Open direct-superior or arthroscopic resection | ACJ OA | Osteolysis | intermediate
- Resect exactly 5–10mm of distal clavicle — more than 10mm risks destabilising the posterior capsule and coracoclavicular ligaments, causing iatrogenic ACJ instability
- The posterior capsule and superior acromioclavicular ligaments must be preserved — they are the primary horizontal stabilisers of the ACJ, and their violation is the main cause of postoperative instability
- Distal clavicle osteolysis (weightlifter's shoulder) is a distinct entity from ACJ OA — repetitive microtrauma with subchondral insufficiency; responds well to DCE with 80–90% return to sport
- Arthroscopic Mumford offers outcomes comparable to open with no deltotrapezial takedown and faster recovery — comparative series report equivalent function; no high-quality RCT has shown either is superior
- Always confirm complete uniform resection — a superior-to-inferior wedge leaves an uneven shelf; resection must be uniform across the entire distal face of the clavicle
When & Why
Indication. Symptomatic acromioclavicular joint pain — localised superior shoulder pain, cross-body adduction pain and aching with overhead activity, with ACJ tenderness and radiographic change — that has failed conservative management. Four settings are treated by distal clavicle excision: - Primary or post-traumatic ACJ osteoarthritis — joint-space narrowing, subchondral sclerosis and osteophytes on radiograph.
- Distal clavicle osteolysis (weightlifter's shoulder) — a distinct entity: young male weightlifter or overhead athlete with subchondral resorption, cystic change and loss of cortical definition at the distal clavicle, without the eburnation of OA. MRI shows bone-marrow oedema in the distal clavicle.
- Post-traumatic ACJ arthritis developing years after a Rockwood type I–II ACJ sprain, treated identically to primary OA.
- ACJ symptoms found during subacromial decompression or rotator cuff repair, where arthroscopic DCE can be performed in the same sitting (selective, not routine). Conservative care first. Before surgery every patient must complete a minimum of three months of supervised physiotherapy (scapular stabilisation, activity modification), a trial of regular NSAIDs or analgesia, and at least one corticosteroid injection into the ACJ. A diagnostic injection that gives complete temporary relief confirms the ACJ as the pain source and predicts a good surgical outcome; no relief means reconsider the diagnosis. The one decision — open or arthroscopic. Every technique resects the same 5–10mm of distal clavicle. The choice is the approach:
Direct tactile feedback and precise resection measurement; simplest for isolated ACJ pathology and needs no special equipment. Requires elevating and repairing the deltotrapezial fascia. Return to work about 6–8 weeks.
Preserves the deltotrapezial fascia and posterior capsule, and addresses concurrent subacromial, cuff or glenohumeral pathology in the same sitting, with faster recovery — return to work 4–6 weeks.
Comparable outcomes in cohort and case series — no RCT proves either superior (be precise in the viva). Choose arthroscopic when concurrent pathology is present; open for isolated ACJ disease, revision or surgeon preference.
Consent specifically for ACJ instability (2–5%), persistent pain from inadequate resection (5–10%), deltoid weakness in the open approach (1–3%), supraclavicular nerve numbness in a cape distribution, and infection. Setup. Beach chair or semi-recumbent with the arm draped free (lateral decubitus is an alternative for the arthroscopic technique); an arthroscopic tower if the Mumford approach is chosen. Mark the clavicle, the acromion and the ACJ before incision.
The Operation
The goal is to remove 5–10mm of the distal clavicle to decompress the painful ACJ while leaving its stabilisers — the posterior capsule and superior AC ligaments horizontally, the coracoclavicular ligaments vertically — completely intact. The exposure, whether open direct-superior or arthroscopic indirect (subacromial, the Mumford procedure), is laid out in full as the first steps below. See also the acromioclavicular joint approach page.
Operative sequence
- Beach chair or semi-recumbent (lateral decubitus optional for arthroscopy), arm draped free.
- Mark the distal clavicle, the acromion and the ACJ before any incision — these landmarks define the joint and the resection line.
- A 3–4cm transverse or oblique incision centred directly over the ACJ.
- Identify and protect the supraclavicular nerve branches (C3–C4) that cross the field — injury causes numbness over the anterolateral chest in a cape distribution.
