Posterolateral extrapleural access to the thoracic vertebral body and disc via rib and transverse process resection
- A paramedian or J-shaped incision over the rib two levels above the target vertebra.
- Resect the transverse process and 4-6 cm of proximal rib to reach the lateral vertebral body.
- Maintain an extrapleural plane throughout - identify and protect the parietal pleura.
- Ligate or protect the intercostal neurovascular bundle at each level.
- The spinal cord lies medially - never retract it; work strictly lateral to the pedicle around the exiting root.
When & Why
What it exposes. The costotransversectomy gives direct posterolateral, extrapleural access to the lateral vertebral body, the disc space and the rib head / costovertebral junction, without entering the pleural cavity. It is the classic route for thoracic disc herniation, vertebral body biopsy, debridement of infection or tumour, drainage of paraspinal abscess, and limited anterolateral cord decompression. Primary indications.
- Thoracic disc herniation (soft or calcified) causing myelopathy or radiculopathy.
- Vertebral body biopsy for suspected tumour or infection.
- Debridement of pyogenic spondylodiscitis or tuberculous spondylitis with a paravertebral abscess.
- Limited anterolateral decompression for anterior cord compression (metastasis, burst fracture).
- Drainage of paraspinal or epidural abscess when a posterior approach is insufficient.
- Excision of rib head or costovertebral joint pathology. Why this approach. It provides direct posterolateral extrapleural access to the lateral vertebral body and disc while avoiding the morbidity of a thoracotomy, and gives far better access to the anterior column than a pure posterior approach. It is ideal when the pathology is lateral or anterolateral and the surgeon wishes to spare the lung, the great vessels and the sympathetic chain that are encountered in a transthoracic route. Contraindications.
- Pathology requiring extensive anterior column reconstruction (consider transthoracic or combined).
- Severe pulmonary disease precluding even brief single-lung ventilation if a pleural breach occurs.
- Previous ipsilateral thoracotomy or pleurodesis likely to obliterate the extrapleural plane.
- Midline anterior pathology best addressed by sternotomy or a transthoracic route.
- Inability to tolerate prone or lateral positioning (rare).
- Trajectory
- Transpleural, direct anterior
- Best for
- Midline calcified discs needing extensive anterior reconstruction; higher morbidity, routine chest drain
- Trajectory
- More lateral, muscle-splitting, more anterior
- Best for
- Wider anterior visualisation; more extensive
- Trajectory
- Purely posterior
- Best for
- Biopsy only; very limited anterior access
- Trajectory
- Posterior
- Best for
- Insufficient for anterior pathology; risks cord manipulation
- Trajectory
- Both
- Best for
- Circumferential tumours or severe deformity
- Description
- Unilateral paramedian, single level
- Typical use
- Thoracic disc herniation
- Description
- Two or more ribs resected
- Typical use
- Tumour or infection debridement
- Description
- Contralateral approach at a second stage
- Typical use
- Circumferential pathology
Position. Prone on a radiolucent table (Jackson or Wilson frame with chest rolls), or lateral decubitus (affected side up) when conversion to thoracotomy may be needed. Head neutral on a padded headrest or Mayfield pins; arms abducted less than 90 degrees; slight reverse Trendelenburg to reduce venous bleeding; knees flexed to relax the hamstrings. Confirm the level with preoperative imaging and skin marking; have a C-arm or O-arm available and tested for anteroposterior and lateral views; use neuromonitoring (MEP/SSEP) when available for myelopathic patients.
Prone spine positioning carries risks of facial swelling, brachial plexus stretch, ischaemic optic neuropathy and pressure sores. Pad all pressure points, keep the shoulders abducted less than 90 degrees, limit operative time, and check the eyes, ears and pressure points every 30 minutes.
Surface landmarks.
- Spinous processes palpable in the midline; the T7 spinous process lies at the level of the inferior angle of the scapula (superior angle marks T3).
- Paraspinal gutter - the depression lateral to the spinous processes where the erector spinae bulge lies.
- Ribs - count from the twelfth rib upwards (more reliable than from the first rib).
