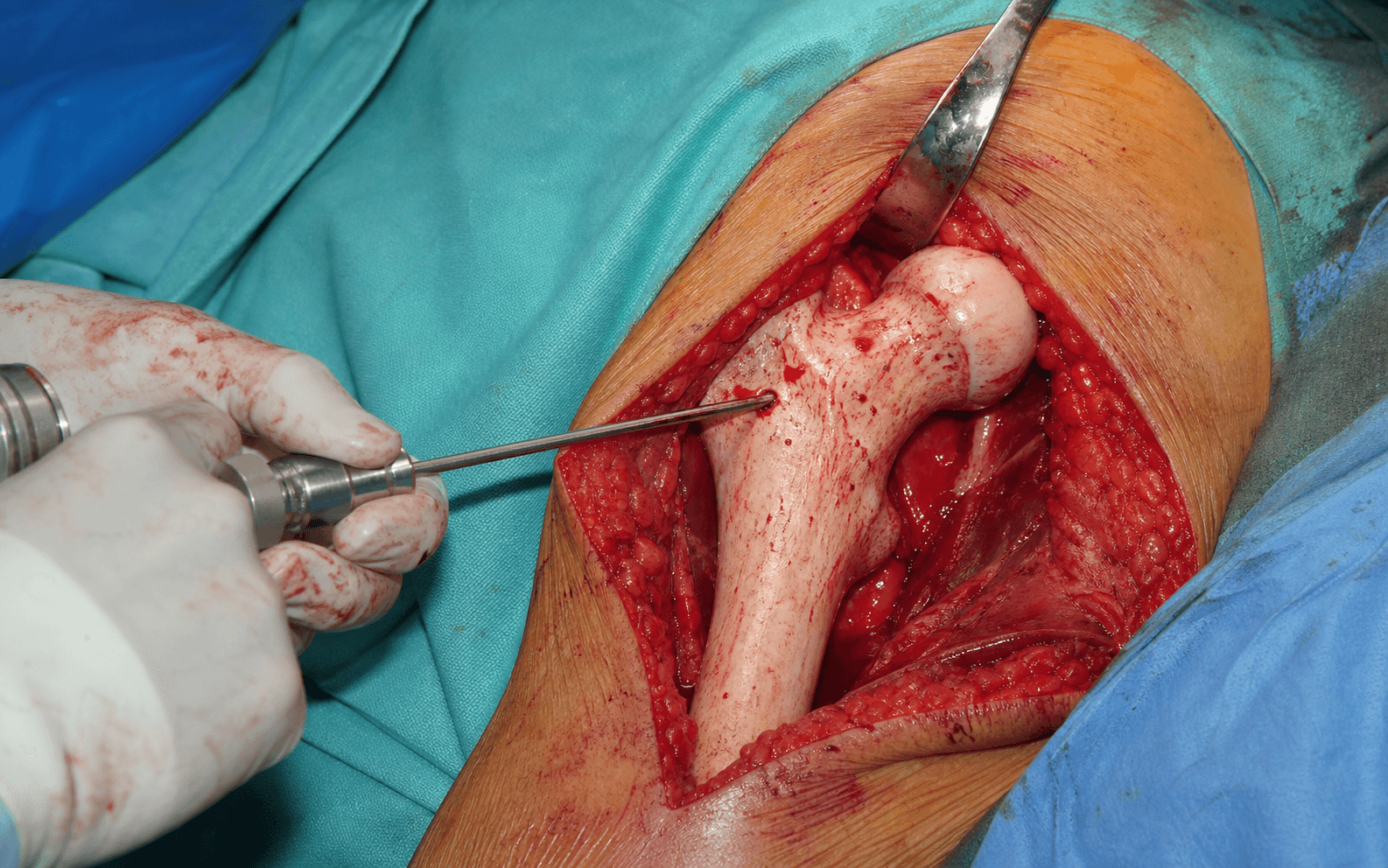
Percutaneous lateral approach through vastus lateralis for pre-collapse (Ficat/ARCO I–II) osteonecrosis · intermediate
- Indicated for pre-collapse (Ficat/ARCO Stage I–II) osteonecrosis that has failed conservative management (activity modification, bisphosphonates, protected weight-bearing) — a crescent sign is an absolute contraindication.