- Elevate the deltotrapezial fascia as a full-thickness flap — incise longitudinally over the clavicle, preserving a cuff of fascia on each side for later repair.
- Subperiosteal elevation exposes the distal clavicle superiorly and anteriorly. Do NOT strip the posterior capsule — this is the key horizontal stabilising structure.
- Standard posterior viewing portal plus an anterior working portal; a direct lateral or direct AC portal may be added.
- Perform a diagnostic glenohumeral arthroscopy first if indicated, then enter the subacromial space and bursectomise to visualise the ACJ capsule from below.
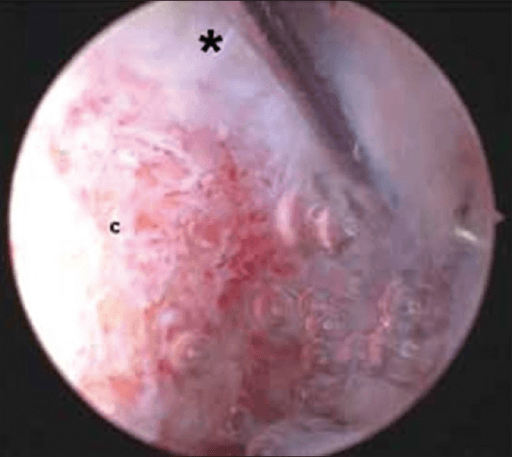
- Identify the inferior capsule of the ACJ and the inferior surface of the distal clavicle.
- The chief advantage of this route: the deltotrapezial fascia and posterior capsule are never violated, preserving every horizontal ACJ stabiliser.
- Plan 5–10mm from the lateral end, target 7–8mm. The AC capsule inserts about 3.5mm from the distal clavicle, so a combined 5–7mm of clearance preserves the capsular insertions (Stine and Vangsness, PMID 19732634).
- Open: mark the line with a ruler or calibrated osteotome. Arthroscopic: use a calibrated probe to set depth.
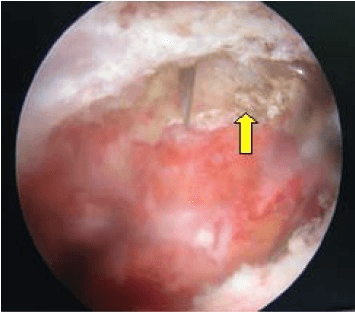
- Open — oscillating saw perpendicular to the long axis of the clavicle, beginning superiorly and completing inferiorly to maintain a perpendicular cut; remove the fragment and smooth sharp edges with a rongeur or burr.
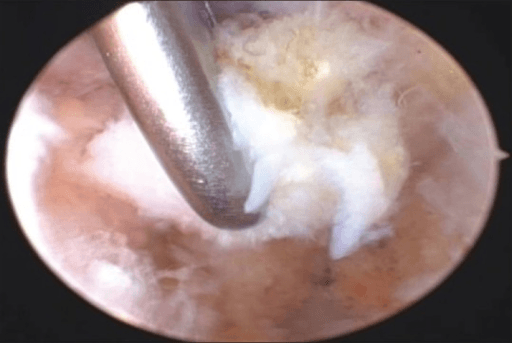
- Arthroscopic — 4.5mm shaver or burr resecting the inferior surface first, then progressing superiorly; switch to the direct AC portal for superior access and final confirmation.
- In both: aim for a uniform flat face perpendicular to the clavicle axis — no wedge, no superior or inferior shelf.
- Palpate the gap — a finger (open) or probe (arthroscopic) should move freely between the clavicle face and the acromion through full range of motion.
- Dynamic test: abduct and horizontally adduct the shoulder — no bony impingement should be felt or seen.
- Confirm a uniform 5–10mm gap and that the posterior capsule is intact.
- Open — repair the deltotrapezial fascia meticulously as a sleeve (critical to prevent deltoid weakness and cosmetic deformity); layered closure with a subcuticular skin closure.
- Arthroscopic — portal closure only; confirm haemostasis.
- Sling for comfort — this is not immobilisation; the arm may be used for light activities immediately.
