Gibson Interval | Digastric Trochanteric Osteotomy | MFCA Preservation | Z-Capsulotomy
- The digastric trochanteric osteotomy preserves gluteus medius to vastus lateralis continuity, keeping the deep branch of the medial femoral circumflex artery intact and the femoral head perfused.
- The deep branch of the MFCA runs along the superior border of quadratus femoris and ascends behind the osteotomy site — never place retractors on the posterior capsule and do not divide the short external rotators indiscriminately.
- A Z-shaped capsulotomy allows anterior dislocation of the head while the posterior capsule and labrum stay intact, preserving stability and blood supply.
- The approach is made through the Gibson interval between gluteus maximus (inferior gluteal nerve) and tensor fasciae latae (superior gluteal nerve).
- Secure trochanteric reattachment with two or three 3.5 mm or 4.5 mm cortical screws (or a cable system), aiming for anatomic reduction and compression, is essential for union.
When & Why
What it exposes. The Ganz trochanteric flip approach gives circumferential, 360-degree access to the femoral head, the head-neck junction and the acetabular rim — safely, without the avascular necrosis risk of a traditional dislocation. It is the gold-standard exposure for femoroacetabular impingement needing open osteochondroplasty, femoral head fractures (Pipkin types), osteochondral lesions, and acetabular rim pathology with labral repair. Why this approach (and not a standard one). Traditional posterior or anterior approaches cannot deliver the whole femoral head without jeopardising its blood supply. Ganz designed the digastric trochanteric osteotomy specifically so the trochanter — with gluteus medius and vastus lateralis still continuous — can be flipped anteriorly, leaving the deep branch of the MFCA undisturbed along the quadratus femoris. A Z-capsulotomy then permits anterior dislocation while the posterior capsule and labrum are preserved for stability. Position & landmarks. Most often lateral decubitus on a radiolucent table (beanbag or lateral supports, axillary and chest rolls, all pressure points padded, the entire leg prepped and draped free to allow full flexion, adduction and external rotation). Supine is an alternative when combined anterior work is planned. Position the C-arm for AP and cross-table lateral views without re-patient repositioning. Palpate and mark the anterior superior iliac spine, the greater trochanter, the vastus ridge (the inferior border of the trochanter and the start of the osteotomy), the iliac crest and the posterior superior iliac spine. Incision. The skin incision follows the Gibson interval — it begins about 6 to 8 cm proximal to the greater trochanter along a line toward the ASIS, curves posteriorly over the trochanter, then runs distally along the lateral femur for 8 to 10 cm (total 15 to 20 cm). The proximal limb reaches the iliac crest if needed; the distal limb allows extension onto the femoral shaft. Primary indications. - Symptomatic femoroacetabular impingement (cam, pincer or mixed) requiring osteochondroplasty and labral repair when arthroscopic access is insufficient
- Displaced femoral head fractures (Pipkin types I to IV) needing anatomic reduction and fixation
- Osteochondral lesions of the femoral head requiring grafting, microfracture or fixation
- Acetabular rim fractures and associated labral pathology
- Synovial chondromatosis or pigmented villonodular synovitis requiring complete synovectomy
- Selected benign tumours of the femoral head and neck (chondroblastoma, osteochondroma)
- Residual deformity after Perthes disease or slipped capital femoral epiphysis requiring correction Contraindications. Active infection around the hip; severe osteoporosis precluding secure trochanteric fixation; previous surgery with scarring that would compromise the MFCA; medical comorbidities precluding major surgery; and isolated posterior wall acetabular fractures, which are better treated through a Kocher-Langenbeck approach. Alternatives. Hip arthroscopy for contained cam lesions and simple labral tears; the Smith-Petersen anterior approach for limited anterior pathology; Kocher-Langenbeck for posterior wall and column acetabular fractures; and combined approaches for complex pelvic deformities.
The Exposure
Work down through the Gibson interval to the greater trochanter, perform the digastric osteotomy that defines the approach, protect the MFCA, then deliver the femoral head through a Z-capsulotomy.
Exposure sequence
- Skin incision follows the Gibson interval: about 6 to 8 cm proximal to the greater trochanter toward the ASIS, curving posteriorly over the trochanter, then distally along the lateral femur for 8 to 10 cm (total 15 to 20 cm).
- The entire leg is free-draped to the iliac crest so the hip can be flexed, adducted and externally rotated for dislocation.