- Small to medium lesion size (less than 30 percent of the femoral head, less than 250 degrees Kerboul angle on MRI) — lesion size is the single most important prognostic factor.
- Young patient (less than 50 years, ideally less than 40) with preserved joint space (greater than 2 mm) — joint registries show a 25–30 percent THA revision rate at 10 years in young AVN patients, justifying aggressive preservation.
- Entry point 2–3 cm distal to the vastus ridge on the lateral femur, trajectory toward the anterosuperior weight-bearing dome, confirmed on biplanar fluoroscopy (AP and lateral) and stopped 5 mm short of the subchondral bone.
When & Why
Core decompression is a joint-preserving operation for the pre-collapse hip. By drilling a track from the lateral femoral cortex into the necrotic segment it relieves intraosseous pressure, stimulates reperfusion and removes a sample of bone for histology. The aim is to prevent collapse and buy time before an inevitable arthroplasty in a young patient — because once the head collapses, total hip arthroplasty in this group carries a markedly higher revision burden than arthroplasty for osteoarthritis. The single decision that governs everything: decompress the pre-collapse hip, replace the collapsed hip. A crescent sign (subchondral fracture, Ficat/ARCO Stage III) means the mechanical failure has already happened — decompression will not rescue it. Detailed staging lives in Background & Evidence, but the eligibility test is this:
- Pre-collapse disease (Ficat/ARCO Stage I–II) that has failed 3–6 months of conservative care - Small to medium lesion: less than 30 percent of the head, less than 250 degrees Kerboul angle - Young patient (less than 50, ideally less than 40) - Preserved joint space (greater than 2 mm) on a weight-bearing AP
- Crescent sign / established collapse (Ficat/ARCO Stage III–IV) — go to arthroplasty - Large lesion (greater than 30 percent, greater than 250 degrees Kerboul) — very high failure - Active septic arthritis or osteomyelitis - Significant osteoarthritis (joint space less than 2 mm, Tönnis 2–3)
- Asymptomatic Stage I–II disease in a high-risk patient (bilateral disease, ongoing steroid use) — controversial but may slow progression - Medium lesion (15–30 percent) — consider an adjunct (tantalum rod, vascularised fibula) - Ficat Stage IIC with a small crescent — most proceed to arthroplasty; a vascularised fibula is a selective salvage
- Elderly / low-demand patient (greater than 65) — THA is more predictable - Severe osteoporosis — fracture risk during and after the procedure - Morbid obesity (BMI greater than 40) — technical difficulty and high mechanical load - Patient unwilling to comply with 12 weeks of protected weight-bearing
Why preserve at all? National joint registries (AOANJRR, NJR, AJRR, SHAR, NZJR) consistently show that THA for osteonecrosis carries a higher revision burden than THA for primary osteoarthritis, driven by the younger, higher-demand population — commonly cited as roughly 25–30 percent revision at 10 years in AVN patients under 55, against 5–7 percent for OA. That risk is the rationale for an aggressive preservation attempt in the pre-collapse hip of a young patient. Consent specifically for: a realistic success rate that depends on stage and lesion size (not a guarantee), the possibility of progression to collapse and eventual arthroplasty, a small but serious risk of articular penetration or periprosthetic fracture, protected weight-bearing for 12 weeks, and (if a graft or rod is used) donor-site or hardware-related morbidity. Setup. Supine on a radiolucent table, hip in neutral rotation (a slight 10–15 degree internal rotation may relax the anterior capsule and improve visualisation). The whole operation depends on biplanar fluoroscopy, so test AP and lateral imaging and confirm a perfectly circular femoral head before draping. A first-generation cephalosporin (cefazolin 2 g IV, weight-adjusted) is given within 60 minutes of incision; vancomycin if beta-lactam-allergic or MRSA risk.
The Operation
The goal: pass a guidewire from the lateral femoral cortex, across the neck, into the centre of the necrotic segment in the anterosuperior weight-bearing dome, and decompress it to within 5 mm of the subchondral bone — without breaching the joint, the femoral neck cortices, or the posterior neurovascular structures. The exposure is a small percutaneous lateral approach through vastus lateralis, laid out in full as the first steps below.
