Longitudinal incision | Extensor protection | Subperiosteal dorsal cortex exposure
- There is no true internervous plane. All the extensor tendons are radial-nerve supplied (posterior interosseous nerve) from the proximal forearm, so the dorsal hand itself carries no crossing motor nerve — the approach is an intertendinous or sub-tendinous interval, and muscle denervation is not a concern.
- The structures at risk are sensory. The superficial radial nerve (thumb, index, middle, radial ring) and the dorsal cutaneous branch of the ulnar nerve (ulnar ring, little) lie in the subcutaneous plane and cross the field — identify and protect them with vessel loops before any retraction.
- Mobilize the extensor tendon rather than divide it. At the metacarpal neck the sagittal bands centralize the tendon over the metacarpal head and must be repaired if incised, to prevent postoperative extensor subluxation into the intermetacarpal valley with loss of active MCP extension.
- Divide the juncturae tendinum only when they block exposure, and elevate the dorsal cortex subperiosteally, limiting stripping to the plate footprint to preserve fragment vascularity.
- Position supine on a radiolucent hand table with an upper-arm tourniquet at 250 mmHg, elbow flexed 90 degrees and forearm pronated. Loupes and a headlight are essential for the fine subcutaneous nerve dissection.
When & Why
What it exposes. The dorsal approach gives direct access to the dorsal cortex of the metacarpal and phalangeal shafts and the dorsal half of the MCP, PIP and DIP joints. It is the workhorse exposure for the majority of metacarpal and proximal/middle phalanx fractures requiring open reduction and internal fixation, for malunion correction, and for MCP joint procedures. Why dorsal. The dorsal surface of the metacarpals and phalanges is relatively flat and subcutaneous, giving the most direct route to the shafts. Plates applied dorsally are biomechanically favourable because they resist the bending forces that act on the hand. The approach also avoids the critical neurovascular structures on the volar side (the common digital arteries and nerves), making it safer than a volar route for the vast majority of shaft and dorsal articular pathology. A volar or Bruner approach is reserved for flexor-tendon and digital-neurovascular problems. Indications - Displaced metacarpal shaft, neck or base fractures requiring ORIF
- Displaced proximal or middle phalanx fractures
- Intra-articular fractures of the MCP, PIP or DIP joints with greater than 2 mm step-off
- Metacarpal or phalangeal malunion requiring corrective osteotomy
- MCP joint arthroplasty or synovectomy
- Extensor tendon repair or reconstruction requiring dorsal exposure
- Metacarpal or phalangeal nonunion Contraindications - Active infection over the planned incision
- Severe dorsal soft-tissue loss or burn requiring alternative coverage
- When volar pathology (flexor tendon, digital nerve) is the primary target — use a volar or Bruner approach
- Isolated volar plate avulsion injuries, which are better accessed volarly Alternative approaches - Volar approach (Bruner or midlateral): for flexor-tendon or digital-neurovascular pathology
- Lateral approach: for collateral-ligament or condylar fractures
- Combined dorsal-volar: for complex intra-articular fractures with both dorsal and volar fragments
- Incision
- Straight longitudinal centered over the shaft
- Best for
- Isolated fracture
- Incision
- Longitudinal in the valley between rays, or two separate incisions
- Best for
- Multiple fractures
- Incision
- Gently curved over the MCP joint, convex ulnar or radial
- Best for
- Joint access or deformity surgery
Position & landmarks. Supine on the operating table with the arm abducted onto a radiolucent hand table, an upper-arm tourniquet at 250 mmHg, the elbow flexed 90 degrees and the forearm pronated. The surgeon sits at the end of the hand table. Palpable landmarks are the metacarpal heads (the knuckles when a fist is made), the metacarpal bases at the carpometacarpal junction (especially the 2nd and 5th), the MCP joint line (about 1 cm proximal to the metacarpal head prominence), and the PIP and DIP joints. Plan the incision before skin prep to avoid distortion. Mark a 4-8 cm longitudinal or gently curved line centered over the fracture or joint to be exposed.
Upper-arm tourniquet at 250 mmHg, maximum 2 hours for adults. Document the inflation time and release the tourniquet before closure to identify and control bleeding points. Prolonged tourniquet time increases postoperative pain and stiffness.
