Aponeurotic release or conjoined-tendon lengthening for isolated gastrocnemius contracture · intermediate
- The Silfverskiöld test is the cornerstone: assess ankle dorsiflexion with the knee extended and then flexed to 90 degrees. If dorsiflexion improves with knee flexion, the contracture is isolated to the gastrocnemius and a recession is appropriate. If it does not change, the whole gastrocnemius-soleus-Achilles complex is tight and a recession will under-correct — a tendo-Achilles lengthening is needed.
- The Strayer procedure (the workhorse) releases the gastrocnemius aponeurosis from the soleus fascia in the proximal-mid calf. The gastrocnemius retracts proximally, lengthening the gastrocnemius component only and preserving soleus push-off. The sural nerve crosses the field posterolaterally and must be identified and protected.
- Gastrocnemius recession is an adjunct, not a primary treatment. It addresses the biomechanical contributor (equinus) when non-operative care for the primary pathology has failed, and the decision to add it rests on a positive Silfverskiöld test.
- Avoid over-lengthening: excessive release causes push-off weakness, recurrent equinus, or a calcaneal gait. Aim for 5 to 10 degrees of dorsiflexion beyond neutral, checking with the knee extended and flexed intra-operatively.
When & Why
The gatekeeper test. Gastrocnemius recession is only appropriate when the contracture is isolated to the gastrocnemius. The Silfverskiöld test decides this: assess ankle dorsiflexion with the knee extended, then flexed to 90 degrees. If dorsiflexion improves by at least 5 degrees with the knee flexed, the soleus has been slackened and the contracture is isolated to the gastrocnemius (a positive test) — recession is the correct operation. If dorsiflexion does not change, the contracture involves the soleus or the entire tendo-Achilles (a negative test) and a recession will under-correct; a formal tendo-Achilles lengthening is required instead. Normal ankle dorsiflexion is at least 10 degrees beyond neutral with the knee extended. Absolute indications — an isolated gastrocnemius contracture (positive Silfverskiöld test) demonstrated as a biomechanical contributor to:
- Forefoot or midfoot pathology (metatarsalgia, midfoot overload) that has failed non-operative treatment
- Recurrent or recalcitrant plantar fasciitis after at least 6 to 12 months of structured non-operative care (stretching programme, orthotics, physiotherapy, night splint, at least one corticosteroid injection)
- Diabetic forefoot ulceration refractory to offloading and wound-care optimisation Relative indications:
- Non-insertional Achilles tendinopathy with isolated gastrocnemius contracture, failed non-operative treatment
- Flatfoot deformity where gastrocnemius contracture contributes to hindfoot valgus — recession as an adjunct to flatfoot reconstruction
- Paediatric equinus — cerebral palsy or idiopathic toe-walking (Baumann or Strayer)
- Chronic ankle stiffness / anterior impingement where gastrocnemius tightness limits dorsiflexion Contraindications. Absolute: a negative Silfverskiöld test (recession under-corrects; TAL required); active infection at the surgical site or ipsilateral limb; severe peripheral vascular disease unlikely to heal (ABI less than 0.4, rest pain, or unoptimised tissue loss). Relative: previous ipsilateral calf surgery or trauma (distorted anatomy, higher sural nerve risk); marked obesity (BMI greater than 40); active Charcot neuroarthropathy (wait until stabilised); calf weakness from neuromuscular disease (polio, stroke, Charcot-Marie-Tooth) — further weakening is poorly tolerated. The one decision that matters — which lengthening. The contracture having been confirmed as isolated, the choice is which technique lengthens the gastrocnemius without sacrificing soleus push-off:
- Procedure
- Release of the gastrocnemius aponeurosis from the soleus fascia in the proximal-mid calf
- What is lengthened
- Gastrocnemius only — soleus preserved
- Advantages
- Most common; precise; preserves soleus push-off power; low over-lengthening risk
- Disadvantages
- Requires identification of the aponeurosis-soleus interface; sural nerve at risk in the posteromedial approach
- Procedure
- V-shaped lengthening of the conjoined gastrocnemius-soleus aponeurosis distal to the musculotendinous junction