Operative sequence
- Supine on a radiolucent table (a fracture table is optional but allows traction if needed for C-arm visualisation); hip in neutral rotation.
- Set the C-arm for biplanar imaging — AP pelvis (both hips visible, femoral head perfectly circular) and a cross-table or frog-leg lateral — and test it before draping.
- Mark the entry point under fluoroscopy: lateral thigh, 2–3 cm distal to the palpable vastus ridge.
- A 1–2 cm stab incision over the marked entry point.
- Tissue layers, in order: skin, subcutaneous fat, fascia lata (split in line with its fibres), then vastus lateralis by blunt dissection perpendicular to the muscle fibres down to the lateral femoral cortex.
- This is a muscle-splitting, internervous-friendly approach that stays on bone and well clear of the posterior structures; confirm the lateral cortex on both fluoroscopic views before any instrumentation.
- Plan the trajectory on both views and correlate with the preoperative MRI lesion location (typically the anterosuperior dome).
- AP view: directed medially and slightly superiorly toward the weight-bearing dome.
- Lateral view: directed anteriorly toward the mid-anterior third of the head — not extreme anterior (cortex perforation risk).
- Measure the depth from lateral cortex to subchondral bone on each view and subtract 5 mm for the safety margin.
- Pass a 2.0–2.4 mm smooth or threaded guidewire through the entry point; penetrate the lateral cortex with mallet taps or power and confirm intramedullary position.
- Advance across the neck toward the lesion centre, checking AP and lateral alternately and adjusting as needed.
- STOP 5 mm from the articular surface on BOTH views, using the depth markings on the wire.
- If the trajectory is off-target on either view, remove and redirect — it cannot be corrected after the core is drilled.
- Single large core (8–11 mm): a cannulated trephine or reamer over the wire, advanced with gentle pressure and frequent fluoroscopy; copiously irrigate to prevent thermal necrosis; stop at the predetermined depth; extract the solid core for histology (empty osteocyte lacunae confirm AVN and exclude tumour or infection).
- Multiple small cores (3–4 cores of 3.5 mm): drill the first wire track, leave it as a reference, then place 2–3 parallel wires 1 cm apart converging on the lesion centre and drill each; copiously irrigate all tracks; send a representative core for histology.
- Systematic reviews show no significant difference in outcome between the two; the choice turns on whether an adjunct graft or rod is planned.
- Tantalum rod (10–12 mm): for 15–30 percent / 200–250 degrees lesions; impact to within 5 mm of subchondral bone.
- Non-vascularised or vascularised fibula strut: structural support through the track (vascularised adds active revascularisation via a peroneal-to-LFCA anastomosis).
- BMAC: aspirate 60–120 ml from the iliac crest, concentrate, and inject into the track(s) — minimal added morbidity, limited evidence.
- See the adjunct table below for the honest evidence on each.
- Irrigate all tracks; bleeding is usually minimal given the avascular necrotic bone.
- Final fluoroscopy: appropriate depth (5 mm margin on both views), no articular penetration, no iatrogenic fracture of the neck, subtrochanteric region or shaft, and stable graft/rod position if used.
- Close in layers — fascia lata with 2-0 absorbable, subcutaneous 3-0 absorbable, skin with a 3-0 monocryl subcuticular suture or staples — and apply a sterile compressive dressing.
- AP and lateral radiographs in recovery document the baseline for follow-up.
