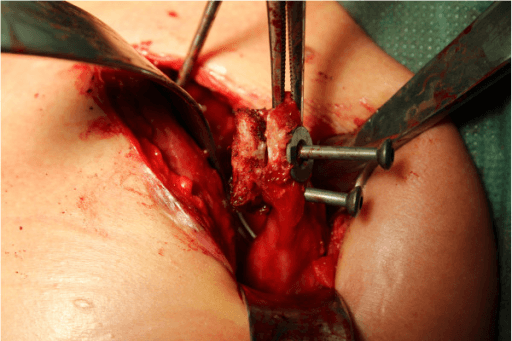
Open deltopectoral approach — coracoid harvest and transfer to the anterior glenoid via a subscapularis split — advanced
- Primary indication is anterior shoulder instability with critical glenoid bone loss greater than 20–25% OR an off-track Hill-Sachs lesion — bone loss is quantified on 3D CT using the best-fit circle method
- The sling effect of the conjoint tendon is the key biomechanical principle — it acts as a dynamic anterior buttress, tensioning the inferior subscapularis in abduction-external rotation regardless of whether the graft bone heals
- The coracoid graft must be placed FLUSH with (or 1 mm proud of) the glenoid articular surface — medial placement is the single most important technical error causing recurrence
- The musculocutaneous nerve enters coracobrachialis 3–8 cm from the coracoid tip (mean 5.4 cm) — excessive distal dissection or over-retraction of the conjoint tendon risks permanent elbow flexion weakness
When & Why
Indication. The Latarjet coracoid transfer is performed for recurrent anterior shoulder instability with significant bone loss or a high-risk soft-tissue failure pattern — the setting in which an arthroscopic Bankart repair alone has an unacceptably high recurrence rate. It is an open, bony augmentation procedure. Absolute indications (strong evidence): - Glenoid bone loss greater than 20–25% on 3D CT (best-fit circle method) — the inverted-pear morphology on a plain radiograph is the clinical proxy
- Off-track Hill-Sachs lesion: the Hill-Sachs interval is wider than the glenoid track (Di Giacomo glenoid-track concept) even with glenoid bone loss less than 20%
- Failed arthroscopic Bankart with recurrent instability — especially with progressive bone loss
- ISIS score of 6 or greater in a contact athlete — a 70% predicted failure rate from arthroscopic Bankart justifies a primary Latarjet Strong relative indications: - Bone loss of 13.5–20% in a high-demand contact athlete (rugby, football) or an ISIS score of 4–5
- Epilepsy with recurrent seizure-related dislocations — repeated re-dislocation mandates a durable bony reconstruction
- Poor labral tissue quality (attenuation, absence, prior failed repair) — there is no tissue to repair arthroscopically
- A significant Hill-Sachs lesion (greater than 25% of humeral head width) where remplissage would excessively limit external rotation The decision — when to abandon arthroscopic Bankart. Bone loss, not soft-tissue technique, is the dominant driver of Bankart failure (Burkhart and De Beer, 2000). The Instability Severity Index Score (ISIS, Balg and Boileau 2007) quantifies that risk pre-operatively. It is a 10-point score (range 0–10 — it caps at 10, not 11): a score greater than 6 predicts a 70% recurrence risk after arthroscopic Bankart, supporting a primary Latarjet instead.
