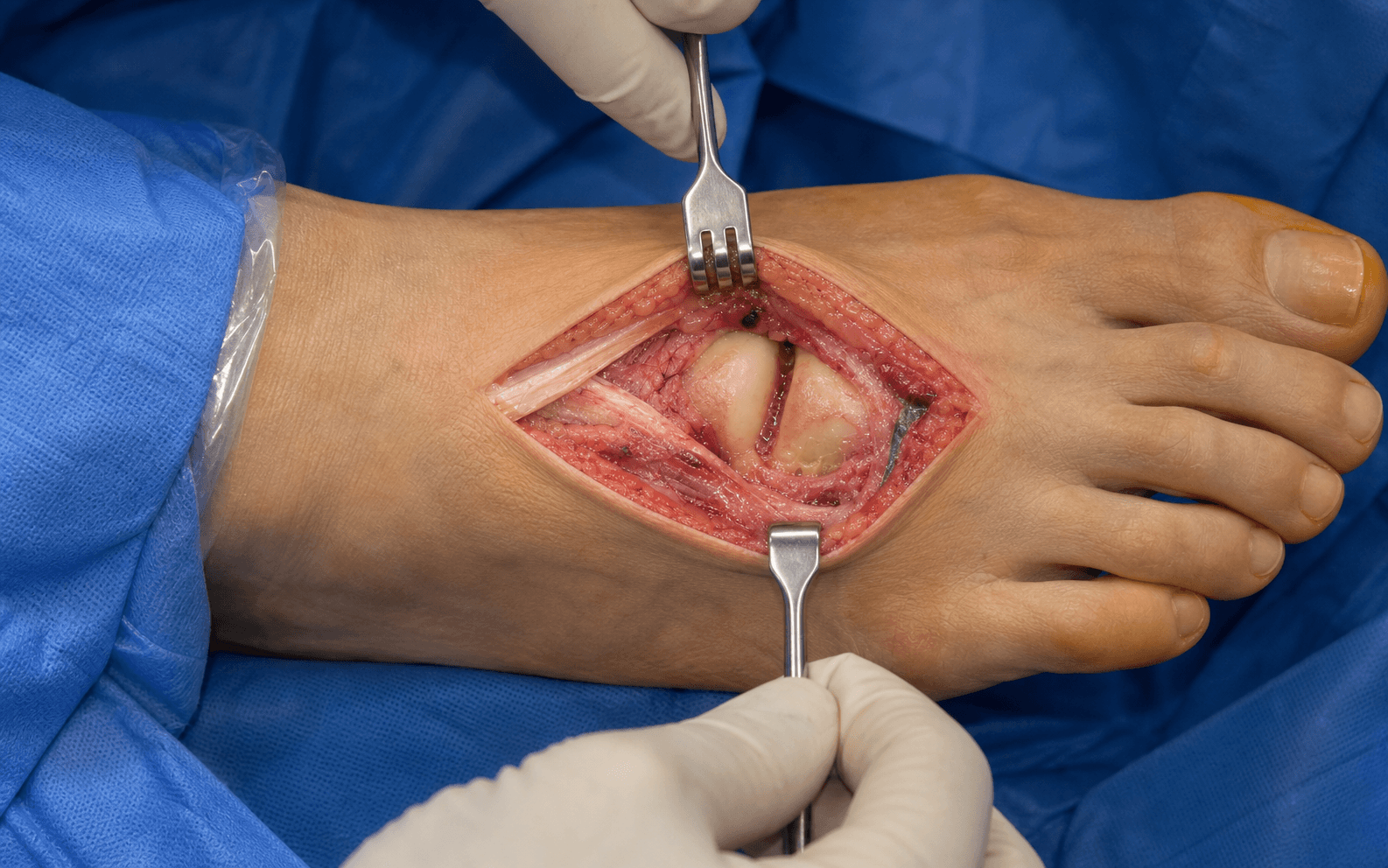
Dorsomedial incision | Dorsomedial cutaneous nerve protection | Capsular plication
- The dorsomedial cutaneous nerve to the hallux lies immediately dorsal or within the field and must be protected meticulously to avoid a painful neuroma.
- The incision is kept just dorsal to the abductor hallucis tendon, which defines the medial boundary and keeps the plantar medial nerve branches safe.
- There is no true internervous plane — this is a subcutaneous, extra-compartmental approach whose safety depends on early nerve identification, not a muscle interval.
- A longitudinal or Y-shaped capsulotomy gives full exposure of the metatarsal head and sesamoid complex.
- Capsular plication on closure is essential to restore medial stability after bunionectomy and to prevent recurrence.
