Superior Strap Incision | Deltotrapezial Fascia Repair Critical | CC Ligament Exposure
- A superior strap or saber incision over the distal clavicle and AC joint is the standard exposure.
- The supraclavicular nerves cross the clavicle 2 to 3 cm medial to the AC joint and must be protected or their sacrifice documented with informed consent.
- The deltotrapezial fascia must be incised in line with its fibers, elevated as a single layer, and meticulously repaired to restore the dynamic AC stabilizer.
- The coracoclavicular ligaments (conoid posterior and medial, trapezoid lateral and anterior) are exposed by dissecting medially along the clavicle to the coracoid base.
- The coracoid base is the key landmark for CC ligament reconstruction tunnels or grafts, and the lateral cord of the brachial plexus lies just medial to it.
When & Why
What it exposes. This approach gives direct access to the acromioclavicular (AC) joint, the distal clavicle and acromion, the coracoclavicular (CC) ligaments (conoid and trapezoid), and the coracoid base. It is the workhorse exposure for AC joint reconstruction (acute or chronic), distal clavicle excision (Mumford), CC ligament reconstruction or augmentation, and AC joint fixation. Incision variants. The superior strap incision is most common — centered over the AC joint and distal clavicle. An alternative saber incision runs obliquely from the posterior distal clavicle toward the coracoid and suits distal clavicle excision. An arthroscopic portal-based approach is reserved for selected low-grade or diagnostic cases. Position & landmarks. The patient is placed in the beach-chair or modified supine position with the head elevated 30 to 45 degrees. A small bump under the ipsilateral scapula protracts the shoulder and improves access to the AC joint and coracoid. The arm is draped free to allow intraoperative stress testing and reduction manoeuvres — avoid excessive traction, which stretches the brachial plexus. Intraoperative fluoroscopy (mini C-arm) is positioned for AP, axillary and Zanca views. The field extends from the sternoclavicular joint medially to the deltoid insertion laterally and includes the coracoid. A sterile