Before any resection, plan to leave the posterior ACJ capsule and the superior acromioclavicular ligaments intact — they are the primary horizontal stabilisers. In the open approach dissect subperiosteally on the anterior and superior surfaces only and never strip posteriorly; keep the saw perpendicular to the clavicle axis, never angled posteriorly; and confirm the capsule is intact at the end. If it is violated the clavicle translates anteroposteriorly on the acromion — iatrogenic horizontal instability, the principal complication of this operation.
Resect 5–10mm, targeting 7–8mm. The AC capsule inserts about 3.5mm from the distal clavicle, so a combined 5–7mm of clearance preserves the capsular insertions (Stine and Vangsness, PMID 19732634). Less than 5mm leaves residual bony contact and persistent pain; more than 10mm destabilises the posterior capsule and begins to threaten the trapezoid.
The trapezoid begins a mean of 14.7mm and the conoid 32.1mm from the lateral end of the clavicle (Stine, PMID 19732634). A standard 5–10mm resection is safe; medial resection beyond about 15mm begins to detach the trapezoid and causes vertical instability — a second, distinct reason never to exceed 10mm.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Activity | |-------|--------|----------------|----------| | 1 | 0–2 weeks | Sling for comfort only (not immobilisation) | Pendulum exercises from day 1; wound review at 10–14 days | | 2 | 2–6 weeks | Discard sling when comfortable (~2 weeks) | Active-assisted and active ROM aiming for full elevation and cross-body adduction by 4–6 weeks; scapular stabilisation; no heavy lifting or overhead loading | | 3 | 6–12 weeks | — | Progressive resistance; non-upper-body gym from 6 weeks; upper-body loading from 8–10 weeks; bench and overhead press by 10–12 weeks | | Return to sport | 3–4 months | — | Weightlifters and overhead athletes back to competition at 3–4 months; manual labourers 6–8 weeks light, 3 months heavy; 80–90% of weightlifters return to pre-injury level | Expected outcomes | Outcome | Open DCE | Arthroscopic DCE | |---------|----------|------------------| | Good/excellent results | 90–95% | 90–95% | | Return to sport | 80–90% | 80–90% | | Pain relief (VAS reduction) | 60–70% | 60–70% | | Return to work | 6–8 weeks | 4–6 weeks | No adequately powered RCT has shown open and arthroscopic DCE to differ in functional outcome; the figures rest on cohort and case-series data (Zawadsky 2000, PMID 10976120; Kay 2003, PMID 14551540). Complications
- Rate
- 2–5%
- Recognition & mechanism
- Horizontal (AP) instability from posterior capsule and superior AC ligament violation — clicking, pain with cross-body adduction, visible clavicle prominence; confirmed on stress views
- Prevention & management
- Preserve the posterior capsule in the open approach; repair the deltotrapezial fascia. Mild: physiotherapy; symptomatic: revision stabilisation (e.g. Weaver-Dunn)
- Rate
- 5–10%
- Recognition & mechanism
- Most common cause of failure; less than 5mm removed with residual bony contact on cross-body adduction; X-ray shows the clavicle face too close to the acromion
- Prevention & management
- Mandatory intraoperative dynamic ROM check with a calibrated probe; revision DCE of an additional 2–3mm guided by fluoroscopy
- Rate
- 1–3% (open only)
- Recognition & mechanism
- Deltotrapezial fascia not repaired after the open approach; the deltoid origin lifts off the superior acromion/clavicle with weak forward flexion and abduction
- Prevention & management
- Repair the deltotrapezial fascia meticulously as a sleeve; early reattachment within 6 weeks if it dehisces
- Rate
- Less than 1%
- Recognition & mechanism
- Over-resection beyond 10mm enters trapezoid territory; superior clavicle translation (vertical instability), distinct from horizontal instability
- Prevention & management
- Never resect more than 10mm; mark the line before cutting; CC ligament repair or reconstruction if disrupted
- Rate
- 2–4%
- Recognition & mechanism
- Cutaneous branches crossing the incision; numbness and dysaesthesia over the anterolateral chest (cape distribution), usually neuropraxia resolving over 3–6 months
- Prevention & management
- Identify and protect branches before incision; blunt dissection near the nerve; observation; neuroma excision rarely needed
- Rate
- Less than 1%
- Recognition & mechanism
- Superficial or deep wound infection — erythema, pain, wound breakdown; higher risk if a corticosteroid injection was given within 3 months of surgery
- Prevention & management
- Standard antibiotic prophylaxis; avoid surgery within 3 months of injection; oral antibiotics for superficial, washout for deep
Viva & Exam Focus
MUMFORDMUMFORD — order of the operation
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old competitive powerlifter presents with 6 months of right ACJ pain worsening with bench press and overhead pressing. X-rays show subchondral resorption and cystic change at the distal clavicle without significant joint space narrowing or eburnation. What is your diagnosis and management?”