When & Why
What it exposes. The dorsomedial approach gives direct, extensile access to the first metatarsophalangeal (MTP) joint — the medial eminence, the metatarsal head articular surface, the base of the proximal phalanx and the sesamoid complex — through a single incision that can be extended proximally or distally. It is the workhorse exposure for the majority of hallux valgus corrective procedures, cheilectomy and first MTPJ arthrodesis. Why dorsomedial. The approach avoids the weight-bearing plantar skin and the plantar medial neurovascular bundle while giving excellent visualization for corrective osteotomies and joint-preserving or fusion procedures. It is familiar to all foot and ankle surgeons and has a low complication rate when the dorsomedial cutaneous nerve is protected. Primary indications. - Hallux valgus corrective surgery — distal soft tissue procedure (modified McBride), chevron (Austin), scarf, proximal metatarsal or Akin osteotomy, and medial eminence resection with capsular plication
- Cheilectomy for hallux rigidus (dorsal osteophyte resection and joint debridement)
- First MTPJ arthrodesis for severe hallux rigidus, inflammatory arthritis or failed previous surgery
- Synovectomy and debridement in inflammatory arthropathies (rheumatoid, gout)
- Removal of loose bodies, osteochondral lesions or dorsal exostoses, and biopsy or curettage of benign bone lesions of the metatarsal head Contraindications. Active infection or ulceration over the proposed incision; severe peripheral vascular disease with inadequate skin perfusion; previous surgery with extensive scarring requiring a different approach; isolated plantar pathology better addressed plantarly; and the need for extensive lateral release that may demand a separate lateral incision. Alternative approaches. A pure medial approach (isolated medial eminence resection in very mild cases, limited exposure); a plantar medial approach (sesamoid pathology or extensive plantar release); a lateral approach (rarely used alone, combined for complete lateral release in severe hallux valgus); and minimally invasive percutaneous techniques for chevron or Akin osteotomies in selected patients (a different skill set). Position & landmarks. The patient is supine with a sandbag under the ipsilateral hip to internally rotate the leg and bring the medial forefoot into view, the knee slightly flexed over a bolster, the ankle in neutral or slight plantarflexion, and the foot at the end of the table. A thigh or ankle tourniquet is applied; the foot is prepped and draped free. Palpable bony landmarks are the first metatarsal head, the MTP joint line (felt by moving the hallux), the medial eminence, the proximal phalanx base and the metatarsal shaft. Key soft-tissue landmarks are the dorsomedial cutaneous nerve (often visible or palpable as a thin cord crossing dorsomedially), the extensor hallucis longus (EHL) tendon laterally and the abductor hallucis tendon plantar-medially. The incision is a longitudinal or gently curved line centered over the joint, 3 to 5 cm long, placed just dorsal to the abductor hallucis tendon (about 5 to 10 mm dorsal to the most medial prominence).
An ankle tourniquet is often preferred for forefoot surgery to shorten tourniquet time and allow earlier release for haemostasis assessment; a thigh tourniquet gives a bloodless field but may cause more postoperative thigh discomfort. Document tourniquet time and pressure in every case.
The Exposure
Work down through the layers along the dorsomedial aspect of the hallux, protecting the dorsomedial cutaneous nerve at every step, retracting (never dividing) the EHL and abductor hallucis, and entering the joint with a longitudinal or Y-shaped capsulotomy.
Exposure sequence
- A longitudinal or gently curved incision on the dorsomedial aspect of the hallux, centered over the first MTP joint line.
- Begins about 1 cm proximal to the joint line and extends 2 to 3 cm distal, giving a total length of 3 to 5 cm.
- Placed just dorsal to the abductor hallucis tendon, avoiding the weight-bearing plantar skin and the plantar medial neurovascular bundle.
- Extendable proximally along the metatarsal shaft for osteotomy, or distally along the phalanx for arthrodesis.
- The dorsomedial cutaneous nerve to the hallux crosses the field immediately beneath the skin, often within the subcutaneous fat or just deep to the dermis.
- Look for the sentinel vein — a consistent superficial vein that lies beside the nerve and is the most reliable surface landmark for finding it.
- Gently dissect around the nerve and place a vessel loop or silastic tape for protection; raise full-thickness skin flaps medially and laterally with the nerve kept in view.
- Use bipolar haemostasis away from the nerve; never apply self-retaining retractors directly onto the nerve.
- Identify the EHL tendon laterally and the abductor hallucis tendon medially; these are retracted, never divided.