The Exposure
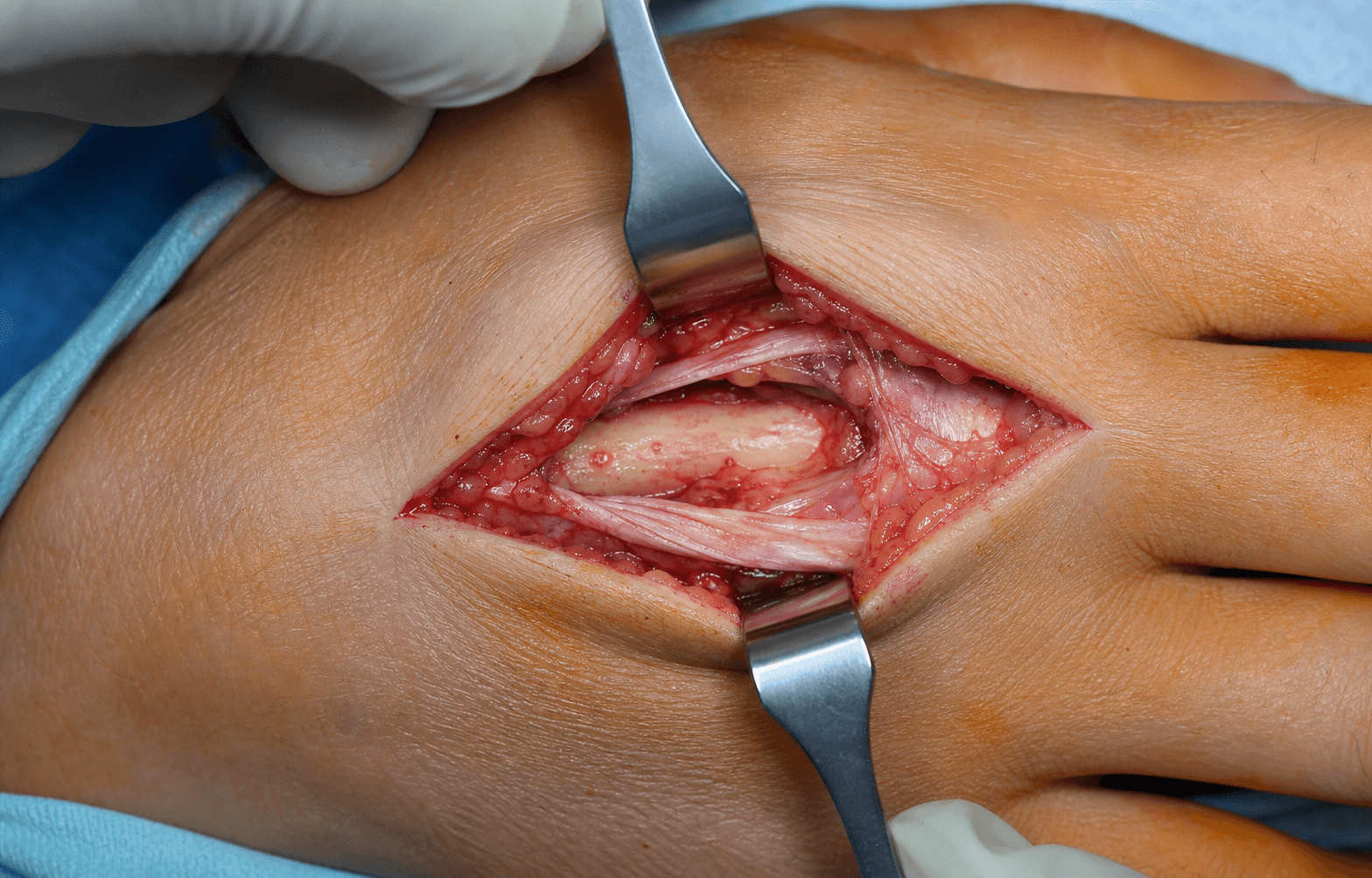
Work down through the dorsal layers, protecting the dorsal veins and the sensory nerve branches first, then mobilize the extensor mechanism to reach the dorsal cortex. The exposure is an intertendinous or sub-tendinous interval, not an internervous plane — all the extensor tendons have already been supplied by the radial nerve (posterior interosseous) in the proximal forearm, so no motor nerve crosses the dorsal hand itself. The real danger throughout is the subcutaneous sensory nerve branches and the extensor mechanism. The layers you traverse (superficial to deep) 1. Skin and subcutaneous fat 2. Dorsal venous network and sensory nerve branches (superficial radial nerve and dorsal cutaneous branch of the ulnar nerve) 3. Extensor tendons enveloped by loose areolar tissue 4. Sagittal bands at the MCP level (centralize the extensor tendon) 5. Juncturae tendinum (interconnect adjacent EDC tendons) 6. Periosteum and dorsal cortex of the metacarpal or phalanx 7. Joint capsule (MCP, PIP, DIP) The extensor mechanism. The extensor digitorum communis (EDC) sends a central tendon to each finger, with the extensor indicis proprius (EIP) and extensor digiti minimi (EDM) providing independent extensors to the index and little fingers. The sagittal bands are transverse fibres at the MCP joint that keep the extensor tendon centralized over the metacarpal head. The juncturae tendinum are oblique interconnecting bands between adjacent EDC tendons proximal to the MCP joints. Distally, the lateral bands (from the interossei and lumbricals) converge to form the terminal extensor tendon at the DIP joint. Neurovascular. The superficial radial nerve supplies the dorsum of the thumb, index, middle and radial ring fingers, while the dorsal cutaneous branch of the ulnar nerve supplies the ulnar ring and little fingers. Both lie in the subcutaneous plane and cross the operative field.
Exposure sequence
- Make a straight or gently curved longitudinal incision through skin only, centered over the metacarpal shaft or in the intermetacarpal valley, typically 4-8 cm for the shaft and shorter or longer as required for phalangeal work.
- Avoid cutting directly through visible large dorsal veins; plan the line to skirt them.
- Gently spread the subcutaneous fat with scissors and preserve the large dorsal veins, ligating only small branches.
