressive lateral retraction or electrocautery causes unilateral ptosis, miosis and anhidrosis. Stay within the medial half of the longus colli and avoid monopolar cautery near its lateral border.
The oesophagus lies immediately medial to the carotid sheath. Perforation presents with neck swelling, crepitus, fever and dysphagia. Prevent it with blunt dissection, frequent retractor relaxation, and a nasogastric tube in high-risk revisions to allow palpation of the oesophageal wall.
The artery enters the C6 transverse foramen; the midline-to-artery distance at C5-6 is about 15-18 mm. Laceration from aggressive uncinate resection causes massive bleeding or posterior-circulation stroke. Confirm anatomy on pre-operative CT and limit lateral resection to the medial half of the uncinate.
Removing subchondral bone or overstuffing the disc space leads to early subsidence and loss of lordosis. Ideal preparation removes only cartilage while preserving dense endplate bone. The implant footprint should cover at least 80 percent of the endplate and distraction should be limited to about 2 mm above resting height.
Bridging bone anterior or posterior to the implant at 6-24 months signals Grade III-IV heterotopic ossification and loss of the motion benefit. Prevent it with meticulous haemostasis, clearing bone dust, and short-course NSAID prophylaxis in high-risk patients (male sex, multilevel disease). Once formed, revision to fusion is the only reliable salvage.
The Device: Constraint, Kinematics and Why Technique Decides Motion
How devices are classified. By constraint — unconstrained (no fixed centre of rotation, e.g. a mobile core), semi-constrained, and constrained (a fixed ball-and-socket centre of rotation) — and by bearing surface: metal-on-polyethylene, metal-on-metal, or ceramic.
What they are trying to reproduce. Physiological segmental kinematics, including a mobile, posteriorly located instantaneous centre of rotation and the coupled flexion-extension and lateral bending of a normal segment — rather than behaving like a single fixed hinge. The goal is to restore the centre of rotation, not merely fill the space.
Why technique decides whether motion is actually preserved. The device must be correctly sized to the endplates (over- or undersizing risks subsidence or poor fit), placed in the midline and parallel to the endplates, with disc-space height and lordosis restored and the endplates preserved, not over-resected. Malposition, undersizing or endplate violation lead to subsidence, migration, accelerated wear and osteolysis, abnormal facet loading and more heterotopic ossification — each of which defeats the whole point of the operation.
Good bone quality is needed both for fixation and to resist subsidence, which is part of why osteoporosis is a contraindication.
A well-chosen patient still needs a correctly designed, correctly implanted device to keep the segment moving. Quote the constraint class and bearing surface, then the three technical requirements — correct sizing, midline and parallel placement, endplate preservation — because those are what separate a mobile segment from one that quietly fuses itself.
Aftercare & Complications
Post-operative protocol | Phase | Timing | Mobilisation and activity | Imaging and review | |-------|--------|---------------------------|--------------------| | Immediate | Day 0-2 | Mobilise out of bed on day of surgery or day 1; soft collar for comfort only (most discard by day 3); paracetamol, NSAIDs, short opioid course | AP and lateral radiographs before discharge; monitor for swelling, dysphagia, hoarseness, new deficit | | Early | 2-6 weeks | Light activities and desk work by 2-4 weeks; no heavy lifting or contact sports for 6-12 weeks; gentle cervical range of motion from 2 weeks | Wound check and radiographs at 2 weeks | | Late | 6 weeks on | Full activities including sport by 3 months if asymptomatic | Dynamic radiographs at 6 weeks, 3, 6 and 12 months, then annually | Most patients return to desk work by 2-4 weeks and to full activities including sport by about 3 months. Dynamic radiographs monitor motion preservation and watch for early heterotopic ossification. Special situations
More operative time and blood loss, and higher heterotopic ossification and dysphagia risk. Demands meticulous midline placement at both levels; some surgeons stage the two levels 6-12 weeks apart in older or frail patients.
Usual reasons are persistent radiculopathy (incomplete decompression), subsidence, heterotopic ossification with motion loss, or infection. Options are conversion to ACDF with an anterior plate, posterior foraminotomy or laminectomy, or rarely implant exchange. Pre-operative CT and MRI are essential to assess bone stock and neural compression.
A relative contraindication. If proceeding, select an implant with a larger footprint and keeled or screw fixation, consider a post-operative bisphosphonate holiday, and follow radiographs longer for subsidence.