- What is lengthened
- Gastrocnemius and some soleus
- Advantages
- Technically simpler; no need to separate gastrocnemius from soleus; shorter incision
- Disadvantages
- Lengthens some soleus fibres — less power preserved; higher over-lengthening risk than Strayer
- Procedure
- Release of the gastrocnemius from its femoral condyle origins at the distal femoral metaphysis
- What is lengthened
- Gastrocnemius only — via proximal release
- Advantages
- No calf incision; no sural nerve risk at calf level; useful in cerebral palsy
- Disadvantages
- Limited exposure; may under-correct in severe contractures; peroneal nerve at risk at the fibular neck
- Procedure
- Triple percutaneous cuts through the Achilles tendon (Hoke or White technique)
- What is lengthened
- Entire gastrocnemius-soleus-Achilles complex
- Advantages
- No open incision; fast; large correction achievable
- Disadvantages
- High wound-complication and rupture risk in diabetics; over-lengthening risk; significant push-off weakness
Special situation — diabetes. In diabetics, isolated gastrocnemius contracture raises forefoot plantar pressure by roughly 20 to 30 percent, driving recalcitrant plantar ulceration. Recession (Strayer) is strongly preferred over percutaneous TAL: it uses a proximal calf incision in better-vascularised tissue, does not violate the Achilles tendon, and avoids the 20 to 50 percent wound-breakdown rate reported with percutaneous TAL in this group. A randomised trial (Holzer, JBJS 2014) showed recession plus wound care improved ulcer healing and reduced recurrence versus wound care alone. Consent specifically for sural nerve neurapraxia (5 to 10 percent transient, less than 1 percent permanent), over-lengthening (push-off weakness, calcaneal gait), under-correction (residual equinus), wound infection (less than 2 percent) and dehiscence, DVT/PE, and the possibility of conversion to a tendo-Achilles lengthening if the recession is found intra-operatively to be insufficient.
The Operation
The goal: expose the gastrocnemius aponeurosis through a short posteromedial calf incision, identify and protect the sural nerve before any release, divide the aponeurosis from the soleus fascia incrementally while checking dorsiflexion, and stop at 5 to 10 degrees beyond neutral — lengthening the gastrocnemius while preserving the soleus. The exposure and the step-by-step release are laid out below.
Operative sequence — Strayer (posteromedial)
- Prone, padded thigh tourniquet (typically 250 mmHg); the prone position gives the most direct access to the posteromedial calf and allows gravity-assisted retraction. A supine position with a bump under the ipsilateral buttock and the leg externally rotated is acceptable but less direct.
- Palpate the gastrocnemius musculotendinous junction — a firm cord roughly 5 to 8 cm distal to the popliteal crease in the midline of the calf (about a hand's breadth below the crease). Mark a longitudinal incision centred on this point along the posteromedial border of the gastrocnemius.
- General or spinal anaesthesia; a popliteal block is an option but carries a theoretical risk of masking a postoperative tibial nerve injury. Prophylactic cefazolin 2 g IV at induction for a clean, short (15 to 25 minute) procedure.
- A 5 to 8 cm longitudinal incision along the posteromedial border of the gastrocnemius, centred on the musculotendinous junction.
- Incise skin sharply and carry through subcutaneous fat to the deep (crural) fascia of the calf.
- Keep the incision long enough for adequate visualisation — a short incision with poor exposure leads to blind cutting and nerve injury. Stay directly over the posteromedial border: not too far posterior (toward the sural nerve) and not too far medial.
- Retract the skin edges. In the subcutaneous fat, identify the sural nerve as a cord-like structure in the posterolateral portion of the wound — it can usually be palpated before it is seen, feeling like a firm strand under the fingertip.
- Place a vessel loop around it and retract it gently posterolaterally; it must remain under direct vision throughout the aponeurotic release.
- This is the single most important safety step: the sural nerve is the most commonly injured structure in this procedure.