- Identify the sensory nerve branches that cross the field — superficial radial nerve for the radial digits, dorsal cutaneous ulnar nerve for the ulnar digits — and place a vessel loop around each for gentle retraction and protection throughout the case.
- Incise the loose areolar fascia over the extensor tendon in the line of the incision.
- Do not divide the extensor tendon itself — it is covered by a thin gliding layer of loose tissue that you sweep aside.
- At the metacarpal level the extensor tendon lies directly over the dorsal cortex. Develop the plane between the tendon and the periosteum with a periosteal elevator or blunt dissection.
- Retract the tendon radially or ulnarly with skin hooks or a small retractor (avoid crushing self-retaining retractors on the tendon) and keep it moist with saline throughout.
- If exposure of the metacarpal neck or MCP joint is required, the sagittal band may be split longitudinally in the midline, or on the side opposite the fracture.
- The sagittal band centralizes the extensor tendon over the metacarpal head — if it is divided it must be repaired at closure with 3-0 or 4-0 non-absorbable suture.
- The juncturae tendinum are oblique interconnecting bands between adjacent EDC tendons. Divide them only when they prevent full retraction of the extensor tendon.
- When a junctura is substantial, attempt repair at closure to maintain extensor balance between adjacent fingers.
- With the extensor tendon retracted, incise the periosteum longitudinally over the dorsal cortex and elevate it medially and laterally with a periosteal elevator.
- Limit stripping to what is required for the plate footprint, to preserve fragment vascularity.
- For intra-articular MCP, PIP or DIP fractures, incise the joint capsule carefully to visualize the dorsal articular surface.
- At the PIP joint protect the central slip insertion on the middle phalanx base; at the DIP joint protect the terminal extensor tendon. Repair any divided structure at closure.
The superficial radial nerve and dorsal cutaneous ulnar nerve branches lie in the subcutaneous plane only millimetres deep and cross the operative field. Injury causes a painful neuroma or dorsal numbness in 3 to 8 percent of cases. Identify each branch early, loop it, retract it gently with vessel loops (never self-retaining retractors on a nerve), and release retraction periodically. If a branch is transected intra-operatively, perform a primary microsurgical repair with 9-0 nylon under the microscope.