Technique choice — single large core versus multiple small cores
- How it is done
- Cannulated trephine over the guidewire; removes a solid core for histology
- Advantages
- Allows a structural graft or tantalum rod; single pass; good central decompression
- Disadvantages
- Greater neck weakening and stress-riser fracture risk; longer protected weight-bearing
- How it is done
- First wire to lesion centre, then 2–3 parallel wires 1 cm apart, each drilled
- Advantages
- Less neck weakening; multiple drainage paths; shorter protected weight-bearing
- Disadvantages
- No structural graft possible; more radiation; wires must converge on the lesion
- Mechanism
- Structural support plus a porous scaffold (75–80 percent porosity) for host ingrowth
- Reported outcomes
- 50–70 percent in Stage II medium lesions — comparable to fibula and simpler
- Caveats
- No active blood supply; retrieval showed minimal ingrowth (mean 1.9 percent); no RCT benefit over core alone; complicates later THA
- Mechanism
- Structural strut AND active revascularisation via the peroneal artery
- Reported outcomes
- 70–90 percent even in selected Stage III disease — the best salvage
- Caveats
- 4–6 hour procedure; microsurgery; donor morbidity (ankle stiffness, peroneal palsy); hard to revise to THA
- Mechanism
- Structural support only — an internal splint
- Reported outcomes
- 40–60 percent — better than core alone for medium lesions
- Caveats
- No revascularisation; may resorb over time
- Mechanism
- Theoretical stem-cell and growth-factor enhancement of revascularisation
- Reported outcomes
- Conflicting — some report 10–15 percent improvement, others none
- Caveats
- Minimal added morbidity; no structural support; needs a centrifuge
Articular cartilage penetration is rare (less than 0.1 percent with proper technique) but catastrophic when it occurs — rapid joint destruction that usually needs salvage arthroplasty within 6–12 months. It is prevented by a mandatory 5 mm safety margin from the subchondral bone on BOTH AP and lateral fluoroscopy, depth markings on the wire, measuring cortex-to-subchondral distance before drilling, and biplanar checks during every advance. A single view cannot judge a 3D trajectory — if you are tempted to rely on one, stop and re-image.
The trajectory from lateral cortex to the anterosuperior lesion is three-dimensional. Check AP and lateral alternately with every advance of the wire, and correlate the target with the preoperative MRI. On the lateral view aim for the mid-anterior third of the head, never the extreme anterior cortex (thin, easily perforated, especially in osteoporotic bone). Stop 5 mm short of subchondral bone on both views.
Place the entry 2–3 cm distal to the vastus ridge. Too proximal (into the greater trochanter) risks a trochanteric fracture and endangers the superior gluteal neurovascular bundle; too distal creates a subtrochanteric stress riser that can fracture weeks later. Avoid cores greater than 11 mm, and for large cores extend non-weight-bearing to 8–12 weeks.
Five danger structures you protect during the approach
Posterior to the femur in the adductor compartment; 3–4 perforating branches cross through the lateral intermuscular septum. Protect by staying on the lateral cortex with blunt, perpendicular vastus split — never dissect posterior to the septum.
Posterior to the hip, about 3–5 cm posterior to the shaft. The lateral percutaneous approach stays well anterior; keep the hip neutral and avoid excessive flexion.
Exits above piriformis and runs between gluteus medius and minimus, 3–5 cm above the greater trochanter tip. The entry point 2–3 cm distal to the vastus ridge keeps you below it — confirm on AP before incision.
Overlies the femoral head, separated from the necrotic zone by a 2–5 mm subchondral plate. Protect with the mandatory 5 mm margin on both views and depth control — breach is the disaster to avoid.
Thin (2–3 mm) and easily perforated by an excessive anterior trajectory. Aim for the mid-anterior third on the lateral view; if the wire perforates the anterior cortex, remove and redirect, and confirm no breach on final fluoroscopy.
Aftercare & Complications
Weight-bearing is the make-or-break of success. The decompressed head needs 3–6 months to revascularise; uncontrolled loading during that window is a direct cause of collapse. The protected-weight-bearing window is therefore non-negotiable.