- Incise skin and subcutaneous tissue in line with the incision and split the fascia lata over the greater trochanter.
- Develop the Gibson interval between gluteus maximus (inferior gluteal nerve) posteriorly and tensor fasciae latae (superior gluteal nerve) anteriorly — a relatively bloodless plane giving direct access to the trochanter.
- Protect the inferior branch of the superior gluteal nerve to the TFL during anterior retraction.
- Retract gluteus maximus posteriorly and the TFL anteriorly to expose the greater trochanter.
- Identify the vastus ridge inferiorly and the posterior border of the trochanter, and visualise the gluteus medius insertion.
- With an oscillating saw, start the osteotomy at the vastus ridge and direct the cut proximally and posteriorly to exit at the posterior border of the greater trochanter, proximal to the piriformis fossa.
- Keep the fragment about 1.5 to 2 cm thick and leave the vastus lateralis fascia attached to it.
- This is a digastric osteotomy — gluteus medius (superior gluteal nerve) and vastus lateralis (femoral nerve) remain one continuous musculotendinous unit, so the MFCA running posterior to the cut is undisturbed. Flip the fragment anteriorly and tag it with a heavy suture.
- With the trochanter flipped anteriorly, gently elevate gluteus minimus off the capsule and identify the piriformis and gemelli tendons posteriorly.
- Identify the deep branch of the MFCA running along the superior border of quadratus femoris; protect it with gentle retraction only — never place retractors on the posterior capsule and do not divide the external rotators.
- Perform a Z-shaped capsulotomy: begin anteriorly along the femoral neck, extend laterally along the acetabular rim to the level of the piriformis, then turn posteriorly. The posterior capsule is left intact.
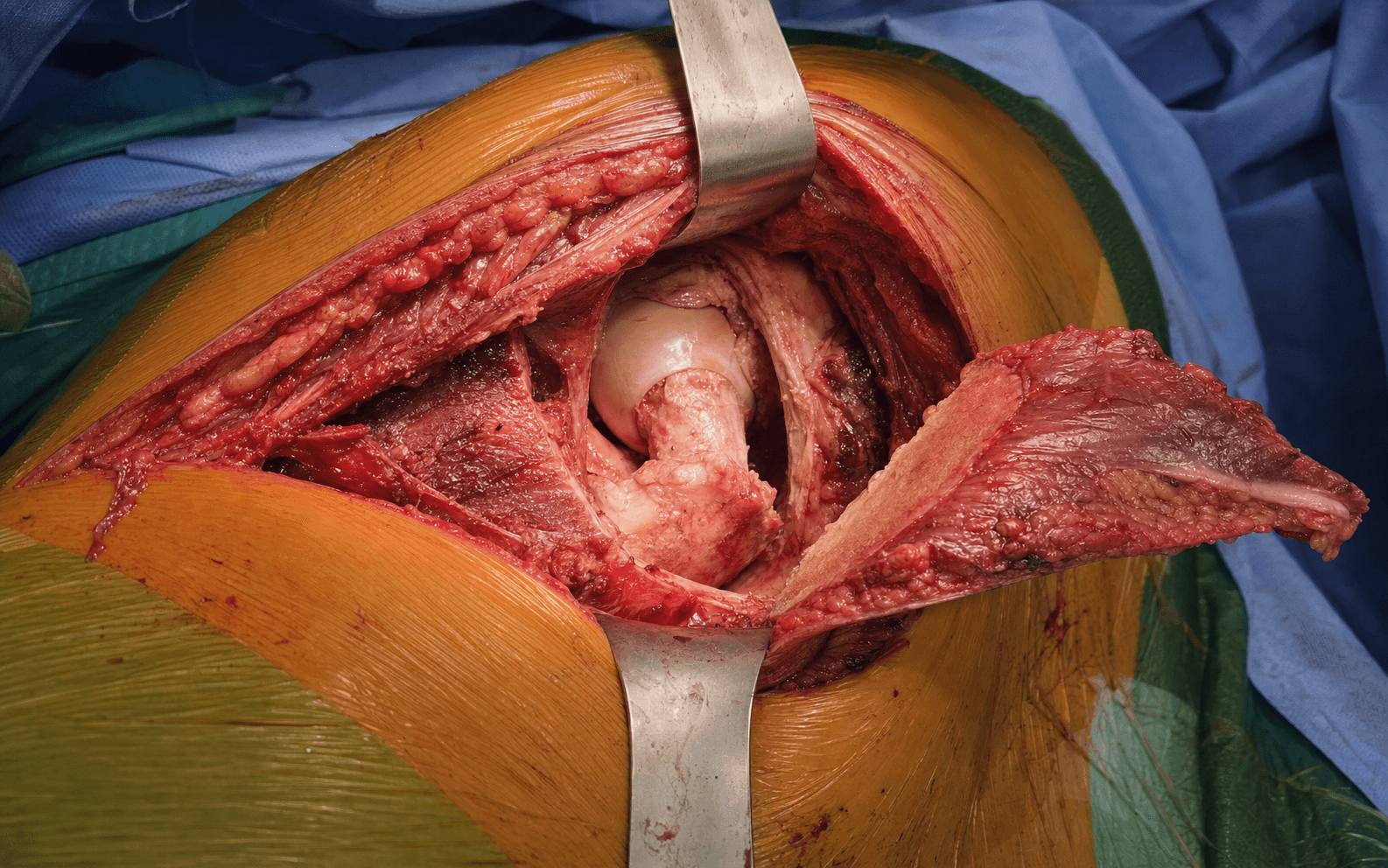
- Flex, adduct and externally rotate the hip to dislocate the femoral head anteriorly — the entire femoral head and acetabular rim are now exposed for osteochondroplasty, fracture fixation or labral work.
The deep branch of the medial femoral circumflex artery supplies most of the femoral head and its preservation is what makes this approach safe. It runs along the superior border of quadratus femoris and ascends behind the osteotomy site. Never place retractors on the posterior capsule, never divide the short external rotators indiscriminately, and stay extracapsular until the deliberate Z-capsulotomy. Injury causes avascular necrosis in 5 to 15 percent of cases.
By keeping gluteus medius and vastus lateralis attached to the same trochanteric fragment, the abductor sling stays continuous and the MFCA is undisturbed — there is no true deep internervous plane, the osteotomy itself is the plane. Start at the vastus ridge, exit proximal to the piriformis fossa, and keep the fragment 1.5 to 2 cm thick so it will accept screw fixation.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Inferior branch of superior gluteal nerve to TFL; lateral femoral cutaneous nerve