- Points
- 2
- Points
- 2
- Points
- 1
- Points
- 1
- Points
- 2
- Points
- 2
- Points
- Score over 6 = consider Latarjet
- Arthroscopic Bankart
- Less than 13.5%
- Remplissage + Bankart
- Less than 20% glenoid with off-track Hill-Sachs
- Latarjet / Coracoid Transfer
- Greater than 20–25% glenoid OR off-track with greater than 15% glenoid loss
- Arthroscopic Bankart
- On-track only
- Remplissage + Bankart
- Off-track engaging lesion
- Latarjet / Coracoid Transfer
- Large or combined with significant glenoid loss
- Arthroscopic Bankart
- Labral bumper + IGHL tensioning
- Remplissage + Bankart
- Fills Hill-Sachs defect, prevents engagement
- Latarjet / Coracoid Transfer
- Bone block + sling effect + capsular reconstruction
- Arthroscopic Bankart
- 5–8% overall; up to 20–25% in contact athletes
- Remplissage + Bankart
- 5–8% combined (vs 18% Bankart alone for off-track)
- Latarjet / Coracoid Transfer
- 5–8% overall; 2–4% in ideal cases
- Arthroscopic Bankart
- 5–10 degrees (acceptable)
- Remplissage + Bankart
- 10–20 degrees (fills posterior defect)
- Latarjet / Coracoid Transfer
- 5–15 degrees
- Arthroscopic Bankart
- Score less than 6
- Remplissage + Bankart
- Score 4–6 with off-track lesion
- Latarjet / Coracoid Transfer
- Score 6 or greater
- Arthroscopic Bankart
- Arthroscopic, anatomic, quick recovery
- Remplissage + Bankart
- Avoids Latarjet when the glenoid is intact
- Latarjet / Coracoid Transfer
- Durable even if the graft lyses (sling persists)
- Arthroscopic Bankart
- Fails with bone loss; high contact-sport recurrence
- Remplissage + Bankart
- ER restriction may affect throwers
- Latarjet / Coracoid Transfer
- Open procedure, nerve risk, graft lysis
Consent. Counsel specifically on the true early complication burden: transient or permanent nerve injury (most often the musculocutaneous nerve, 0.8–8%), recurrent instability (5–8%), graft lysis on CT (15–30% at 5 years, which does not equal failure), hardware problems (3–5%), and glenohumeral arthritis progression (around 30% radiographic arthritis at 10 years). Document elbow flexion and lateral forearm sensation on day one. Setup. Beach-chair position, 30–45 degrees head-up, arm free-draped over the edge of the table. Mark the coracoid tip, anterior acromion and deltopectoral groove before prep — the coracoid is the key landmark, and all dissection references from it.
The Operation
The goal is to expose the anterior glenoid through the deltopectoral approach, harvest the coracoid, pass it through a subscapularis split, and fix it flush to the anteroinferior glenoid rim — restoring stability by three mechanisms: a bone block that extends the articular arc, the sling effect of the conjoint tendon, and capsular reconstruction using the preserved coracoacromial ligament stump. The exposure and coracoid harvest are laid out in full as the first steps below.
Operative sequence
- Beach-chair, 30–45 degrees head-up, head neutral on a padded horseshoe; arm free-draped over the table edge with an arm holder (permits single-surgeon technique).
- Ipsilateral arm in slight abduction and forward flexion for exposure.
- Mark the coracoid tip, anterior acromion edge and deltopectoral groove before prep.
- 6–8 cm incision from 2 cm medial to the coracoid tip, curving distally along the deltopectoral groove toward the deltoid insertion.
- Internervous plane: the deltopectoral interval — deltoid (axillary nerve) versus pectoralis major (medial and lateral pectoral nerves). It is truly internervous.
- Identify the cephalic vein in the groove and retract it laterally with the deltoid (preserves venous drainage, reduces haematoma risk).
- Develop the interval sharply distally; identify the coracoid tip beneath the clavipectoral fascia.
- Incise the clavipectoral fascia lateral to the conjoint tendon to open the subcoracoid space.
- Release pectoralis minor from the medial coracoid surface under direct vision.
- Score the coracoacromial ligament 1 cm from the coracoid tip — the lateral stump is preserved for later capsular repair.
- Place a curved Hohmann retractor under the coracoid base; protect the brachial plexus medially.
- Osteotomy: oscillating saw or 15 mm osteotome at the coracoid base, perpendicular to the coracoid shaft. Deliver the graft and confirm a 2.0–2.5 cm length.