- Timing
- 0–6 weeks
- Weight-bearing
- Non-weight-bearing (crutches or walker)
- Therapy
- Supine ROM (flexion, abduction, external rotation), ankle pumps, quad sets, transfer training; aquatic therapy if available
- Timing
- 6–12 weeks
- Weight-bearing
- Touch-down (10–20 kg foot contact only)
- Therapy
- Hip and core strengthening (isometric then resisted), proprioception, gait with an aid
- Timing
- 3–6 months
- Weight-bearing
- Progressive to full if X-rays are stable
- Therapy
- Advanced lower-limb and core strengthening; sport-specific training
- Timing
- Beyond 6 months
- Weight-bearing
- Full (if stable)
- Therapy
- Gradual return to impact activities; continue monitoring for pain or mechanical symptoms
- Recognition
- New crescent or progressive flattening with joint-space narrowing on serial X-rays; worsening pain and ROM; MRI persistent oedema; typically within 18–24 months
- Prevention
- Operate only on pre-collapse I–II small–medium lesions (less than 30 percent); accurate staging; protected WB for 12 weeks; adjuncts for medium–large lesions; realistic counselling
- Management
- THA is the usual salvage (25–30 percent revision at 10 years in young AVN, per AOANJRR). For the very young (less than 35), vascularised fibula salvage (60–80 percent)
- Recognition
- Intra-op: wire or drill advances past the planned depth with loss of resistance; fluoro shows subchondral breach. Post-op: rapid severe pain, effusion, fast progressive arthritis
- Prevention
- Mandatory 5 mm margin from subchondral bone on BOTH AP and lateral; depth markings; measure cortex-to-subchondral distance before drilling; biplanar checks during advancement
- Management
- If intra-op: stop, remove instruments, consider aborting. Post-op: protected WB and close monitoring; rapid joint destruction usually needs salvage THA within 6–12 months
- Recognition
- Sudden lateral thigh pain during the protected-WB phase; unable to bear weight; X-ray fracture at the entry point
- Prevention
- Entry 2–3 cm distal to the vastus ridge (not too proximal or distal); avoid cores greater than 11 mm; prefer multiple small cores; gradual WB progression; extended NWB for large cores
- Management
- Non-displaced: protected NWB 6–12 weeks. Displaced: cephalomedullary nailing; avoid early full WB (the head is still at risk)
- Recognition
- Intra-op: loss of wire position, visible fracture line on fluoro. Post-op: groin pain, unable to bear weight; shortened and externally rotated leg if displaced
- Prevention
- Gentle reaming; limit single large cores (greater than 10 mm higher risk); protected WB 6–12 weeks; prefer multiple small cores in osteoporotic bone
- Management
- Non-displaced (intra-op): abort, percutaneous screws, prolonged NWB. Displaced or post-op: likely arthroplasty — the head is already compromised
- Recognition
- Fever, wound erythema or drainage, increasing hip pain and effusion; raised WCC, CRP, ESR; aspirate grows Staph aureus
- Prevention
- Cefazolin 2 g IV within 60 min of incision (vancomycin if allergic or MRSA risk); sterile technique; minimise soft-tissue trauma; routine post-op antibiotics not indicated
- Management
- Aspirate for culture; empiric IV anti-staphylococcal antibiotics; irrigation and debridement (remove graft or rod); 6 weeks organism-specific IV antibiotics; salvage THA only after infection control
- Recognition
- Pain unchanged at 3–6 months despite compliance; X-rays may be stable or subtly progressive; MRI persistent oedema
- Prevention
- Exclude OA, labral tear, impingement and spine pain pre-operatively; realistic counselling on success rates; address risk factors (steroids, alcohol, bone health)
- Management
- Systematic re-evaluation (X-ray, MRI, aspirate); if stable, conservative care; if progressing, arthroplasty; treat any other identified pathology
- Recognition
- Iliac crest: donor pain, lateral femoral cutaneous nerve injury, haematoma. Fibula: ankle stiffness (20–30 percent), peroneal palsy (5–10 percent), chronic pain (15–25 percent)
- Prevention
- Iliac: protect the LFCN (2–3 cm medial to ASIS), meticulous haemostasis. Fibula: protect the peroneal nerve, limit harvest to 8–12 cm, preserve 6 cm of distal fibula, early ankle ROM
- Management
- Usually self-limiting; analgesia and physio; LFCN injury usually neuropraxia; peroneal palsy mostly recovers over 6–12 months (AFO meanwhile)
Recognising failure and the salvage options. Most failures declare within 18–24 months (but can occur up to 3–5 years) as progressive collapse, joint-space narrowing beyond 1 mm, or worsening pain despite initial improvement. Salvage options: - Total hip arthroplasty — the standard and most common salvage; good outcomes but a high revision rate in young AVN patients (registries: roughly 25–30 percent at 10 years versus 5–7 percent for OA).
- Vascularised fibula graft — a salvage attempt for the very young (less than 35) with small–medium lesions who have failed core decompression (60–80 percent success in carefully selected cases); buys time before an inevitable THA.
- Hip resurfacing — controversial; bone-quality concerns and inferior registry survivorship in osteonecrosis versus OA; not mainstream for AVN.
- Rotational osteotomy (Sugioka / transtrochanteric) — mainly in specialist East-Asian centres; rotates the defect away from the weight-bearing zone; only for small contained anterosuperior lesions; technically demanding with unpredictable outcomes.