- Protection
- Develop the Gibson interval bluntly; avoid excessive anterior retraction
- Structure at risk
- Sciatic nerve (medial to gluteus maximus)
- Protection
- Gentle posterior retraction; avoid prolonged hip-flexion stretch
- Structure at risk
- Deep branch of MFCA along quadratus femoris
- Protection
- Identify early; never posterior capsular retractors; do not divide external rotators — injury causes AVN
- Structure at risk
- Superior gluteal neurovascular bundle
- Protection
- Limit proximal dissection to about 5 cm proximal to the ASIS; avoid excessive retraction (causes abductor weakness)
- Structure at risk
- Labrum and femoral head / acetabular cartilage
- Protection
- Careful Z-capsulotomy; pad retractors; handle the head gently with bone hooks padded with sponges
Extensile options. Extend proximally along the iliac crest to reach the ilium and acetabular roof (useful for combined periacetabular osteotomy or rim reconstruction), limited by the superior gluteal neurovascular bundle to roughly 5 cm proximal to the ASIS. Extend distally by splitting vastus lateralis in its midline to reach the femoral shaft (protect the nerve to vastus lateralis in the anterior third of the muscle). The approach can be combined with a Smith-Petersen for global acetabular access or with a posterior column approach for complex acetabular fractures, with staged positioning where needed. In revision cases with prior surgery the MFCA may be scarred — consider pre-operative angiography or proceed with extreme caution. Closure. Irrigate thoroughly, reduce the femoral head, and repair the capsule with heavy absorbable suture if possible (many surgeons leave the Z-capsulotomy open). Reattach the greater trochanter with two or three 3.5 mm or 4.5 mm cortical screws with washers, or a trochanteric cable system, aiming for anatomic reduction and compression. Close the fascia lata, subcutaneous tissue and skin in layers; drains are optional. Complications
- Rate
- 5 to 15 percent
- Note and prevention
- Anatomic reduction, multiple screws or cables, protected weight bearing; risk factors — poor fixation, smoking, osteoporosis
- Rate
- 5 to 15 percent
- Note and prevention
- Presents 6 to 24 months post-op; prevented by meticulous MFCA protection
- Rate
- 10 to 30 percent
- Note and prevention
- Prophylaxis with indomethacin or radiation in high-risk patients
- Rate
- Less than 1 percent
- Note and prevention
- Careful retraction, avoid prolonged stretch
- Rate
- 1 to 3 percent
- Note and prevention
- Routine peri-operative antibiotic prophylaxis
- Rate
- 2 to 5 percent
- Note and prevention
- LMWH or aspirin prophylaxis per protocol
Recovery. Touch or partial weight bearing (20 to 30 kg) for 6 to 8 weeks, advancing to full weight bearing at 8 to 12 weeks once trochanteric union is radiographic. Aim for 0 to 90 degrees flexion by 6 weeks; start abduction exercises at 6 weeks and avoid resisted abduction until 8 to 12 weeks. Follow-up radiographs at 2, 6 and 12 weeks, then 6 months and 1 year to watch for AVN.