- Incision - a paramedian or gently curved J-shaped incision, 8-12 cm long and 4-5 cm lateral to the midline, centred over the rib that articulates with the superior half of the target disc space (the rib two levels above the target vertebra). Confirm the correct rib with fluoroscopy before the skin incision.
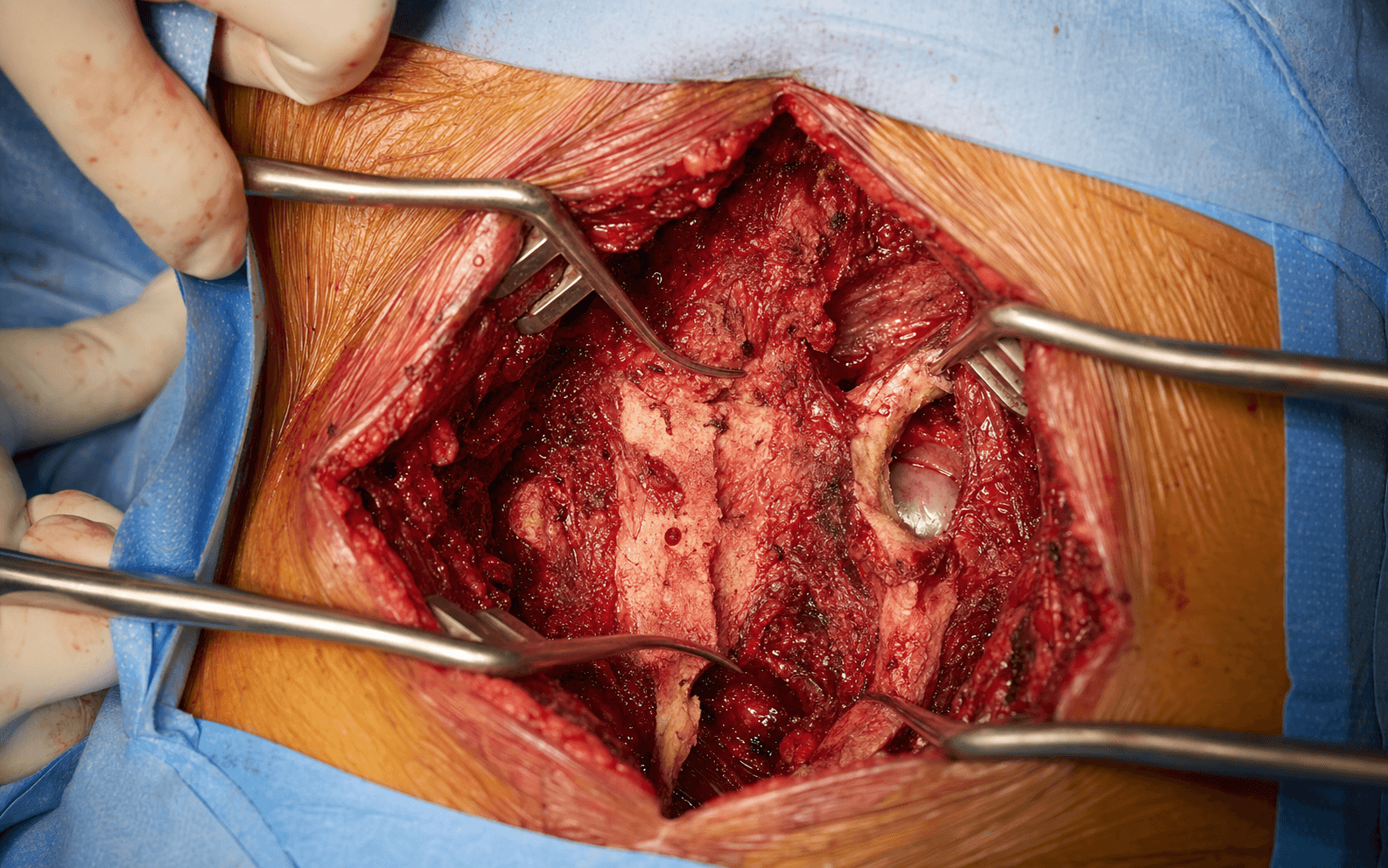
The Exposure
Work down through the paraspinal layers, resect the transverse process and the proximal rib, then develop the extrapleural plane lateral to the pedicle to reach the vertebral body and disc - all while the spinal cord stays safely medial and untouched.