Viva & Exam Focus
FACEFACE — Ficat staging (and when you may decompress)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 38-year-old man on long-term steroids for lupus has bilateral hip pain. X-rays show bilateral Ficat Stage II AVN. MRI shows a 25 percent lesion (220 degrees Kerboul) on the right and a 10 percent lesion (150 degrees Kerboul) on the left. How would you manage each hip?”
“Explain the significance of the crescent sign on X-ray. How do you identify it and what are the implications for core decompression?”
“Compare and contrast vascularised fibula grafts versus tantalum rods as adjuncts to core decompression. When would you use each?”
Indications
- Pre-collapse (Ficat/ARCO I–II) AVN failing 3–6 months of conservative care
- Small–medium lesion: less than 30 percent head, less than 250 degrees Kerboul — size is the key prognostic factor
- Young patient (less than 50, ideally less than 40) with joint space greater than 2 mm
- Crescent sign (Stage III) = absolute contraindication — go to arthroplasty
Anatomy & target
- MFCA is the dominant head supply (80–90 percent); AVN follows MFCA interruption
- Typical lesion: anterosuperior weight-bearing dome (MFCA–LFCA watershed) — the target
- Entry point 2–3 cm distal to the vastus ridge, confirmed on AP and lateral fluoro
- Five danger zones: profunda perforators, sciatic nerve, superior gluteal bundle, articular cartilage, femoral neck anterior cortex
The critical steps
- Stage with Ficat, ARCO and Kerboul angle (less than 200 degrees good, greater than 250 degrees poor)
- Biplanar fluoroscopy is mandatory — trajectory cannot be judged from one view
- Advance the guidewire to the lesion centre, STOP 5 mm from subchondral bone on BOTH views
- Single large core (8–11 mm) allows a graft; multiple small cores (3–4 × 3.5 mm) weaken the neck less — similar outcomes
Aftercare
- NWB 4–6 weeks, then touch-down 4–6 weeks — 12 weeks protected total
- X-rays at 6 weeks, 3, 6 (most failures), 12 months, then annually for 5+ years
- MRI at 3–6 months predicts outcome (falling oedema = success)
- Bisphosphonate adjunct for steroid-induced AVN — mixed evidence, not a substitute for surgery
Complications
- Head collapse despite treatment (30–60 percent) — most common; salvage with THA
- Articular cartilage penetration (less than 0.1 percent but catastrophic) — prevented by the 5 mm margin
- Subtrochanteric fracture (0.5–2 percent) — stress riser at the entry point
- Femoral neck fracture (0.5–1 percent) during or after reaming
Exam tips
- Crescent sign = subchondral fracture = Ficat III = absolute contraindication
- Lesion size drives prognosis: less than 200 degrees or 15 percent = 80–90 percent success; greater than 250 degrees or 30 percent = 30–40 percent
- Adjuncts: tantalum (simple, no donor morbidity, no RCT benefit over core alone); vascularised fibula (best salvage, morbidity)
- Registries (AOANJRR, NJR, AJRR, SHAR): higher THA revision in young AVN than OA — justifies preservation; ARCO 2019 is the consensus system; cefazolin 2 g IV within 60 min (vancomycin if allergic or MRSA risk)
Background & Evidence
Epidemiology. Non-traumatic osteonecrosis of the femoral head is a disease of younger adults (peak 30–50 years) driven by corticosteroid use, alcohol excess, sickle-cell disease and other haemoglobinopathies, decompression sickness, and idiopathic causes; traumatic AVN follows femoral-neck and displaced femoral-head fractures. Non-traumatic disease is bilateral in 30–70 percent of cases, so the contralateral hip must always be imaged and counselled about. Pathoanatomy — why the head dies and collapses. The femoral head is supplied predominantly by the medial femoral circumflex artery (MFCA, 80–90 percent via the posterosuperior retinacular vessels), with a minor contribution from the lateral femoral circumflex artery (10–20 percent) and a negligible adult contribution from the artery of the ligamentum teres. The typical AVN lesion sits in the anterosuperior weight-bearing dome — the watershed zone between MFCA and LFCA territories — which is the operative target. Interruption of the MFCA supply (trauma, emboli, thrombosis) leads to ischaemia, osteocyte death, a necrotic zone, then mechanical failure of the dead bone, a subchondral fracture (the crescent sign) and finally collapse and arthritis. Core decompression intervenes in the pre-collapse phase by relieving intraosseous pressure and stimulating reperfusion. Staging — know both systems (and the size quantification).