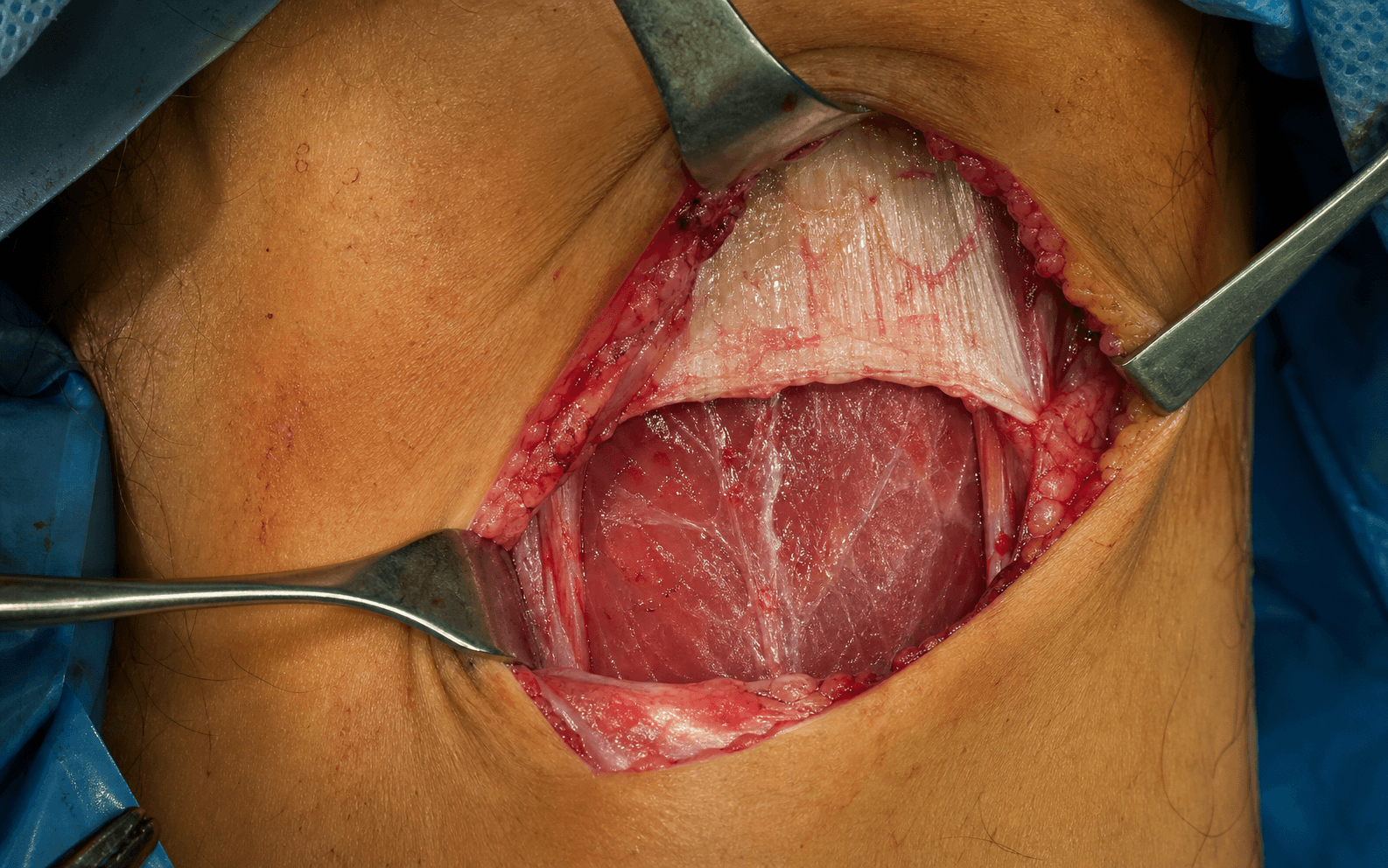
- Incise the deep fascia in line with the skin incision and retract the fascial edges to expose the gastrocnemius aponeurosis — a distinct, glistening, white fibrous layer with transversely-oriented fibres lying superficial to the soleus muscle belly.