- Retract the EHL laterally with a Langenbeck or small Hohmann retractor and sweep the abductor hallucis plantarward.
- The dorsal metatarsal artery and accompanying veins may be encountered in the subcutaneous plane; cauterize only small branches under direct vision and preserve the major vessels.
- Make a longitudinal capsulotomy along the dorsomedial joint from the metatarsal neck to the proximal phalanx base, or a Y-shaped capsulotomy (stem along the dorsomedial line, limbs at the joint line) for wider exposure and later layered repair.
- Protect the medial collateral ligament and plantar plate during the capsular incision — excessive release risks hallux varus.
- Plantarflex the hallux to relax the sesamoid complex and expose the plantar aspect of the metatarsal head.
- Use small Hohmann or Langenbeck retractors to display the medial eminence, the metatarsal head articular surface, the proximal phalanx base and the sesamoid-metatarsal articulation.
- Remove any loose bodies, osteophytes or inflamed synovium; for cheilectomy, resect the dorsal osteophyte flush with an osteotome or burr and smooth the surface with a rasp.
- Hallux valgus — resect the medial eminence flush with the metatarsal shaft with an oscillating saw or osteotome, protecting the sesamoid complex; perform the planned osteotomy (chevron, scarf and so on).
- Arthrodesis — prepare the joint surfaces with flat cuts or conical reamers, correcting alignment to 10 to 15 degrees of dorsiflexion and 10 to 15 degrees of valgus.
- Synovectomy — debride inflamed synovium thoroughly.
- Release the tourniquet, irrigate copiously and achieve meticulous haemostasis; confirm the dorsomedial cutaneous nerve is intact and not entrapped.
- Plicate the medial capsule with a pants-over-vest or imbrication technique using absorbable suture, holding the hallux in slight varus (5 to 10 degrees) to ensure adequate medial tightening; repair the capsule in layers if a Y-shaped capsulotomy was used.
- Assess stability through a full range of motion, then close the skin with interrupted non-absorbable or running subcuticular suture and apply a sterile dressing with the hallux in slight varus and neutral dorsiflexion.
The single most important — and most often injured — structure in this exposure is the dorsomedial cutaneous nerve to the hallux, which crosses the field just beneath the skin. Injury causes a painful neuroma and dorsomedial numbness, the commonest source of patient dissatisfaction and litigation after hallux surgery. Identify it immediately after the skin incision (using the sentinel vein as a guide), loop it under loupes, keep it in view within full-thickness flaps, use bipolar cautery away from it, never clamp a self-retaining retractor onto it, and release retraction regularly.
Because the dorsomedial approach is entirely subcutaneous and extra-compartmental, it does not utilize a true internervous plane. The dissection passes between the EHL (deep peroneal nerve) laterally and the abductor hallucis (medial plantar nerve) medially, but both are simply retracted rather than divided. Safety therefore depends on early nerve identification, full-thickness flaps and staying dorsal to the abductor hallucis — not on a muscle interval.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Dorsomedial cutaneous nerve to hallux (just deep to dermis)
- Protection
- Identify immediately (sentinel vein landmark); vessel loop; full-thickness flaps; no self-retainers on the nerve
- Structure at risk
- Dorsal metatarsal artery and veins
- Protection
- Cauterize only small branches under direct vision; preserve major vessels
- Structure at risk
- Medial collateral ligament and plantar plate
- Protection
- Longitudinal or Y-shaped capsulotomy; preserve or repair; avoid over-release (hallux varus)
- Structure at risk
- Sesamoid complex and crista
- Protection
- Plantarflex the hallux; retract gently; avoid excessive force during eminence resection
- Structure at risk
- Extensor hallucis longus tendon
- Protection
- Retract laterally, never divide; protect during proximal extension
- Structure at risk
- Medial plantar nerve branches
- Protection
- Keep the incision dorsal to the abductor hallucis tendon
A terminal sensory branch of the medial dorsal cutaneous nerve (superficial peroneal), occasionally directly from the deep peroneal nerve. Injury is the signature complication — identify it first, every time. If inadvertently divided, bury the ends in muscle or bone to minimise neuroma.
Defines the lateral limit of the approach. Retract laterally but never divide; proximal extension requires identification and protection to prevent iatrogenic rupture or bowstringing (which causes hallux drop).
Provide medial and plantar stability. Preserve or repair if divided; excessive release can cause hallux varus or instability.
The medial (tibial) and lateral (fibular) sesamoids sit within the flexor hallucis brevis tendons and articulate with the plantar grooves of the metatarsal head, divided by the crista. Damage can cause sesamoiditis or transfer metatarsalgia.