Because the radial nerve (posterior interosseous) has supplied all the extensor tendons proximally in the forearm, the dorsal hand carries no crossing motor nerve. The approach is therefore an intertendinous or sub-tendinous interval, and muscle denervation is not the concern. The structures that matter are the subcutaneous sensory branches of the radial and ulnar nerves and the sagittal-band stabilization of the extensor tendon at the MCP joint.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Dorsal veins
- Protection
- Preserve large channels, ligate only small branches
- Structure at risk
- Superficial radial nerve (radial digits) and dorsal cutaneous ulnar nerve (ulnar digits)
- Protection
- Identify early, vessel loop, gentle retraction, no self-retainers on the nerve
- Structure at risk
- Extensor tendon proper
- Protection
- Mobilize with skin hooks, keep moist, do not crush or divide
- Structure at risk
- Sagittal bands
- Protection
- Split longitudinally only if needed, repair with non-absorbable suture at closure
- Structure at risk
- Juncturae tendinum
- Protection
- Divide only if blocking exposure, repair if substantial
- Structure at risk
- Periosteum and dorsal cortex, joint capsule
- Protection
- Elevate subperiosteally with limited stripping, protect central slip and terminal tendon
Extensile options. The incision extends proximally along the radial or ulnar border to the carpometacarpal joints or distal radius (the same nerve and vein protection applies; for thumb metacarpal base fractures place the incision more radially and extend into the anatomic snuffbox if the scaphoid or trapezium must be reached). It extends distally over the proximal or middle phalanx — at the PIP joint the central slip insertion must be protected and repaired if divided, and at the DIP joint the terminal extensor tendon is likewise protected. For complex intra-articular fractures with volar and dorsal fragments a combined dorsal and volar (Bruner) approach may be required, staged or simultaneous depending on the soft tissues. For selected fractures, percutaneous or limited-open mini-incision techniques are acceptable, but the principles of nerve and extensor protection remain identical. Closure. Copious irrigation, release the tourniquet and achieve haemostasis. Repair any divided sagittal bands with non-absorbable suture, approximate the subcutaneous tissue loosely, and close the skin with interrupted non-absorbable suture or an absorbable subcuticular suture. Apply a light compressive dressing with a plaster slab in the intrinsic-plus position. Complications
- Incidence
- 10-20%
- Prevention
- Early ROM, extensor gliding exercises
- Management
- Tenolysis if no improvement at 6 months
- Incidence
- 2-5%
- Prevention
- Sagittal band repair whenever divided
- Management
- Revision repair or sagittal band reconstruction
- Incidence
- 3-8%
- Prevention
- Careful nerve handling, vessel loops
- Management
- Desensitization, steroid injection, excision and burial into muscle
- Incidence
- 1-3%
- Prevention
- Prophylactic antibiotics, sterile technique
- Management
- Irrigation and debridement, antibiotics
- Incidence
- 5-10%
- Prevention
- Intra-operative rotational cascade check
- Management
- Corrective osteotomy
- Incidence
- Less than 5%
- Prevention
- Stable fixation, bone graft if needed
- Management
- Revision ORIF with bone graft
Mobilization protocol. Days 0-3: elevation, finger pumps and active ROM of uninvolved joints. Days 3-14: early active and passive ROM of the MCP, PIP and DIP as fixation stability allows (usually within 48-72 hours for stable fixation). Weeks 2-6: progressive strengthening and tendon-gliding, with sutures removed at 10-14 days and a protective splint for 4-6 weeks. Weeks 6-12: full active use and return to light work; full unrestricted activity by about 3 months. DVT prophylaxis is not routinely required for isolated hand surgery unless the patient carries additional risk factors.
Extensor tendon subluxation into the intermetacarpal valley after an unrepaired sagittal-band injury presents with loss of active MCP extension and a snapping sensation. Prevention is simple — repair the sagittal band with non-absorbable suture at the index procedure whenever it has been divided. Established subluxation needs revision repair or sagittal-band reconstruction.