Anatomy that governs the dissection. Each rib articulates with the vertebral body at the costovertebral and costotransverse joints (except the first, eleventh and twelfth ribs). The transverse process projects posterolaterally and the rib head lies immediately anterior to it, articulating with the body and disc - so resecting the transverse process and proximal rib removes the bony obstacles to the lateral vertebral body. The approach passes through the trapezius (upper thoracic) or latissimus dorsi (lower thoracic), then the erector spinae (longissimus and iliocostalis), developing the plane between the erector spinae and the rib cage. The intercostal neurovascular bundle runs in the subcostal groove on the inferior border of each rib (vein-artery-nerve from superior to inferior) and must be identified before rib resection; segmental radicular arteries feed the anterior spinal artery, and the artery of Adamkiewicz (great radicular artery) usually enters on the left between T9 and T12. The parietal pleura lines the inner rib cage and is loosely attached to the vertebral bodies - its reflection is more posterior at the costovertebral junction, which is what makes extrapleural access possible. Internervous plane. There is no true internervous plane. The dissection is intermuscular between the erector spinae (dorsal rami) medially and the intercostal muscles and external oblique (ventral rami via intercostal nerves) laterally, developed by subperiosteal elevation of the paraspinal muscles off the ribs and transverse processes. No motor nerves are divided in the superficial dissection. Safety comes from staying extrapleural and strictly lateral to the pedicle - the exiting nerve root is the only neural structure that may be sacrificed.
The costotransversectomy is an intermuscular, extrapleural, posterolateral approach. Stay in the plane immediately outside the pleura and work lateral to the pedicle. The exiting nerve root is the only nerve that may be sacrificed; the spinal cord and the contralateral structures are never exposed or retracted.
Exposure sequence
- Make a paramedian or gently curved J-shaped incision 8-12 cm long, 4-5 cm lateral to the midline, over the rib two levels above the target vertebra; the superior limb curves medially toward the spinous process.
- Incise the skin and subcutaneous tissue and divide the trapezius (upper thoracic) or latissimus dorsi (lower thoracic) in line with the incision.
- Identify the lateral border of the erector spinae.
- Elevate the erector spinae (longissimus and iliocostalis) subperiosteally from the rib and transverse process using Cobb elevators and electrocautery, working distal to proximal and retracting the muscle mass medially.
- Expose the rib from its angle to the costotransverse joint and the entire transverse process. No motor nerves are divided in this intermuscular plane.
- Before any osteotomy, identify the intercostal neurovascular bundle in the subcostal groove on the inferior border of the rib (vein-artery-nerve from superior to inferior).
- Dissect it free with a right-angle clamp and pass a vessel loop; ligate it only at the level of pathology if exposure demands, protecting the bundle at adjacent levels to avoid cord ischaemia from segmental artery compromise.
- Osteotomize the transverse process at its base with a Leksell rongeur or osteotome and remove it completely.
- This exposes the costovertebral joint and the lateral aspect of the vertebral body and pedicle.
- Resect 4-6 cm of the proximal rib including the costotransverse and costovertebral joints, using a rib cutter or Gigli saw.
- Protect the pleura with a thin malleable retractor or moist patties during the osteotomy; remove the rib head completely for anterior access.
- Gently dissect the parietal pleura away from the lateral vertebral body and disc using blunt finger dissection and moist neuro patties, maintaining the extrapleural plane.
- If a small pleural tear occurs, plan to repair it primarily or cover it with a pleural flap.
- Identify the exiting nerve root in the neural foramen, just below the pedicle.
- Retract it gently, or sacrifice it if required for disc or body access - patients tolerate unilateral thoracic root sacrifice well. Work strictly lateral to the pedicle.
- Remove the lateral cortex of the vertebral body with rongeurs or a high-speed burr; access the disc space by resecting the posterior longitudinal ligament if necessary.