- Prepare the flat surface: rongeur or high-speed burr to flatten the inferomedial coracoid surface (this is the face that will contact the glenoid neck).
- Drill two parallel holes through the graft, 25–30 mm apart, for 3.5 mm cortical screws (countersink the entry holes).
- Identify the subscapularis tendon; mark the junction of the lower two-thirds and the upper one-third with electrocautery — this level is critical and is NOT the midpoint.
- Split the subscapularis horizontally with scissors and index finger, length 3–4 cm, from the lateral tendon toward the medial muscle.
- Retract the upper and lower halves with blunt self-retaining retractors, exposing the anterior shoulder capsule and glenoid neck.
- Incise the anterior capsule horizontally in line with the subscapularis split.
- Elevate the capsulolabral tissue from the anterior glenoid neck subperiosteally (Cobb elevator).
- Decorticate the anteroinferior glenoid neck with a rongeur or burr to create a bleeding cancellous recipient bed (approximately 20 mm wide by 25 mm tall — matches the graft footprint).
- Confirm the glenoid articular margin with a probe — the graft surface must end flush with this margin.
- Pass the coracoid graft through the subscapularis split with its flat surface facing the glenoid neck; the conjoint tendon lies inferior to the split (the sling position).
- Align the graft so its inferior edge sits at the 4–5 o'clock position on the glenoid (covers the critical anteroinferior defect).
- Key checkpoint: the graft articular surface must be flush (0–1 mm proud) with the glenoid articular cartilage — not medial, not lateral.
- Hold position with a temporary K-wire; confirm with intraoperative fluoroscopy (axillary view) before definitive fixation.
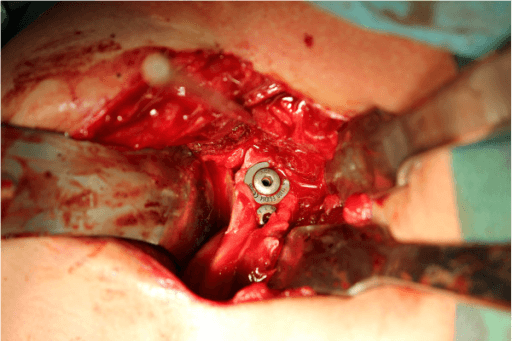
- Insert the proximal 3.5 mm cortical screw first, then the distal screw; tighten sequentially. Confirm both screws are parallel, within the graft, and not penetrating the posterior glenoid cortex.
- Suture the preserved lateral stump of the coracoacromial ligament to the medial capsular tissue (residual anterior capsule and labrum).
- 2–3 interrupted absorbable sutures (Number 1 Vicryl or equivalent).
- This is the third mechanism of stability — capsular reconstruction.
- Confirm haemostasis; copious irrigation.
- The subscapularis split does NOT require formal repair — it closes spontaneously as the arm adducts.
- Close the deltopectoral fascia with absorbable sutures; subcutaneous and skin closure per surgeon preference.
- Apply a sling with the arm in 15 degrees of forward flexion and neutral rotation.
The musculocutaneous nerve is the most commonly injured nerve in Latarjet (0.8–8%). It enters coracobrachialis 3–8 cm from the coracoid tip (mean 5.4 cm, range 3–10 cm depending on patient height). Excessive distal retraction of the conjoint tendon stretches the nerve at its entry point. Prevent it: identify the nerve before any distal release, limit conjoint-tendon retraction to less than 2–3 cm below the coracoid tip, use flat retractors on bone (not hooks dragging soft tissue), and release retraction periodically. In the short-statured patient the nerve may lie only 3 cm from the coracoid tip.
A graft placed medial to the glenoid articular surface fails to extend the arc and causes recurrent instability despite healed bone. The graft surface must be flush with the glenoid face (0–1 mm lateral). Confirm with intraoperative axillary fluoroscopy at the time of fixation. A medially placed graft on a postoperative CT is an indication for revision.