tourniquet is rarely used. Palpable landmarks are the AC joint (a step-off or point of tenderness), the subcutaneous distal clavicle, the coracoid (approximately 2 cm inferior to the clavicle), the acromion, and — in thin patients — the supraclavicular nerve branches crossing the clavicle. Coracoclavicular ligament anatomy to plan around. The conoid ligament attaches to the conoid tubercle on the posterior clavicle approximately 4.5 cm medial to the AC joint (more posterior and medial); the trapezoid ligament attaches more laterally and anteriorly. Both share a common attachment at the coracoid base. Knowing these distinct footprints is essential for anatomic CC reconstruction.
The Exposure
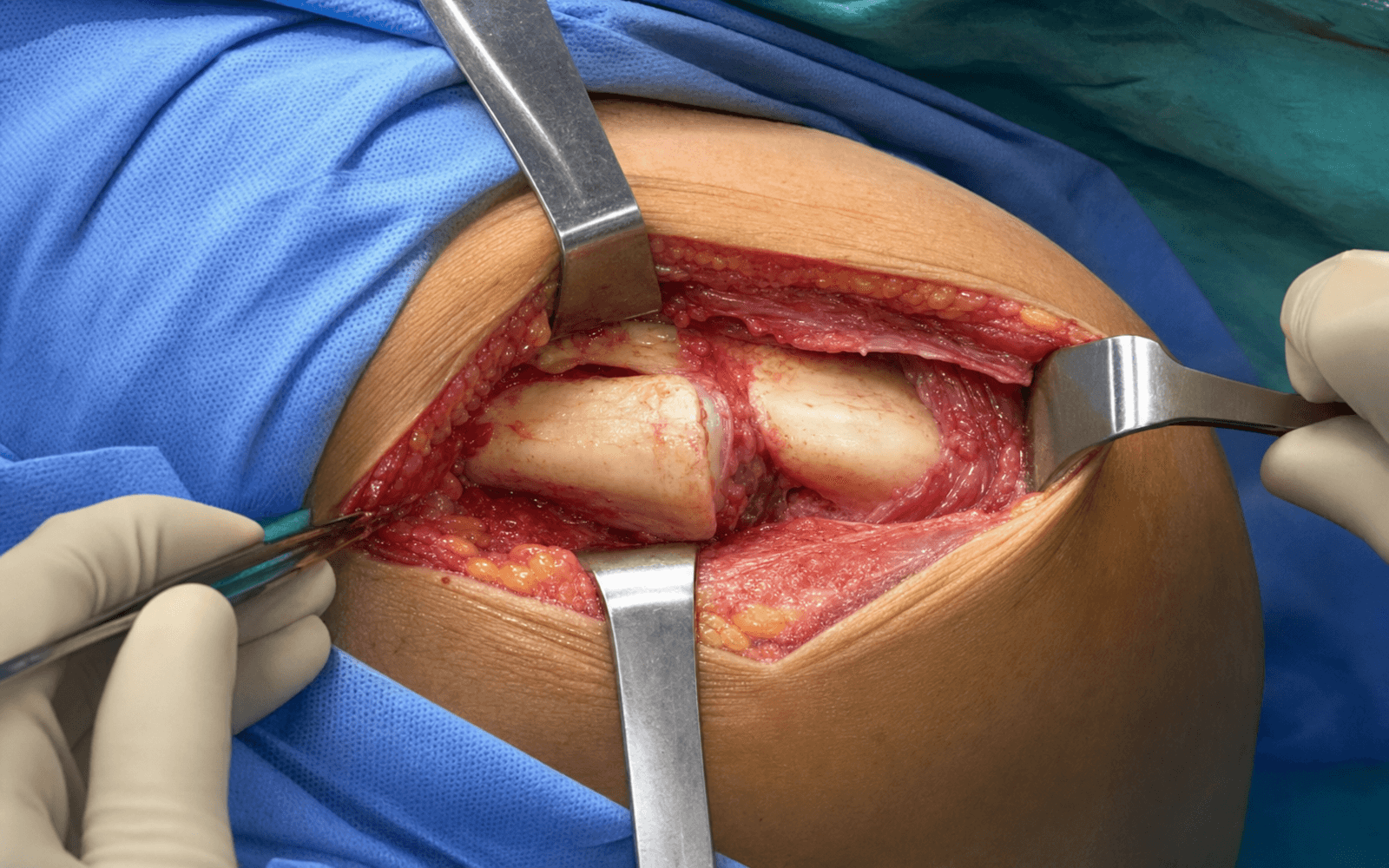
Work from the skin down through the deltotrapezial fascia, opening the AC capsule and then sweeping medially along the clavicle to expose the coracoclavicular ligaments and coracoid base.
Exposure sequence
- Centre a superior strap incision directly over the AC joint, extending 4 to 6 cm medially along the distal clavicle and 2 to 3 cm laterally over the acromion (or use a saber incision for distal clavicle excision).
- Mark it with the arm in slight abduction and forward flexion to relax skin tension, then carry it through skin and subcutaneous tissue.
- In the subcutaneous plane, identify the supraclavicular nerves (C3 to C4) crossing the clavicle 2 to 3 cm medial to the AC joint.
- Protect them with vessel loops where possible; if they must be sacrificed for exposure, document preoperative consent and bury the cut ends in muscle to reduce neuroma risk.
- There is no true internervous plane superficially — the deltotrapezial fascia is the confluence of deltoid (axillary nerve) and trapezius (spinal accessory nerve) fibres.
- Incise the fascia in line with the skin incision, splitting the fibres rather than transecting them, then elevate it as a single layer off the clavicle and acromion.
- Tag the fascial edges with stay sutures for later repair — this preserves the dynamic stabilising envelope.
- Open the AC joint capsule superiorly to expose the articular disc (if present) and the distal clavicular articular surface.