Nerve injury management. If a clean transection is recognised intra-operatively, consider primary repair or bury the ends in muscle or bone to minimise neuroma; suspected postoperative neurapraxia is observed and documented; an established painful neuroma is managed with desensitisation, local anaesthetic injection and, if refractory, surgical exploration with proximal-stump burial. Extensile options. Extend proximally along the dorsomedial border of the first metatarsal shaft for scarf, proximal metatarsal osteotomy or shaft pathology — the EHL tendon and the more variable proximal nerve branches must be identified and protected. Extend distally along the dorsomedial proximal phalanx for arthrodesis, Akin osteotomy or Keller-Brandes resection arthroplasty — the nerve continues distally and the EHL insertion becomes relevant. A combined lateral release can usually be done through the same incision by retracting the metatarsal head laterally, or through a separate small first web-space incision in severe deformities. In revision surgery, previous incisions and scarring increase the difficulty of nerve identification and may demand a more extensile or alternative exposure. Complications
- Prevention
- Identify early, protect with vessel loop
- Management
- Bury ends in muscle or bone; counsel patient
- Prevention
- Careful flap elevation, bipolar cautery
- Management
- Direct pressure, fine ties, avoid cautery near nerve
- Prevention
- Identify and retract the tendon
- Management
- Primary repair if divided
- Prevention
- Preserve MCL and plantar plate
- Management
- Repair or imbricate if over-released
- Prevention
- Gentle retraction, protect the crista
- Management
- Address intra-operatively if recognised
- Incidence
- 2 to 8 percent
- Prevention
- Meticulous nerve protection
- Treatment
- Desensitisation, injection, surgical burial
- Incidence
- 1 to 3 percent
- Prevention
- Avoid over-plication, preserve lateral structures
- Treatment
- Revision soft tissue or osteotomy
- Incidence
- 5 to 15 percent
- Prevention
- Adequate plication, correct osteotomy
- Treatment
- Revision surgery
- Incidence
- 1 to 3 percent
- Prevention
- Sterile technique, prophylactic antibiotics
- Treatment
- Antibiotics, debridement if deep
- Incidence
- 5 to 10 percent
- Prevention
- Early range of motion exercises
- Treatment
- Physiotherapy, manipulation if refractory
- Incidence
- 3 to 8 percent
- Prevention
- Preserve sesamoid function, correct metatarsal length
- Treatment
- Orthotics, distal osteotomy if severe
Reported dorsomedial cutaneous nerve injury rates in hallux valgus surgery range from 2 to 15 percent depending on technique and the diligence of nerve protection. Most injuries are neurapraxias that recover, but a permanent painful neuroma in a small percentage is a major source of dissatisfaction. Meticulous identification and protection of the nerve is the single most important technical step in this approach.
Closure and aftercare. The capsule is closed with absorbable suture (pants-over-vest or imbrication for plication), subcutaneous tissue approximated, and skin closed without tension. Postoperatively the patient is weight-bearing as tolerated in a postoperative shoe, with elevation for 48 to 72 hours; early active and passive range of motion begins at 7 to 14 days, sutures are removed at 10 to 14 days, normal footwear resumes at 6 to 12 weeks, and full return to sport at 3 to 6 months, protecting the capsular repair throughout.
Procedures Through This Approach
- Chevron (Austin) osteotomy for mild hallux valgus — distal metatarsal osteotomy for mild deformity.
- First MTPJ arthrodesis — fusion for severe hallux rigidus, inflammatory arthritis or salvage.
- Cheilectomy — dorsal osteophyte resection and joint debridement for hallux rigidus.
- Distal soft tissue procedure (modified McBride), scarf osteotomy, proximal metatarsal osteotomy and Akin phalangeal osteotomy.
- Medial eminence resection with capsular plication; synovectomy for inflammatory arthropathy.
- Removal of osteochondral lesions or loose bodies; biopsy or curettage of benign bone lesions (for example intraosseous ganglion, enchondroma).
- Keller-Brandes resection arthroplasty (historical, rarely performed). Most hallux valgus operations combine soft-tissue balancing, osteotomy and an Akin procedure through this single extensile incision; a lateral release can be added through the same incision or via a separate first web-space incision.
Viva & Exam Focus
DORSOMEDDORSOMEDIAL APPROACH — the key steps
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old woman presents for hallux valgus corrective surgery and is anxious about numbness afterwards. How do you protect the nerve during the dorsomedial approach?”
“During hallux valgus surgery through a dorsomedial approach, how do you perform capsular closure and why is plication important?”