In abduction-external rotation (the position of instability), the conjoint tendon lying inferior to the subscapularis split tenses and transmits a compressive force to the anteroinferior glenoid — a dynamic anterior buttress independent of graft healing. Provided the split is at the correct level and the tendon is uninjured, the sling persists even if the bone graft lyses completely over the years. This is the concept that makes Latarjet durable.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 — Protection | Weeks 0–4 | Sling in 15 degrees forward flexion, neutral rotation | Pendulum exercises from day 1; hand, wrist, elbow ROM unrestricted; no active shoulder motion against resistance | | 2 — Early motion | Weeks 4–8 | Sling discontinued at 4 weeks | Active-assisted ROM: elevation in the scapular plane to 90 degrees, external rotation to neutral then 20 degrees; scapular stabilisation; no subscapularis strengthening until week 6 | | 3 — Strengthening | Weeks 8–16 | — | Full active ROM; progressive rotator-cuff strengthening; closed-chain proprioception; sport-specific (non-contact) drills from 12 weeks; optional CT at 12 weeks to confirm graft incorporation | | 4 — Return to sport | Months 4–6 | — | Contact training from 4 months when full strength and ROM achieved; full contact sport return at 6 months minimum; criterion-based discharge (greater than 90% limb symmetry index, full pain-free ROM) |
- Latarjet
- 4 weeks
- Arthroscopic Bankart
- 4 weeks
- Latarjet
- 4–6 weeks
- Arthroscopic Bankart
- 4–6 weeks
- Latarjet
- 10–12 weeks
- Arthroscopic Bankart
- 8–10 weeks
- Latarjet
- 8 weeks
- Arthroscopic Bankart
- 6–8 weeks
- Latarjet
- 3–4 months
- Arthroscopic Bankart
- 3 months
- Latarjet
- 5–6 months
- Arthroscopic Bankart
- 4–6 months
- Latarjet
- 74–97%
- Arthroscopic Bankart
- 65–85%
- Latarjet
- Mild restriction 5–15 degrees
- Arthroscopic Bankart
- Minimal restriction 0–10 degrees
Expected outcomes. Recurrence rate 5–8% overall (2–4% in appropriately selected patients at 10 years); return to sport 74–97% across series (contact athletes 80–90%); mean external rotation loss 5–10 degrees (clinically acceptable); CT-confirmed graft union in 70–85% at 6 months; 85–95% satisfied or very satisfied at 5 years. Complications
- Incidence
- 0.8–8%
- Prevention
- Limit distal retraction to less than 2–3 cm; identify the nerve
- Management
- Observation; 90% recover by 6 months; EMG at 6 weeks
- Incidence
- 5–8%
- Prevention
- Flush graft placement; correct split level
- Management
- CT to assess graft; revision Latarjet or allograft if medial graft
- Incidence
- 15–30% at 5 years
- Prevention
- Cortical screws; adequate graft bed preparation
- Management
- Observation if asymptomatic; revision only if instability recurs
- Incidence
- 3–5%
- Prevention
- Cortical screws (not cancellous); confirm purchase on fluoroscopy
- Management
- Revision surgery; remove prominent hardware
- Incidence
- 3–8%
- Prevention
- Correct split level; avoid a superior split
- Management
- Physiotherapy; ultrasound-guided injection; rarely revision
- Incidence
- ~30% at 10 years
- Prevention
- Flush graft position; no over-lateral placement
- Management
- Activity modification; reverse TSA preferred for severe arthritis
- Incidence
- 2–4%
- Prevention
- Haemostasis; bipolar to the circumflex vessels
- Management
- Aspiration if tense; operative evacuation if compressing neurovascular structures
- Incidence
- Less than 0.5%
- Prevention
- Identify the nerve before inferior dissection
- Management
- Observation; exploration if no recovery at 4 months
Graft lysis does NOT equal failure. CT evidence of graft resorption appears in 15–30% at 5 years, but the sling mechanism preserves stability provided the conjoint tendon remains correctly positioned. Revise only for symptomatic recurrent instability when CT confirms the sling is compromised (graft medially displaced or conjoint tendon detached). Factors associated with lysis include screw divergence, a thin graft, excessive bone-bed preparation and infection. Long-term arthritis. Arthritis progression is the most significant long-term concern — around 30% radiographic arthritis at 10 years, comparable to post-instability arthritis without surgery. Causes include an over-lateral graft (proud screw heads), hardware impingement and loss of normal articular geometry. When severe, reverse shoulder arthroplasty is preferred over anatomic TSA because the subscapularis is unreliable after Latarjet.