- Identify the critical plane between the gastrocnemius aponeurosis (above, the structure to release) and the soleus fascia (below, to preserve). Do not confuse the deep fascia with the aponeurosis — the aponeurosis is deeper, thicker, and has a distinct transverse fibre pattern.
- Insert a fine elevator (Freer or Macdonald dissector) into the plane between the gastrocnemius aponeurosis and the soleus fascia and sweep from medial to lateral to develop the interval fully.
- With scissors (Metzenbaum or Mayo), divide the gastrocnemius aponeurosis transversely from medial to lateral, separating it from the soleus fascia beneath; extend the release medially and laterally across the full width of the aponeurosis.
- Release incrementally. After each increment of division, check ankle dorsiflexion with the knee extended — the endpoint is determined intra-operatively (see Step 6). Do not cut blind: visualise the full aponeurosis before each cut.
- Knee extended: target 5 to 10 degrees of dorsiflexion beyond neutral.
- Knee flexed to 90 degrees: dorsiflexion should now be approximately equal to (or slightly better than) the extended value, confirming the gastrocnemius restriction has been removed — the Silfverskiöld test is now negative.
- If dorsiflexion remains limited with the knee extended but improves with flexion, the release is incomplete — further aponeurotic division is needed. If dorsiflexion remains limited even with the knee flexed, the soleus is involved and this procedure alone will not correct it; discuss the finding and whether a concomitant TAL is indicated (ideally identified pre-operatively).
- Deflate the tourniquet and achieve haemostasis with bipolar diathermy.
- Close the deep fascia with interrupted 0 Vicryl, the subcutaneous layer with 2-0 Vicryl, and skin with a running subcuticular 3-0 Monocryl or Prolene.
- Apply a sterile dressing and a below-knee walker boot (or a short-leg posterior splint) with the ankle in neutral. The patient is allowed to bear weight as tolerated in the boot.
Identify the sural nerve in the subcutaneous fat of the posterolateral corner before opening the deep fascia; it runs roughly 1 to 2 cm posterior to the lateral fibular border in the proximal calf and may be adherent to the deep fascia in scarred tissue. Place a vessel loop, retract gently (over-retraction causes stretch injury), and keep it under direct vision throughout. Separately, stay in the plane between the gastrocnemius aponeurosis and the soleus fascia: the posterior tibial neurovascular bundle (tibial nerve, posterior tibial artery and vein) lies deep to the soleus between flexor digitorum longus and flexor hallucis longus. If exposure is inadequate, extend the incision rather than dissecting deeper.
Release the aponeurosis incrementally, checking dorsiflexion with the knee extended after each cut, and stop at 5 to 10 degrees beyond neutral. Re-check the Silfverskiöld intra-operatively: with the knee flexed, dorsiflexion should now equal (or slightly better) the extended value, confirming the gastrocnemius restriction is gone. Over-lengthening — releasing too much, or drifting into the soleus fibres — produces a calcaneal gait and loss of push-off that the patient cannot recover.
The Vulpius-Baker is a V-Y lengthening of the conjoined gastrocnemius-soleus aponeurosis (apex of the V pointing distally, advance the distal flap proximally): simpler, with no need to separate the two muscles, but it lengthens some soleus fibres, so the over-lengthening endpoint is even more critical. The Baumann releases the gastrocnemius from its femoral condyle origins through a distal-femoral incision: no calf incision and no sural nerve risk at the calf, useful in cerebral palsy and idiopathic toe-walking, but limited exposure in severe contractures and the common peroneal nerve at the fibular neck is at risk when releasing the lateral head.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation & weight-bearing | Therapy | |-------|--------|--------------------------------|---------| | 1 | 0–2 weeks | Below-knee walker boot (or posterior splint) in neutral; touch-down to partial weight-bearing | Elevation above the heart for 48 hours; paracetamol ± NSAIDs; DVT prophylaxis per protocol | | 2 | 2–4 weeks | Boot; sutures/clips out at 10–14 days | Gentle active dorsiflexion out of the boot; passive dorsiflexion within the surgical range | | 3 | 4–8 weeks | Wean the boot by 4–6 weeks into a stiff-soled shoe | Calf stretching within the corrected range; gait retraining; progressive calf strengthening | | 4 | 8–12 weeks+ | Normal footwear | Eccentric calf strengthening; sport-specific rehabilitation | Return to function: sedentary work 2–4 weeks; standing or manual work 6–8 weeks; driving 4–6 weeks (right foot; earlier for the left in an automatic); light sport at 8 weeks and full sport by 12 weeks. Maximum medical improvement — full calf strength and final dorsiflexion range — takes 6 to 12 months. Complications