Procedures Through This Approach
- Finger fracture fixation — the principal operation done through this exposure: ORIF of metacarpal shaft, neck and base fractures and of proximal and middle phalanx fractures.
- Intra-articular fracture fixation of the MCP, PIP and DIP joints (aiming for less than 2 mm articular step-off).
- Corrective osteotomy for metacarpal or phalangeal malunion.
- MCP joint arthroplasty or synovectomy, and extensor-tendon repair or reconstruction requiring dorsal exposure.
- Revision ORIF with bone graft for metacarpal or phalangeal nonunion.
Viva & Exam Focus
DORSALDORSAL HAND — the surgical steps
DANGERDANGER STRUCTURES — layer by layer
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old right-hand-dominant carpenter sustains a displaced spiral fracture of the right ring finger metacarpal shaft after a fall, with clinically evident rotational malalignment. Describe your surgical approach and key technical points.”
“A 35-year-old pianist presents with a displaced intra-articular fracture of the index MCP joint after a fall onto the knuckle. CT shows a volar fragment with greater than 3 mm step-off and 30 percent articular surface involvement. Describe your approach and fixation strategy.”
“A 22-year-old motorcyclist sustains displaced fractures of the 2nd, 3rd and 4th metacarpal shafts. Describe your surgical planning and approach selection for multiple rays.”
Position & setup
- Supine, arm on a radiolucent hand table
- Upper-arm tourniquet at 250 mmHg
- Elbow 90 degrees flexion, forearm pronated
- Chinese finger traps available for traction
- Headlight and loupes essential
Incision & superficial
- Longitudinal or gently curved dorsal incision
- Identify and protect the dorsal veins first
- Identify SRN (radial digits) and SUN (ulnar digits) branches
- Vessel-loop the nerves for gentle retraction
- Incise the loose fascia over the extensor tendon
Extensor mechanism
- Mobilize the extensor tendon with skin hooks
- Do not divide the extensor tendon if avoidable
- Split the sagittal band longitudinally if MCP exposure is needed
- Repair the sagittal band with non-absorbable suture at closure
- Divide the juncturae tendinum only if blocking exposure
Deep exposure
- Develop the plane between the extensor tendon and the periosteum
- Subperiosteal elevation of the dorsal cortex
- Limit stripping to the plate footprint
- Protect the joint capsule if intra-articular work is required
- Keep the tendon moist with saline throughout
Danger structures
- Dorsal veins — preserve the large channels
- SRN and SUN sensory branches — vessel loop early
- Extensor tendon — mobilize, do not crush or divide
- Sagittal bands at MCP — repair if incised
- Juncturae tendinum — repair if substantial
Closure & aftercare
- Repair the sagittal band if divided
- Loose subcutaneous closure
- Skin with interrupted or subcuticular suture
- Intrinsic-plus splint initially
- Early active ROM within 48-72 hours if fixation is stable
References
Complications and range of motion following plate fixation of metacarpal and phalangeal fractures
- Extensor tendon adhesions and stiffness occur frequently after dorsal plating
- Early motion protocols reduce adhesion rates and improve outcomes
- Painful neuromas from SRN injury are a preventable cause of poor outcome
Internal fixation of oblique metacarpal fractures. A biomechanical evaluation by impact loading
- Dorsal plating provides superior bending stiffness compared with crossed K-wires or intramedullary fixation
- Plate fixation allows earlier mobilization with lower rates of malunion
- Rotational control is critical and is best achieved with plate fixation
Functional anatomy of the thumb sagittal band
- Sagittal band disruption leads to extensor tendon subluxation and loss of active MCP extension
- The sagittal band is critical for maintaining extensor tendon centralization over the metacarpal head
- Repair of the sagittal band is essential when it is divided during dorsal exposure
Prognostic factors for non-surgically treated sagittal band injuries of the metacarpophalangeal joint
- Sagittal band injuries at the MCP joint have variable healing potential depending on severity
- Acute injuries with tendon subluxation benefit from surgical repair of the sagittal band
- Chronic injuries may require reconstruction with tendon graft or local tissue flaps