Viva & Exam Focus
LATARJETLATARJET — steps of the procedure
GRAFTGRAFT — complications of Latarjet
Critical exam pitfalls
Most common nerve injury in Latarjet (0.8–8%). Enters coracobrachialis 3–8 cm from the coracoid tip (mean 5.4 cm). Test elbow flexion and lateral forearm sensation postoperatively; avoid retraction greater than 2–3 cm distal to the coracoid and identify the nerve before any distal release.
The most critical technical error. A graft placed medial to the articular surface fails to extend the arc and causes recurrence despite healed bone. The graft must sit flush (0–1 mm proud); confirm on intraoperative fluoroscopy. Medial graft on postoperative CT equals revision.
The split is at the junction of the lower two-thirds and upper one-third — NOT the midpoint. The intact lower two-thirds forms the sling, tensioning in abduction-external rotation. A split that is too superior damages the upper half and weakens internal rotation.
Screws must be parallel, in the midline of the graft and 25–30 mm apart, with tips not penetrating the posterior glenoid cortex. Proud screws abrade the humeral head and accelerate arthritis. Confirm on the axillary view.
Resorption on CT occurs in 15–30% at 5 years. A common exam trap is to panic and recommend revision. It does NOT equal failure — the sling maintains stability. Revise only for symptomatic recurrence with poor graft position.
First establish WHY: check the original graft/screw position on CT and conjoint-tendon integrity on MRI. Options: revision Latarjet (if coracoid available), Eden-Hybinette (iliac crest autograft or distal tibial allograft), or reverse TSA for established arthritis. Revision recurrence is 15–25%.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old male rugby player presents with his fourth anterior shoulder dislocation over 18 months. He plays competitive provincial rugby as a flanker. His plain AP radiograph of the shoulder in internal rotation shows the classic inverted-pear appearance of the glenoid. Describe your assessment and management.”
“You perform a Latarjet on a 28-year-old male. On day 1 postoperatively he reports numbness and weakness in his index and middle fingers with weak elbow flexion on the right side. What nerve has been injured, why is it at risk in this procedure, and how do you manage it?”
“A 32-year-old male presents 3 years after a Latarjet for recurrent anterior shoulder instability. CT shows near-complete graft lysis. He has had two more dislocation episodes in the past 6 months. What are your options?”