Complications
- Incidence
- 10-50% at 5 years (Grade I-IV)
- Recognition
- Bridging bone anterior or posterior to implant on lateral radiograph; progressive loss of motion on dynamic films
- Prevention and management
- Prevention: meticulous haemostasis, removal of bone dust, short-course NSAID prophylaxis in high-risk patients. Management: observation for Grade I-II; revision to fusion for symptomatic Grade III-IV with loss of motion
- Incidence
- 2-5%
- Recognition
- Progressive loss of disc height, implant settling into vertebral body, new neck pain or radiculopathy
- Prevention and management
- Prevention: preserve subchondral bone during endplate preparation, select appropriate implant size, avoid over-distraction. Management: revision to larger implant or conversion to fusion with anterior plate
- Incidence
- 1-3% hoarseness (higher on right at C6-7)
- Recognition
- Post-operative hoarseness, vocal cord paralysis on laryngoscopy
- Prevention and management
- Prevention: left-sided approach at C6-7, gentle medial retraction of visceral column, pre-operative vocal cord assessment in revision cases. Management: observation (most resolve); ENT referral for persistent paralysis
- Incidence
- 5-15% transient; less than 1% permanent
- Recognition
- Difficulty swallowing solids or liquids; worse with multilevel procedures
- Prevention and management
- Prevention: limit retraction time, use smooth retractors, place nasogastric tube in high-risk cases. Management: speech therapy, dietary modification; persistent dysphagia warrants swallow study
- Incidence
- 1-2%
- Recognition
- Worsening myelopathy or radiculopathy post-operatively; new sensory or motor loss
- Prevention and management
- Prevention: complete foraminal decompression, avoid over-distraction, intra-operative neuromonitoring. Management: immediate post-operative MRI; return to theatre if compressive haematoma or malpositioned implant
- Incidence
- less than 0.5%
- Recognition
- Neck crepitus, fever, dysphagia, mediastinitis
- Prevention and management
- Prevention: blunt dissection, frequent retractor relaxation, nasogastric tube in revision surgery. Management: urgent contrast swallow, surgical repair, broad-spectrum antibiotics, drainage
- Incidence
- less than 0.5%
- Recognition
- Profuse bleeding from lateral gutter, posterior circulation stroke
- Prevention and management
- Prevention: limit lateral resection to medial half of uncinate, pre-operative CT to assess transverse foramen anatomy. Management: immediate tamponade, endovascular or open repair, posterior circulation imaging
Viva & Exam Focus
SMITHSMITH — Smith-Robinson anterior cervical exposure
IMPLANTIMPLANT — critical technical points for cervical TDR
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 48-year-old man with single-level C5-6 soft-disc herniation causing radiculopathy has failed 8 weeks of conservative treatment. Dynamic radiographs show 8 degrees of motion at C5-6, no instability, and CT confirms minimal facet arthrosis. He is keen to avoid fusion. Outline your indications assessment and operative plan for cervical disc arthroplasty.”
“You are planning a C6-7 cervical disc arthroplasty. The patient is a 52-year-old woman with C7 radiculopathy. Describe the specific anatomic considerations at C6-7 and how they influence your approach and implant placement.”
“A 45-year-old man undergoes uneventful single-level C5-6 arthroplasty. On the first post-operative day he develops progressive neck swelling, dysphagia and stridor. What is your differential diagnosis and immediate management?”
Indications — patient selection
- Single- or two-level soft-disc radiculopathy or myelopathy with preserved motion greater than 5 degrees on dynamic radiographs
- Minimal facet arthrosis, no instability (translation less than 2 mm), no kyphosis greater than 10 degrees
- Failure of 6 weeks non-operative care; patient preference for motion preservation after informed consent
- Contraindications: ankylosis, severe spondylosis, osteoporosis (T-score less than -2.5), active infection, tumour, inflammatory disease
Surgical anatomy — key structures
- Smith-Robinson interval: between carotid sheath (lateral) and visceral column (medial) — protects recurrent laryngeal nerve and oesophagus
- Recurrent laryngeal nerve: higher risk on right at C6-7 — prefer left-sided approach at this level
- Sympathetic chain: on lateral border of longus colli 10-15 mm from midline — avoid aggressive lateral retraction
- Vertebral artery: enters C6 transverse foramen; limit lateral uncinate resection to medial half
- Endplate: preserve subchondral bone for implant stability; remove only cartilage
Operative technique — critical steps
- Confirm level with needle and fluoroscopy before deep dissection
- Left-sided approach at C6-7; blunt development of carotid-visceral plane
- Complete discectomy including posterior annulus and compressive uncovertebral osteophytes
- Endplate preparation preserving dense subchondral bone; match implant footprint
- Midline placement confirmed on AP fluoroscopy; cover at least 80 percent of endplate