- For disc herniation, remove the fragment with pituitary rongeurs and curettes; for debridement, remove necrotic bone and disc material. The spinal cord lies immediately medial - never place any instrument or retractor against the thecal sac.
The spinal cord lies immediately medial to the operative field. All work is performed lateral to the pedicle and the exiting root. Any direct trauma or retraction of the cord causes irreversible myelopathy. If cord visualisation is required, this approach is insufficient - convert to a laminectomy or a transthoracic route.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Dorsal rami cutaneous branches
- Protection
- Identify and preserve if possible; divide only if necessary
- Structure at risk
- Intercostal neurovascular bundle (subcostal groove)
- Protection
- Identify before osteotomy; ligate at the level of pathology only
- Structure at risk
- Parietal pleura
- Protection
- Blunt dissection with moist patties; repair small tears
- Structure at risk
- Exiting nerve root
- Protection
- Sacrifice only if required for exposure; protect at adjacent levels
- Structure at risk
- Spinal cord / thecal sac
- Protection
- Never retract; work strictly lateral to the pedicle
- Structure at risk
- Segmental radicular arteries (artery of Adamkiewicz)
- Protection
- Preserve when possible, especially left T9-T12
Consequence of injury.
- Spinal cord injury - permanent paraplegia, and bowel, bladder and sexual dysfunction.
- Intercostal artery ligation at multiple levels - anterior spinal artery syndrome.
- Pleural injury - pneumothorax, haemothorax, pleural effusion, empyema.
- Nerve root sacrifice - unilateral thoracic radiculopathy (usually tolerable).
- Sympathetic injury - Horner syndrome (ptosis, miosis, anhidrosis) if above T1.
- Prevention
- Blunt extrapleural dissection, moist patties
- Management
- Primary repair or pleural flap; chest drain if large
- Prevention
- Identify the bundle before osteotomy
- Management
- Bipolar cautery or ligation
- Prevention
- Never retract the cord; stay lateral to the pedicle
- Management
- Immediate steroids (controversial), imaging, supportive care
- Prevention
- Fluoroscopy before incision; count ribs from T12
- Management
- Immediate re-exploration if recognised
- Prevention
- Gentle retraction; sacrifice only if necessary
- Management
- Unilateral thoracic root loss is usually tolerable
- Incidence
- 5-15%
- Prevention
- Meticulous pleural inspection; chest drain if a tear
- Treatment
- Chest drain, respiratory support
- Incidence
- 2-5%
- Prevention
- Prophylactic antibiotics, layered closure
- Treatment
- Antibiotics; debridement if deep
- Incidence
- 1-3%
- Prevention
- Neuromonitoring, gentle technique
- Treatment
- Steroids, imaging, possible re-exploration
- Incidence
- 5-10%
- Prevention
- Chest drain if a pleural breach
- Treatment
- Observation or drainage
- Incidence
- 10-20%
- Prevention
- Minimise root manipulation
- Treatment
- Analgesia, gabapentinoids, nerve block
- Incidence
- Less than 1%
- Prevention
- Avoid deep anterior dissection above T1
- Treatment
- Observation (often resolves)
Pleural injury is the most common intra-operative complication of costotransversectomy. Small tears are repaired with absorbable suture or covered with a pleural flap. Larger defects or a persistent air leak require a 28 Fr chest drain connected to an underwater seal. A post-operative chest radiograph is mandatory in every patient to exclude pneumothorax or haemothorax.
Extensile options.
- Proximal extension along the paraspinal gutter, resecting additional ribs and transverse processes for multilevel pathology; the scapula may need mobilising for upper thoracic levels (T1-T4).
- Distal extension for lower thoracic or thoracolumbar disease - the approach can reach the L1-L2 disc if the twelfth rib is resected, though the lumbar plexus and psoas become relevant below T12.
- Bilateral staged approach - a contralateral costotransversectomy at a second stage achieves circumferential decompression for tumours or severe deformity while avoiding single-stage bilateral morbidity.