“A 55-year-old man with hallux rigidus and dorsal osteophytes is planned for cheilectomy. Describe the dorsomedial approach and the key steps for joint debridement.”
Position and landmarks
- Supine with a sandbag under the ipsilateral hip to internally rotate the leg
- Incision centered over the first MTPJ, just dorsal to the abductor hallucis
- Length 3 to 5 cm, extendable proximally or distally
- Dorsomedial cutaneous nerve often visible pre-incision (sentinel vein landmark)
- EHL defines the lateral boundary, abductor hallucis the medial limit
Internervous plane
- No true internervous plane — subcutaneous and extra-compartmental
- Dissection between EHL (deep peroneal) laterally and abductor hallucis (medial plantar) medially
- Safety depends on nerve identification rather than a muscle interval
- Stay dorsal to the abductor hallucis to protect the plantar medial nerve branches
Danger structures by layer
- Skin/subcutaneous: dorsomedial cutaneous nerve to hallux (identify first, vessel loop)
- Subcutaneous: dorsal metatarsal artery and veins (preserve major vessels)
- Capsular: medial collateral ligament and plantar plate (preserve or repair)
- Deep: sesamoid complex and crista (protect during retraction and resection)
- Lateral: EHL tendon (retract but never divide)
Step-by-step dissection
- Incise skin and subcutaneous tissue in one layer
- Identify and protect the dorsomedial cutaneous nerve immediately
- Raise full-thickness flaps medially and laterally
- Retract the EHL laterally and the abductor hallucis plantarward
- Perform a longitudinal or Y-shaped capsulotomy
- Plantarflex the hallux to expose the sesamoid complex
- Execute the procedure-specific steps
- Close with capsular plication for medial stability
Extension and procedures
- Proximal extension: along the metatarsal shaft for scarf or proximal osteotomy
- Distal extension: along the phalanx for arthrodesis or Akin osteotomy
- Procedures: chevron, scarf, distal soft tissue procedure, cheilectomy, MTPJ fusion
- Lateral release: through the same incision or a separate web-space incision
- Capsular plication is essential on closure to maintain correction
Closure and complications
- Capsular plication with absorbable suture, hallux in slight varus (5 to 10 degrees)
- Skin closure without tension on the flaps
- Nerve injury (2 to 8 percent): painful neuroma is the most significant complication
- Hallux varus (1 to 3 percent): avoid over-plication and lateral over-release
- Recurrence (5 to 15 percent): adequate plication and correct procedure selection
References
Global epidemiology. Hallux valgus affects approximately 20 to 30 percent of adults worldwide, with a higher prevalence in women and in populations that wear constrictive footwear. First MTPJ arthrodesis and cheilectomy are among the most common forefoot procedures performed by orthopaedic foot and ankle surgeons globally. Guidelines, registries and global practice. AAOS and AOFAS clinical practice guidelines emphasise the importance of nerve protection and proper capsular management in hallux valgus surgery; NICE and BOA guidance highlights the need to counsel patients about nerve injury risk; EFORT and national foot and ankle societies recommend the dorsomedial approach as the standard for most first MTPJ procedures. Registry data from the NJR, AJRR and national foot and ankle registries show low revision rates for properly performed chevron osteotomy and arthrodesis when nerve complications are avoided. Universally accepted technical principles are early identification and protection of the dorsomedial cutaneous nerve, capsular plication to maintain correction, avoidance of excessive medial release to prevent hallux varus, and deformity-matched procedure selection.
The surgical anatomy of the dorsomedial cutaneous nerve of the hallux
- The dorsomedial cutaneous nerve follows a constant anatomical course that makes it vulnerable during the dorsomedial approach.
- Meticulous identification immediately after incision prevents painful neuroma.
The sentinel vein: an anatomical guide to localisation of the dorsomedial cutaneous nerve in hallux surgery
- The sentinel vein is a reliable anatomical landmark for locating the dorsomedial cutaneous nerve.
- Using this landmark reduces the risk of nerve injury during the dorsomedial approach to the first MTP joint.
Anatomy of the dorsomedial cutaneous nerve to hallux and surgical implications according to the severity of hallux valgus deformity: a cadaveric study
- Nerve position varies with hallux valgus severity, requiring adjusted protection strategies in the dorsomedial approach.
- Cadaveric data support early nerve identification to minimise iatrogenic injury.
Hallux rigidus. Grading and long-term results of operative treatment
- Cheilectomy via the dorsomedial approach yields good long-term outcomes in lower-grade hallux rigidus with proper selection.
- Intraoperative grading and joint inspection through this approach guide treatment decisions effectively.