- Restore 5-7 mm disc height and 5-7 degrees segmental lordosis without over-distraction
- Verify full nerve-root decompression with nerve hook before final implantation
- Immediate mobilisation without collar; dynamic radiographs at 6 weeks and 3 months
Complications — incidence and management
- Heterotopic ossification: 10-50 percent at 5 years; Grade III-IV causes motion loss; NSAID prophylaxis in high-risk patients
- Implant subsidence or migration: 2-5 percent; preserve subchondral bone, avoid over-distraction
- Recurrent laryngeal nerve injury: 1-3 percent hoarseness; higher on right at C6-7; left approach preferred
- Dysphagia: 5-15 percent transient; limit retraction time, relax retractors frequently
- Expanding haematoma: immediate re-exploration for airway compromise; consider drain in selected cases
- Oesophageal perforation: less than 0.5 percent; nasogastric tube in revision cases, blunt dissection
- Vertebral artery injury: less than 0.5 percent; pre-operative CT, limit lateral resection
Post-operative protocol
- Mobilise day of surgery or day 1; soft collar for comfort only
- Dynamic radiographs at 6 weeks, 3 months, 6 months, 12 months and annually
- Return to light work 2-4 weeks; full activities including sport by 3 months
- Surveillance for heterotopic ossification and adjacent-segment disease long-term
- Revision options for failure: conversion to ACDF, posterior decompression, rarely implant exchange
Evidence and outcomes versus ACDF
- FDA IDE trials show non-inferiority to ACDF at 2-7 years with better motion preservation
- Modest reduction in adjacent-segment re-operation (about 50 percent relative risk reduction at 7-10 years)
- Heterotopic ossification is the dominant device-specific complication and may eliminate the motion benefit
- Patient selection is the strongest predictor of durable motion preservation
- Long-term data beyond 10 years still maturing; informed consent must reflect this uncertainty
Background & Evidence
Why preserve motion. Cervical disc arthroplasty was developed to reduce the adjacent-segment degeneration that occurs in roughly 25-30 percent of patients at 10 years after ACDF. By preserving physiologic motion, the theoretical load transfer to adjacent discs and facets is reduced. Landmark trials. Multiple FDA Investigational Device Exemption trials (Prestige, ProDisc-C, Secure-C, PCM, Mobi-C) demonstrated non-inferiority to ACDF at 2 and 7 years, with superior preservation of range of motion and lower re-operation rates for adjacent-segment disease in some series. Heterotopic ossification. The most common device-specific complication. Incidence ranges from 10-50 percent at 5 years depending on implant design and patient factors. Grade III-IV HO eliminates the motion-preserving benefit and converts the arthroplasty into a de facto fusion. Adjacent-segment disease. Meta-analyses suggest a modest reduction in symptomatic adjacent-segment disease requiring surgery (approximately a 50 percent relative risk reduction at 7-10 years), but the absolute benefit remains small and long-term data beyond 10 years are still maturing.
References
Long-term Clinical Outcomes of Cervical Disc Arthroplasty: A Prospective, Randomized, Controlled Trial
Prospective RCT demonstrating sustained clinical benefit and preserved segmental motion at long-term follow-up after cervical disc arthroplasty compared with fusion. Cervical disc arthroplasty provides durable clinical outcomes and motion preservation beyond five years in appropriately selected patients. (Spine 2017;42(4):209-216; DOI 10.1097/BRS.0000000000001746)
Cervical disc arthroplasty with the Prestige LP disc versus anterior cervical discectomy and fusion, at 2 levels: a prospective, multicenter randomized controlled clinical trial at 24 months
Two-level Prestige LP arthroplasty demonstrated non-inferiority to ACDF with superior motion preservation and lower re-operation rates at 24 months. Two-level cervical disc arthroplasty is a safe and effective motion-preserving alternative to fusion with reduced adjacent-segment stress. (J Neurosurg Spine 2017;26(6):653-667; DOI 10.3171/2016.10.SPINE16264)
Cervical Disk Arthroplasty and Range of Motion at 7 Years: Impact on Adjacent Level Degeneration
Seven-year follow-up of an RCT cohort showed maintained range of motion at index levels and reduced radiographic adjacent-level degeneration compared with fusion. Preserved motion at seven years correlates with lower rates of adjacent segment degeneration, supporting the long-term benefit of arthroplasty. (Clin Spine Surg 2023;36(3):83-89; DOI 10.1097/BSD.0000000000001446)
Ten-year Outcomes of Cervical Disc Replacement With the BRYAN Cervical Disc: Results From a Prospective, Randomized, Controlled Clinical Trial
Ten-year RCT data for the BRYAN disc showed sustained clinical success, preserved motion, and lower rates of subsequent surgery versus ACDF. Long-term (10-year) evidence confirms durability of motion preservation and reduced re-operation risk with cervical disc arthroplasty. (Spine 2019;44(9):601-608; DOI 10.1097/BRS.0000000000002907)