- Combined with posterior stabilisation - pedicle screw instrumentation through a separate midline or extended paramedian incision, before or after decompression.
- Conversion to thoracotomy - if the extrapleural plane is obliterated or more anterior access is needed, enter the pleural cavity (requires a chest drain and respiratory support). Closure.
- Inspect the pleura; repair small tears with 3-0 absorbable suture, or insert a 28 Fr chest drain through a separate stab for large tears or a persistent air leak.
- Achieve meticulous haemostasis (intercostal vessels are the commonest source of bleeding); use bipolar cautery on the muscle edges and irrigate copiously.
- Layered closure: approximate the erector spinae to the rib remnants with absorbable suture, close the trapezius or latissimus in a separate layer, then the subcutaneous tissue and skin (staples or interrupted nylon).
- Obtain a post-operative chest radiograph to exclude pneumothorax; confirm the level and extent of decompression on anteroposterior and lateral films (CT if concern about residual compression or hardware). Post-operative care.
- Neurovascular assessment documenting lower-limb motor and sensory function; chest radiograph to exclude pneumothorax or haemothorax.
- Multimodal analgesia (avoid excessive opioids that depress respiration); incentive spirometry and chest physiotherapy to prevent atelectasis.
- Chest drain (if used) remains until output is less than 100 mL per 24 hours with no air leak; early mobilisation as tolerated.
- DVT prophylaxis with LMWH or mechanical devices; no weight-bearing restrictions unless stabilisation was performed; log-roll if posterior instrumentation placed; gradual return to activity over 4-6 weeks.
- Follow-up at 2 weeks (wound check, suture or staple removal), 6 weeks (clinical review, radiographs if instrumented), 3 months (CT or MRI if indicated) and 6-12 months (final review).
Procedures Through This Approach
- Spine tumour decompression and stabilisation - decompression, biopsy and combined posterior stabilisation for metastatic disease.
- Excision of thoracic disc herniation (soft or calcified) causing myelopathy or radiculopathy.
- Vertebral body biopsy for suspected tumour or infection.
- Debridement of pyogenic spondylodiscitis or tuberculous spondylitis with a paravertebral abscess.
- Drainage of paraspinal or epidural abscess when a posterior approach is insufficient.
- Limited anterolateral decompression for anterior cord compression (metastasis, burst fracture).
- Excision of rib head or costovertebral joint pathology.
Viva & Exam Focus
COSTOTRANSCOSTOTRANS - key steps
DANGERDANGER - structures at risk by layer
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old presents with progressive myelopathy and a large calcified thoracic disc herniation at T8-T9, posterolateral on MRI. How would you approach this?”
“A 68-year-old diabetic has T10-T11 discitis, vertebral osteomyelitis and a large left paravertebral abscess causing cord compression. How would you manage this?”
“A 62-year-old with known lung cancer has a T7 metastasis causing anterior cord compression and myelopathy, extending laterally into the rib head. How would you approach this?”