“What is the most important anatomical structure to preserve during distal clavicle excision, and what happens if it is violated?”
“Compare open and arthroscopic distal clavicle excision. When would you choose each technique, and what does the evidence show?”
Indications
- ACJ osteoarthritis — primary or post-traumatic, after failed 3 months of conservative care
- Distal clavicle osteolysis — weightlifter's shoulder with subchondral resorption
- A diagnostic ACJ injection giving temporary relief confirms the source
- ACJ symptoms during subacromial decompression or rotator cuff repair
- Post-traumatic ACJ arthritis years after a Rockwood type I–II sprain
Amount of resection
- 5–10mm is the gold standard (target 7–8mm)
- Less than 5mm — inadequate, persistent bony contact
- More than 10mm — risks the posterior capsule and trapezoid
- Confirm with a calibrated probe and dynamic intraoperative ROM
- Uniform flat cut perpendicular to the clavicle axis — no wedge
Critical anatomy
- Posterior capsule plus superior AC ligaments are the horizontal stabilisers — preserve
- CC ligaments are the vertical stabilisers — safe with standard DCE (trapezoid at about 15mm, conoid about 32mm)
- Repair the deltotrapezial fascia meticulously in the open approach
- Protect the supraclavicular nerves (C3–C4, cape distribution)
- The acromion is not resected — distal clavicle only
Open vs arthroscopic
- Comparable outcomes in cohort and case series — no RCT proves either superior
- Open: direct tactile feedback, no special equipment, requires deltotrapezial repair
- Arthroscopic: preserves fascia and posterior capsule, ideal with concurrent pathology
- Zawadsky 2000 (PMID 10976120): 38 of 41 good or excellent at 6.2 years
- Both achieve roughly 90% good or excellent results
Complications
- ACJ instability 2–5% — posterior-capsule violation causing horizontal instability
- Persistent pain 5–10% — most common failure, inadequate resection under 5mm
- Deltoid weakness 1–3% (open only) — deltotrapezial fascia not repaired
- CC ligament injury — only with over-resection beyond 10–15mm
- Supraclavicular nerve injury — numbness over the chest in cape distribution
Post-op milestones
- Sling for comfort only — early active ROM from day 1
- Full ROM by 4–6 weeks
- Return to non-upper-body gym at 6 weeks
- Bench and overhead press by 10–12 weeks
- Weightlifters — 80–90% return to pre-injury competitive level
Background & Evidence
Epidemiology. Acromioclavicular osteoarthritis is a common source of shoulder pain in older adults and frequently coexists with rotator-cuff disease and subacromial impingement; post-traumatic arthritis may follow even low-grade (Rockwood type I–II) ACJ sprains. Distal clavicle osteolysis (weightlifter's shoulder) is a separate entity seen in young male weightlifters and overhead athletes subjected to repetitive compressive loading. Pathoanatomy. The ACJ is a diarthrodial joint containing a fibrocartilaginous disc that degenerates with age. It is stabilised in two planes. Horizontally (anteroposterior translation) the posterior capsule and superior acromioclavicular ligament are the primary restraints; vertically (superior translation) the coracoclavicular ligaments — the posteromedial fan-shaped conoid resisting superior displacement and the anterolateral quadrilateral trapezoid resisting axial compression — are primary. The deltoid and trapezius share a common fascial origin (the deltotrapezial fascia) across the superior ACJ, which the open approach must elevate and repair. The supraclavicular nerves (C3–C4) cross the field and are at risk with a superior incision.