Top indications
- Glenoid bone loss greater than 20–25% (inverted-pear sign)
- Off-track Hill-Sachs lesion
- ISIS score of 6 or greater in a contact athlete
- Failed arthroscopic Bankart with recurrent instability
- Epilepsy with recurrent seizure dislocations
- Poor labral tissue quality (attenuation / prior failed repair)
Three mechanisms of stability
- Bone block: coracoid graft extends the anterior articular arc
- Sling effect: conjoint tendon below the subscapularis split tenses in ABER
- Capsular reconstruction: lateral coracoacromial ligament to residual capsule
- The sling persists even if the graft lyses completely
- Graft lysis alone (without recurrence) does NOT require revision
Key steps (LATARJET)
- Deltopectoral approach; cephalic vein retracted laterally
- Coracoid harvest: 2.0–2.5 cm, pectoralis minor released, flat surface prepared
- Subscapularis split at the junction of lower two-thirds and upper one-third (NOT the midpoint)
- Anterior capsulotomy and glenoid-neck decortication
- Graft positioned FLUSH with the articular surface (0–1 mm) — NOT medial
- Two 3.5 mm cortical screws, 25–30 mm apart, parallel
- Capsular repair: coracoacromial ligament stump to residual capsule
Critical technical points
- Graft flush with the articular surface: medial placement is the number-one cause of recurrence
- Subscapularis split level: lower two-thirds and upper one-third junction, NOT the midpoint
- Musculocutaneous nerve: mean 5.4 cm from the coracoid tip — limit distal retraction
- Confirm graft position on intraoperative axillary fluoroscopy
- Cortical screws (not cancellous) to prevent back-out
Complications (GRAFT)
- Graft lysis: 15–30% at 5 years, does NOT equal failure
- Recurrence: 5–8% overall, usually from medial graft placement
- Axillary / musculocutaneous nerve: musculocutaneous most common (0.8–8%)
- Fixation failure: hardware back-out 3–5%, non-union 2–5%
- Tight repair / subscapularis dysfunction: ER loss greater than 20 degrees
ISIS score thresholds
- Score less than 6: arthroscopic Bankart appropriate (5–10% recurrence)
- Score over 6: consider Latarjet as the primary procedure (70% Bankart failure)
- Scoring: age less than 20 (2), competitive sport (2), contact/overhead sport (1), hyperlaxity (1), Hill-Sachs on AP (2), loss of glenoid contour on AP (2)
- Maximum score: 10 points
Rehabilitation milestones
- Sling 4 weeks
- Active ROM commenced at 4–6 weeks
- Full ROM expected by 10–12 weeks
- Strengthening from 8 weeks
- Non-contact sport at 3–4 months
- Full contact sport return at 6 months minimum
Background & Evidence
Why bone loss drives failure. Anterior dislocation is the most common direction of shoulder dislocation, and recurrence after a first dislocation is frequent — especially in the young, contact-sport population. The dominant determinant of failure after a soft-tissue (Bankart) repair is bony deficiency: an inverted-pear glenoid (loss of the normal inferior glenoid width) and an engaging Hill-Sachs lesion. Burkhart and De Beer (2000) showed that shoulders with significant bone defects had a 67% recurrence rate after arthroscopic Bankart versus 4% without, and 89% in contact athletes with defects — the foundational rationale for choosing Latarjet. Surgical anatomy that governs the operation. - Subscapularis and the split. Subscapularis arises from the subscapular fossa and inserts on the lesser tuberosity, with distinct upper (upper subscapular nerve, C5) and lower (lower subscapular nerve, C5–C6) neurovascular territories. The split is made at the junction of the lower two-thirds and upper one-third — the intact lower two-thirds becomes the sling, tensioning in abduction-external rotation. A split that is too superior damages the upper half (responsible for internal-rotation strength) and weakens the lift-off and belly-press.
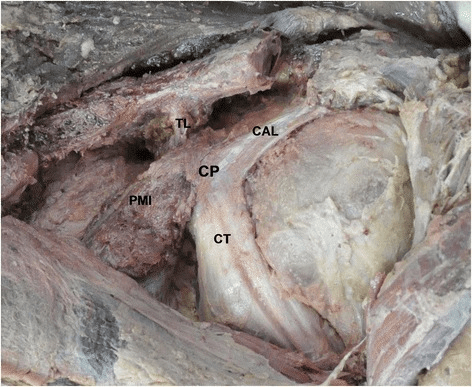
- Coracoid and conjoint tendon. The coracoid projects anterolaterally from the supraglenoid scapular base; its tip lies 1–2 cm medial and 1–2 cm inferior to the AC joint. Pectoralis minor inserts on the medial coracoid (released during harvest); coracobrachialis and the short head of biceps arise at the tip (preserved as the conjoint tendon). The flat inferomedial coracoid surface is the graft contact face; the deep coracoid surface bears a hyaline-like fibrocartilage. Only the coracoacromial ligament is divided — the coracoclavicular ligaments (conoid and trapezoid) are preserved.