- Elevate the capsule as a sleeve medially and laterally so it can be repaired or reconstructed at closure; the superior capsule is the strongest component and the chief horizontal stabiliser.
- Working medially, elevate the fascia off the clavicle to expose the CC ligaments.
- Identify the conoid tubercle on the posterior clavicle and visualise the conoid (posterior and medial) and trapezoid (lateral and anterior) ligaments; protect them unless reconstruction is planned.
- Retract the deltoid anteriorly and pectoralis minor medially to expose the coracoid base — the landmark for CC reconstruction tunnels, anchors or grafts.
- Protect the lateral cord of the brachial plexus lying immediately medial to the coracoid, and the short head of biceps, coracobrachialis and pectoralis minor attachments on the coracoid.
The supraclavicular nerves (C3 to C4) cross the clavicle only 2 to 3 cm medial to the AC joint in the subcutaneous plane and supply sensation to the anterior shoulder skin. Injury causes numbness, dysesthesia and a recognised risk of painful neuroma. Identify them early under direct vision, protect them with vessel loops when possible, and — if sacrifice is needed for exposure — confirm documented preoperative counselling and bury the cut ends in muscle.
The deltotrapezial fascia is the primary dynamic stabiliser of the AC joint once the capsule and CC ligaments are disrupted or reconstructed. Split it in line with its fibres, elevate it as one tagged sleeve, and close it meticulously with strong interrupted sutures (reinforced with suture anchors if tissue quality is poor). Poor fascial repair causes scapular dyskinesis and persistent instability even with perfect ligament reconstruction.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Supraclavicular nerves (C3 to C4, 2 to 3 cm medial to AC joint)
- Protection
- Identify early; vessel-loop when possible; document consent for sacrifice; bury cut ends
- Structure at risk
- Deltotrapezial fascia (primary dynamic stabiliser)
- Protection
- Split in line with fibres; elevate as a single tagged sleeve; meticulous strong-suture repair
- Structure at risk
- AC joint capsule (horizontal stability; superior capsule strongest)
- Protection
- Open superiorly; preserve as a sleeve; repair or reconstruct
- Structure at risk
- Conoid and trapezoid ligaments (conoid posterior and medial, 4.5 cm from AC joint)
- Protection
- Visualise and protect unless reconstructing; know the distinct footprints
- Structure at risk
- Lateral cord of brachial plexus (medial to coracoid); musculocutaneous nerve (enters coracobrachialis 5 to 8 cm distal to coracoid tip); axillary nerve (inferior extension)
- Protection
- Blunt Hohmann on the coracoid base; drill sleeve and direct vision; limit inferior dissection
- Structure at risk
- Cephalic vein (deltopectoral interval if extended laterally)
- Protection
- Avoid aggressive lateral extension into the deltopectoral interval
Extensile options. Extend medially along the clavicle for more proximal clavicle exposure or further CC ligament work. Extend laterally over the acromion or into the deltopectoral interval for combined procedures such as rotator cuff repair or shoulder arthroplasty. Inferior extension toward the coracoid is limited and demands protection of the lateral cord and musculocutaneous nerve. Closure. Layered closure is essential. Repair the AC capsule with absorbable suture. Close the deltotrapezial fascia with strong interrupted sutures — reinforced with suture anchors if tissue quality is poor. Approximate subcutaneous tissue and close skin; apply a sling postoperatively.
Procedures Through This Approach
- AC joint reconstruction (acute or chronic) — CC ligament reconstruction with autograft, allograft or synthetic device, plus AC capsule repair.
- Distal clavicle excision (Mumford) — resection of 8 to 10 mm of distal clavicle with smoothing of the cut surface.
- AC joint fixation (hook plate) — plate applied with reduction maintained; removal planned at 3 to 6 months to prevent acromial erosion.