- Imaging
- Normal X-ray; MRI shows marrow oedema or necrosis
- Status
- Pre-collapse — decompression candidate
- Imaging
- Sclerosis, cysts, porosis; NO collapse
- Status
- Pre-collapse — decompression candidate
- Imaging
- Crescent sign (subchondral fracture); early collapse
- Status
- Post-collapse — too late for decompression
- Imaging
- Flattening, head deformity, secondary acetabular arthritis
- Status
- End-stage — arthroplasty
- Definition
- Normal imaging; high-risk patient (bilateral disease, steroids)
- Definition
- Normal X-ray, MRI positive — subdivided by lesion size (less than 15 percent, 15–30 percent, greater than 30 percent)
- Definition
- Abnormal X-ray, no collapse — subdivided by lesion size
- Definition
- Subchondral fracture (crescent) — subdivided by flattening (less than 2 mm, 2–4 mm, greater than 4 mm)
- Definition
- Acetabular involvement
- Success with core decompression
- 80–90 percent
- Success with core decompression
- 50–70 percent
- Success with core decompression
- 30–40 percent
Success rates by combined stage and size (the most predictive pairing):
- Success at about 5 years
- 85–90 percent
- Success at about 5 years
- 60–75 percent
- Success at about 5 years
- 40–50 percent
- Success at about 5 years
- 70–80 percent
- Success at about 5 years
- 45–60 percent
- Success at about 5 years
- 30–40 percent
Key evidence — the honest message on adjuncts. Mont and colleagues established that joint-preserving procedures are indicated for pre-collapse disease and that, once collapse has occurred, THA gives excellent results beyond ten years — the paradigm that anchors the decompress-versus-replace rule. The systematic review by Marker showed core decompression is safe and effective for early disease, with the best results in small lesions and Stage I, and that improvement over historical results came substantially from better patient selection rather than technique alone. The network meta-analysis of RCTs by Liu (17 RCTs, 784 patients, 918 hips) found core decompression with cell therapy ranked best for limiting radiographic progression, but no significant difference between any joint-preserving method and non-surgical treatment for conversion to THA — which tempers claims that structural adjuncts outperform core decompression alone. Tanzer's retrieval analysis of 15 failed porous tantalum implants explained why: residual osteonecrosis in 14 of 15, subchondral fracture in all, collapse in 60 percent, and minimal bone ingrowth (mean 1.9 percent). Yoo's long-term vascularised-fibula series (124 hips, mean 13.9 years) supports the fibula as a durable option for selected hips, including some post-collapse disease, accepting microsurgical complexity and donor morbidity. This consistent evidence base is why core decompression alone is the default for small lesions and why adjuncts are reserved for medium–large lesions or salvage. Guidelines, registries and global practice. - Registry evidence (arthroplasty for AVN). AOANJRR (Australia), NJR (England, Wales and Northern Ireland), AJRR (USA), SHAR (Sweden) and NZJR all report osteonecrosis as a risk factor for earlier revision relative to OA, with age the dominant confounder; common failure modes are aseptic loosening, instability or dislocation, and periprosthetic fracture. This underpins the rationale for joint-preserving surgery in the pre-collapse hip.
- Diagnosis and staging consensus. The ARCO 2019 revised classification is the current international consensus staging system; stage and lesion size or location remain the key prognostic determinants, and MRI is the most sensitive modality for pre-collapse disease across all guidelines.
- Pharmacological adjuncts — global view. Bisphosphonates (alendronate, or annual IV zoledronic acid) are used in many centres for corticosteroid-associated osteonecrosis to slow progression, though evidence is mixed and they are not a substitute for joint-preserving surgery in symptomatic pre-collapse disease; statins and anticoagulants have been trialled for prophylaxis in high-risk steroid users with limited evidence.