- Axillary nerve. Exits the quadrangular space with the posterior circumflex humeral artery and courses anteroinferiorly along the inferior subscapularis, lying approximately 12–15 mm inferior to the glenoid rim at the 6 o'clock position. At risk during inferior capsulotomy and inferior screw placement; injury (less than 0.5%) causes deltoid paralysis and lateral shoulder numbness.
- Anterior circumflex humeral vessels. Arise from the third part of the axillary artery and run along the lower border of subscapularis (contributing the arcuate artery to humeral head supply). Coagulate with bipolar before division during the inferior capsulotomy. The decision tools — ISIS and the glenoid track. Balg and Boileau (2007) derived the 10-point ISIS in 131 patients; a score greater than 6 carried a 70% recurrence risk after arthroscopic Bankart, recommending a Bristow-Latarjet instead (the score was validated multicentre by Rouleau, ICC 0.933). Yamamoto and Itoi (2007) defined the glenoid track: the medial margin of glenohumeral contact lies a mean 84% of the glenoid width medial to the rotator-cuff footprint, so a Hill-Sachs lesion extending medial to that margin is off-track and at risk of engagement — justifying bony augmentation in bipolar bone loss even when glenoid loss alone is subcritical.
References
Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion
- 194 consecutive arthroscopic Bankart repairs analysed; shoulders with significant bone defects (inverted-pear glenoid or engaging Hill-Sachs) had a 67% recurrence rate versus 4% without defects
- Contact athletes with bone deficits had an 89% recurrence rate, versus 6.5% in contact athletes without defects
- Defined the inverted-pear glenoid and the engaging Hill-Sachs lesion and recommended Latarjet coracoid grafting for significant glenoid bone loss
The instability severity index score: a simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation
- Prospective case-control study of 131 patients undergoing arthroscopic Bankart repair; overall recurrent instability 14.5% at a mean 31 months
- Derived a 10-point pre-operative Instability Severity Index Score (ISIS) from age under 20, competitive or contact/overhead sport, hyperlaxity, Hill-Sachs on AP radiograph and loss of the inferior glenoid contour
- A score greater than 6 points carried a 70% recurrence risk, on which basis the authors deemed arthroscopic Bankart contraindicated and recommended a Bristow-Latarjet procedure
Contact between the glenoid and the humeral head in abduction, external rotation, and horizontal extension: a new concept of glenoid track
- Nine cadaveric shoulders tested in abduction, external rotation and horizontal extension to map the zone of glenohumeral contact (the glenoid track)
- The medial margin of the glenoid track lay a mean 18.4 mm medial to the rotator-cuff footprint, equivalent to 84% of the glenoid width
- A Hill-Sachs lesion extending medial to the track margin is at risk of engagement and dislocation (an off-track lesion)
Short-term complications of the Latarjet procedure
- 48 Latarjet shoulders with anterior glenoid bone deficiency or prior failed Bankart; overall complication rate 25%
- Recurrent instability 8%, neurologic injury 10% (musculocutaneous, axillary, radial — mostly transient sensory neurapraxia resolving by 2 months), superficial infection 6%
- Two patients had persistent axillary nerve sensory disturbance, underscoring that not all nerve injuries fully recover
Validation of the instability shoulder index score in a multicenter reliability study in 114 consecutive cases
- Prospective multicentre (North America and Europe) study of 114 patients with anterior shoulder instability
- The ISIS showed very high interobserver reliability (intraclass correlation coefficient 0.933)
- Patients undergoing more complex procedures (remplissage or open Latarjet) had higher mean ISIS scores, supporting its use to guide surgical selection
Treatment of recurrent dislocation of the shoulder — original coracoid transfer
The original description of coracoid process transfer to the anterior glenoid rim for recurrent anterior shoulder dislocation — the foundation of all subsequent modifications of the procedure.