- CC ligament reconstruction or augmentation, and exposure of the scaphotrapezial-type pantrapezial work is done through other approaches; this exposure is dedicated to the AC/CC complex.
Viva & Exam Focus
ACJOINTAC JOINT APPROACH — surgical steps
DANGERDANGER STRUCTURES BY LAYER
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“During an AC joint reconstruction, why is meticulous repair of the deltotrapezial fascia considered the most critical step for postoperative stability?”
“A patient is undergoing open AC joint reconstruction. How do you manage the supraclavicular nerves during the approach and what preoperative discussion is required?”
“During exposure of the coracoid base for CC ligament reconstruction, what neurovascular structures are at risk and how do you protect them?”
Position and setup
- Beach-chair with 30 to 45 degree head elevation
- Bump under scapula to protract shoulder
- Arm draped free for intraoperative stress testing
- Fluoroscopy for AP, axillary and Zanca views
- Field from SC joint to deltoid insertion
Incision and superficial dissection
- Superior strap or saber incision over AC joint and distal clavicle
- Identify and protect or document supraclavicular nerves
- Incise deltotrapezial fascia in line with skin incision
- Elevate fascia as a single layer from clavicle and acromion
- Tag fascia edges with stay sutures for repair
Deep dissection
- No true internervous plane — split deltotrapezial fascia fibres
- Open AC capsule superiorly to expose articular surfaces
- Elevate capsule medially and laterally as a sleeve
- Dissect medially along clavicle to expose CC ligaments
- Expose coracoid base as the CC reconstruction landmark
Danger structures
- Supraclavicular nerves (C3 to C4) in the subcutaneous layer
- Deltotrapezial fascia — repair is critical for outcome
- AC capsule for horizontal stability
- Lateral cord of brachial plexus medial to coracoid
- Musculocutaneous nerve 5 to 8 cm distal to coracoid tip
Closure and key principles
- Repair AC capsule with absorbable suture
- Meticulous deltotrapezial fascia closure with strong sutures
- Consider suture anchors if tissue quality is poor
- Document supraclavicular nerve management
- Sling immobilization postoperatively
Procedures and extensions
- AC joint reconstruction (acute or chronic)
- Distal clavicle excision (Mumford) — resect 8 to 10 mm
- AC joint fixation (hook plate) — remove at 3 to 6 months
- Medial extension along the clavicle
- Limited inferior extension to coracoid with nerve protection
References
Surgical Treatment of Complete Acromioclavicular Dislocations
- Described the classic Weaver-Dunn procedure using the coracoacromial ligament for CC reconstruction
- Highlighted the importance of deltotrapezial fascia repair for dynamic stability
- Reported good results in 15 patients with chronic AC separations
Anatomic Coracoclavicular Ligament Reconstruction
- Defined the anatomic footprints of the conoid and trapezoid ligaments on the clavicle and coracoid
- Demonstrated that anatomic double-bundle reconstruction restores native AC joint kinematics
- Emphasized the role of the AC capsule in horizontal stability
Supraclavicular Nerve Injury in Clavicle Surgery
- Anatomic study showing supraclavicular nerves cross the clavicle 2.5-3.5 cm medial to the AC joint in 80 percent of specimens
- Recommended preoperative counseling about anterior shoulder numbness
- Suggested nerve preservation when possible and burying cut ends to reduce neuroma risk
Deltotrapezial Fascia Repair in AC Joint Reconstruction
- Early recognition that failure to repair the deltotrapezial fascia leads to poor outcomes despite ligament reconstruction
- Described the fascia as the key dynamic stabilizer of the AC joint
- Recommended strong suture repair and consideration of reinforcement techniques
Coracoid Drilling Safety in Shoulder Surgery
- Defined safe zones for coracoid drilling and the proximity of the lateral cord and musculocutaneous nerve
- Recommended use of drill sleeves and direct visualization to avoid neurovascular injury
- Reported the distance from coracoid tip to musculocutaneous nerve entry as 5-8 cm