Position and incision
- Prone or lateral decubitus (affected side up)
- Paramedian or J-shaped incision 4-5 cm lateral to the midline
- Incision over the rib two levels above the target vertebra
- Confirm the level with fluoroscopy before the skin incision
- Divide the trapezius (upper) or latissimus (lower) in line with the incision
Internervous plane
- Intermuscular between the erector spinae (dorsal rami) and the intercostal muscles (ventral rami)
- Elevate the erector spinae subperiosteally from the ribs and transverse processes
- No motor nerves divided in the superficial dissection
- The exiting nerve root is the only neural structure that may be sacrificed
- The spinal cord lies medial and must never be retracted
Deep dissection steps
- Identify the intercostal neurovascular bundle in the subcostal groove before osteotomy
- Resect the transverse process at its base with a rongeur or osteotome
- Resect 4-6 cm of proximal rib including the costotransverse and costovertebral joints
- Maintain the extrapleural plane with blunt dissection and moist patties
- Work strictly lateral to the pedicle at all times
Danger structures by layer
- Superficial: dorsal rami cutaneous branches
- Rib: intercostal neurovascular bundle (ligate at the level of pathology only)
- Extrapleural: parietal pleura (repair small tears, chest drain if large)
- Deep: exiting nerve root (can sacrifice unilaterally)
- Medial: spinal cord (never retract - irreversible injury)
- Anterior: segmental radicular arteries (protect, especially left T9-T12)
Closure and post-op
- Repair pleural tears primarily or with a pleural flap
- Insert a 28 Fr chest drain if a large tear or a persistent air leak
- Layered closure: erector spinae, trapezius/latissimus, subcutaneous, skin
- Post-operative chest radiograph is mandatory
- Document lower-limb neurology immediately after surgery
Key exam points
- Costotransversectomy is extrapleural and posterolateral
- Distinct from transthoracic (transpleural) and lateral extracavitary (more lateral)
- The spinal cord is never retracted - work lateral to the pedicle
- The exiting root can be sacrificed; the cord cannot
- Pleural injury is the most common complication - chest drain if needed
- Confirm the level twice before rib resection
References
Guidelines, registries and global practice. Costotransversectomy is used worldwide for thoracic disc herniation, spinal tumour and infection when posterolateral extrapleural access is needed, and is a standard component of neurosurgical and orthopaedic spine fellowship training. AO Spine and the North American Spine Society emphasise that myelopathic thoracic disc herniations should be approached from the side of the pathology using an extrapleural route when possible, avoiding cord manipulation; NICE (UK) and the Spine Society of Australia recommend costotransversectomy or lateral extracavitary approaches for lateral and anterolateral thoracic disc disease, reserving transthoracic routes for midline calcified discs needing extensive anterior reconstruction. Thoracic disc herniation requiring surgery is rare (approximately 1 per 1,000,000 per year); surgical series consistently report neurological improvement in 80-95 percent of myelopathic patients when the cord is decompressed without manipulation, with pleural injury rates of 5-15 percent across large series, the majority managed with chest drainage. In high-resource centres intraoperative neuromonitoring (MEP/SSEP) is routine for myelopathic patients; in resource-limited settings the same anatomical principles apply and the approach is performed safely with meticulous technique. Chest-drain availability and post-operative chest radiography remain essential everywhere. Consent. Discuss pleural injury requiring a chest drain (5-15 percent), neurological deterioration (1-3 percent), wrong-level surgery (a never event), wound infection (2-5 percent), chronic radicular pain (10-20 percent), and the possibility of staged posterior stabilisation if anterior column reconstruction is required.
For the Operative Surgery station, describe the costotransversectomy systematically: prone positioning, paramedian incision, identification of the intercostal bundle, resection of the transverse process and proximal rib, maintenance of the extrapleural plane, protection of the spinal cord by staying lateral to the pedicle, and management of pleural injury. Know the differences from the transthoracic and lateral extracavitary approaches and the indications for each.
Surgical approach to single-level symptomatic thoracic disc herniations through costotransversectomy
- Case series of 10 patients undergoing costotransversectomy for symptomatic thoracic disc herniation
- All patients showed neurological improvement with no major complications reported
- Confirmed the approach provides safe posterolateral access for single-level pathology
Posterolateral approaches to the thoracic spine for calcific disc herniation
- Analysis of posterolateral approaches including costotransversectomy for calcified thoracic discs
- Wider exposure variants improve access but increase morbidity trade-offs
- Emphasises careful patient selection for extrapleural posterolateral routes
Additional lateral intermuscular access to standard costotransversectomy
- Describes a modification of costotransversectomy with additional lateral access for large median thoracic discs
- Improved surgical operability and exposure while maintaining extrapleural principles
- Demonstrates the evolution of the classic approach for challenging central herniations
Role of endoscopy in thoracic disc surgery and costotransversectomy
- Discusses ambulatory potential and endoscopic assistance in thoracic disc procedures including costotransversectomy
- Highlights reduced morbidity with minimally invasive adaptations of the posterolateral route
- Supports the safety profile for appropriately selected cases
Costotransversectomy for Thoracic Disc Herniation
- Classic series describing the posterolateral extrapleural approach for thoracic disc herniation with good neurological outcomes