- ACJ osteoarthritis
- Older adult; often post-traumatic
- Distal clavicle osteolysis
- Young male weightlifter or overhead athlete
- ACJ osteoarthritis
- Degenerative cartilage wear
- Distal clavicle osteolysis
- Repetitive microtrauma exceeding subchondral remodelling
- ACJ osteoarthritis
- Joint-space narrowing, subchondral sclerosis, osteophytes (eburnation)
- Distal clavicle osteolysis
- Subchondral resorption, cystic change, loss of cortical definition — no eburnation
- ACJ osteoarthritis
- Cartilage loss, osteophytes
- Distal clavicle osteolysis
- Bone-marrow oedema in the distal clavicle, small joint effusion
- ACJ osteoarthritis
- DCE after failed conservative care
- Distal clavicle osteolysis
- DCE; 80–90% return to pre-injury sport
OSTEOLYSISOSTEOLYSIS — when to suspect distal clavicle osteolysis
Key evidence. The consistent message across the literature is that arthroscopic distal clavicle resection is safe and effective and gives results comparable to open excision. Gartsman (1993) established the arthroscopic technique; Zawadsky (2000) showed durable relief for osteolysis (38 of 41 good or excellent at 6.2 years); Kay (2003) showed combined DCE and subacromial decompression was 100% good or excellent at six years; and Stine and Vangsness (2009) provided the anatomic basis for the 5–10mm resection rule. No adequately powered randomised trial has shown either approach superior.
References
Historical and contextual references 1. Mumford EB. Acromioclavicular dislocation: a new operative treatment. J Bone Joint Surg. 1941;23:799-802. 2. Flatow EL, Duralde XA, Nicholson GP, et al. Arthroscopic resection of the distal clavicle with a superior approach. J Shoulder Elbow Surg. 1995;4(1):41-50. 3. Gartsman GM, Khan M, Hammerman SM. Arthroscopic repair of full-thickness tears of the rotator cuff. J Bone Joint Surg Am. 1998;80(6):832-840. PMID 9655101.
Arthroscopic resection of the acromioclavicular joint
Twenty-six patients with isolated ACJ osteoarthritis treated by arthroscopic distal clavicle resection; 20 reviewed at a minimum of two years with marked improvement in pain, activities of daily living, work and sport in 17, and no intraoperative complications. Three failures required subsequent open surgery. The landmark series establishing arthroscopic distal clavicle resection as safe and effective for isolated ACJ arthritis.
Osteolysis of the distal clavicle: long-term results of arthroscopic resection
Forty-one shoulders in 37 patients (mean age 39) with isolated distal clavicle osteolysis treated by arthroscopic direct-superior resection, mean follow-up 6.2 years: 22 excellent, 16 good, 3 failures (38 of 41 good or excellent). All three failures occurred in the post-traumatic subgroup; microtraumatic overuse osteolysis did slightly better. Confirms durable relief with low morbidity, with a traumatic aetiology carrying a slightly higher failure rate.
Long-term results of arthroscopic resection of the distal clavicle with concomitant subacromial decompression
Twenty patients with coexisting subacromial impingement and ACJ disease treated by combined arthroscopic distal clavicle excision and subacromial decompression, mean follow-up 6 years: 100% good or excellent, with mean UCLA score improving from 17.5 to 29.8 and Constant from 70.5 to 98.5. Asymptomatic calcific density distal to the resection seen in 25%. Impingement and ACJ disease frequently coexist and should be treated together in one sitting.
Analysis of the capsule and ligament insertions about the acromioclavicular joint: a cadaveric study
Twenty-eight cadaveric shoulders: the AC capsule inserts a mean 3.5mm from the distal clavicle and 2.8mm from the medial acromion; removing 2–3mm of medial acromion plus 3–4mm of distal clavicle (combined 5–7mm) preserves the capsular insertions, while resection greater than 15mm medially begins to detach the trapezoid. The trapezoid begins a mean 14.7mm and the conoid 32.1mm from the lateral clavicle. Provides the anatomic basis for the 5–10mm resection rule.