Procedures Through This Approach
- Femoroacetabular impingement osteochondroplasty (cam and pincer resection) with labral preservation.
- Femoral head fracture fixation (Pipkin types I to IV) under direct vision, using headless compression screws or bioabsorbable pins.
- Osteochondral lesion grafting, microfracture or fixation.
- Acetabular rim fracture fixation and labral repair.
- Selected femoral head osteonecrosis core decompression with grafting.
- Excision of benign tumours of the head and neck (chondroblastoma, osteochondroma).
- Synovial chondromatosis or pigmented villonodular synovitis debridement and complete synovectomy.
Viva & Exam Focus
GANZ HIPGANZ HIP — the safe surgical dislocation sequence
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old male with symptomatic cam-type FAI has failed conservative treatment. Describe how you would perform surgical dislocation using the Ganz approach, focusing on MFCA protection.”
“During a Ganz approach for a Pipkin II femoral head fracture, you notice the MFCA deep branch appears stretched but intact. What are your immediate and post-operative considerations?”
“A patient develops a Trendelenburg gait and trochanteric nonunion 4 months after a Ganz approach. What technical factors during the index procedure likely contributed and how would you revise?”
Positioning & setup
- Lateral decubitus most common — entire leg free draped
- Supine alternative when combined anterior work is planned
- C-arm for AP and lateral hip views
- Landmarks: ASIS, greater trochanter, vastus ridge, iliac crest
The exposure
- Gibson interval (gluteus maximus vs TFL) is the superficial internervous plane
- Digastric trochanteric osteotomy 1.5 to 2 cm thick — the deep step, no true plane
- Z-capsulotomy for anterior dislocation with the posterior capsule intact
- Secure trochanteric reattachment with two or three screws or a cable system
Dangers
- Deep branch of MFCA along quadratus femoris — AVN if injured
- Sciatic nerve medial to gluteus maximus (less than 1 percent)
- Superior gluteal neurovascular bundle limits proximal extension
- Labrum and cartilage during capsulotomy and dislocation
Indications
- FAI osteochondroplasty (cam and pincer)
- Femoral head fractures (Pipkin I to IV)
- Osteochondral lesions requiring grafting or fixation
- Acetabular rim pathology and labral repair
Complications
- Trochanteric nonunion 5 to 15 percent
- AVN 5 to 15 percent if the MFCA is injured
- Heterotopic ossification 10 to 30 percent
- Sciatic nerve injury less than 1 percent
References
Safe surgical dislocation of the hip
The original description of the trochanteric flip approach. The digastric osteotomy preserves the MFCA blood supply to the femoral head, the Z-capsulotomy permits 360-degree visualisation while maintaining stability, and excellent outcomes were demonstrated in FAI and femoral head pathology with minimal complications.
Long-term outcomes of surgical hip dislocation
Long-term review confirming that surgical hip dislocation via the trochanteric flip gives reliable, extensile access for complex hip pathology with low complication rates when the digastric osteotomy and MFCA protection are performed correctly.
Surgical dislocation of the hip for femoroacetabular impingement
Large series confirming the Ganz approach as the standard for open FAI treatment, with low rates of AVN and trochanteric complications when the technique is followed precisely, and efficacy for both cam and pincer lesions with labral preservation.
Femoral head fractures treated with the Ganz approach
Series of Pipkin fractures treated with surgical dislocation showing anatomic reduction is achievable, with AVN rates comparable to or lower than traditional approaches when the MFCA is protected; advocates its use in displaced femoral head fractures requiring direct visualisation.