- Surgical antibiotic prophylaxis — side by side. Most national guidance (AAOS, BOA or UK, AO Foundation, WHO surgical safety) recommends a first-generation cephalosporin (cefazolin 2 g IV, weight-adjusted) within 60 minutes of incision; for beta-lactam allergy or MRSA risk, vancomycin (15–20 mg/kg over 60–120 minutes) or teicoplanin per local protocol. A single dose is sufficient for this short percutaneous procedure; routine post-operative antibiotics are not indicated.
References
Nontraumatic Osteonecrosis of the Femoral Head: Where Do We Stand Today? A Ten-Year Update
- Comprehensive review establishing that joint-preserving procedures are indicated for pre-collapse disease, with successful mid- and long-term outcomes in selected patients
- Once collapse has occurred, total hip arthroplasty gives excellent results at greater than ten years — a paradigm shift in management
- Hemiresurfacing and total resurfacing arthroplasty gave suboptimal results and have restricted indications in osteonecrosis
Do modern techniques improve core decompression outcomes for hip osteonecrosis?
- Multiple small-diameter drilling cohort (52 patients, 79 hips) confirmed core decompression is safe and effective for early-stage osteonecrosis
- Best results in small lesions and Ficat Stage I (79 percent with no radiographic progression)
- Improvement over historical results was substantially explained by better patient selection (fewer Stage III hips), not technique alone
Efficacy of various core decompression techniques versus non-operative treatment for osteonecrosis of the femoral head: a systematic review and network meta-analysis of RCTs
- Network meta-analysis of 17 RCTs (784 patients, 918 hips) across seven interventions including core decompression alone, with bone graft, with tantalum rod, with cell therapy, and vascularized bone graft
- Core decompression with cell therapy ranked best for limiting radiographic progression (SUCRA 96.4 percent)
- NO significant difference between any joint-preserving method and non-surgical treatment for conversion to THA
Histopathologic retrieval analysis of clinically failed porous tantalum osteonecrosis implants
- Retrieval analysis of 15 failed porous tantalum implants from Steinberg Stage II hips converted to THA
- Residual osteonecrosis in 14 of 15, subchondral fracture in all, and femoral head collapse in 60 percent
- Bone ingrowth confirmed in 87 percent of specimens but extent was minimal (mean 1.9 percent, range 0 to 4.4 percent) — insufficient mechanical support of subchondral bone
Long-term followup of vascularized fibular grafting for femoral head necrosis
- 110 patients (124 hips) followed a mean of 13.9 years after free vascularized fibular grafting
- Mean Harris Hip Score improved from 72 to 88; only 13 hips (10.5 percent) converted to THA
- Graft survival was associated with patient age and lesion size or location, but NOT with disease stage or etiology; donor-site morbidity included great-toe clawing and partial peroneal nerve palsy
Osteonecrosis of the femoral head. A prospective randomized treatment protocol
- Prospective RCT (55 hips) comparing core decompression with conservative treatment
- Decompression outperformed conservative care in early stages (e.g. Stage I 70 percent versus 20 percent; Stage II 71 percent versus 0 percent by Harris Hip Score)
Idiopathic bone necrosis of the femoral head. Early diagnosis and treatment
The classic paper defining the Ficat staging system (I–IV) for AVN from radiographic findings: Stage I–II are pre-collapse (core decompression candidates) and Stage III–IV are post-collapse.
The conservative surgical treatment of idiopathic aseptic necrosis of the femoral head
The original description of the Kerboul angle method for quantifying lesion size on imaging, establishing its prognostic value (less than 200 degrees good, greater than 250 degrees poor outcomes).
A quantitative system for staging avascular necrosis
The University of Pennsylvania or Steinberg staging system, adding quantification to the Ficat system and emphasising lesion size as a prognostic factor (the basis of the modern ARCO quantified subgroups).
Prevalence of nontraumatic osteonecrosis of the femoral head and its associated risk factors in the Chinese population
A nationally representative survey reporting 30–70 percent bilateral involvement in non-traumatic AVN, underlining the need to image and monitor the contralateral hip.
National joint registries (AOANJRR, NJR, AJRR, SHAR, NZJR) — annual arthroplasty reports
Registry evidence consistently shows higher THA revision rates in young patients with osteonecrosis than in age-matched osteoarthritis, supporting aggressive joint preservation in the pre-collapse hip.