- Incidence
- 5–15% transient; less than 1% permanent
- Recognition
- Numbness or dysaesthesia over the lateral foot and fifth toe; positive Tinel in the calf; burning or shooting pain
- Prevention & management
- Identify the nerve before the deep fascia; vessel loop; direct vision. Transient: observe, reassure, desensitise. Persistent beyond 3–6 months: nerve conduction studies; consider neurolysis or neuroma resection
- Incidence
- less than 5%
- Recognition
- Dorsiflexion greater than 15 degrees beyond neutral; calcaneal gait; unable to single-leg heel rise; push-off weakness
- Prevention & management
- Incremental release with intra-operative dorsiflexion check; stop at 5–10 degrees. Mild: calf strengthening, heel-lift. Severe with functional deficit: rare Achilles reconstruction
- Incidence
- 3–8%
- Recognition
- Persistent limited dorsiflexion with the knee extended despite surgery; no symptom improvement
- Prevention & management
- Adequate pre-operative Silfverskiöld; incremental release; do not stop early. Revision recession if Silfverskiöld positive; TAL if the soleus is involved
- Incidence
- 1–3%
- Recognition
- Erythema, warmth, swelling, purulent discharge; fever; raised inflammatory markers
- Prevention & management
- Single-dose prophylactic antibiotics; sterile technique; haemostasis; layered closure. Superficial: swab, oral antibiotics. Deep: washout, IV antibiotics, VAC
- Incidence
- 1–2%
- Recognition
- Separation of wound edges; exposed fascia or aponeurosis; serous or serosanguinous discharge
- Prevention & management
- Layered closure without tension; boot protection 2–4 weeks. Small: conservative (dressing, secondary intention). Large or deep: return to theatre
- Incidence
- 2–5% temporary
- Recognition
- Reduced single-leg heel-rise height; difficulty uphill or on stairs; reduced concentric plantar-flexion power
- Prevention & management
- Preserve soleus (Strayer); avoid over-lengthening. Calf and eccentric strengthening, heel-lift; most recover by 6–12 months
- Incidence
- 2–5%
- Recognition
- Return of limited dorsiflexion months to years later; recurrence of original symptoms
- Prevention & management
- Adequate initial release; post-operative stretching. Revision recession if Silfverskiöld positive; TAL if the soleus is now involved
- Incidence
- less than 1% with prophylaxis
- Recognition
- Calf swelling, tenderness, warmth (DVT); dyspnoea, pleuritic chest pain, tachycardia (PE)
- Prevention & management
- Chemical prophylaxis (LMWH or aspirin) per protocol; early mobilisation; pneumatic compression. Standard DVT/PE treatment
Viva & Exam Focus
SILFVERSILFVER — gastrocnemius recession decision-making
STRAYERSTRAYER — operative technique steps
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old woman has 18 months of recalcitrant plantar fasciitis despite structured physiotherapy, custom orthotics, two corticosteroid injections and a night splint. She has tenderness at the plantar medial calcaneal tuberosity and a positive Silfverskiöld test — dorsiflexion improving from 0 degrees (knee extended) to 10 degrees (knee flexed). How would you manage her?”
“A 65-year-old man with Type 2 diabetes (HbA1c 7.8%) has a recurrent plantar forefoot ulcer beneath the second metatarsal head that has failed to heal after 4 months of total contact casting and offloading. He has a positive Silfverskiöld test and asks whether surgery can help his ulcer heal. How do you counsel him?”
“A 40-year-old runner has 10 months of non-insertional Achilles tendinopathy that has not responded to an eccentric calf strengthening programme, activity modification and one PRP injection. There is a palpable tender nodular swelling in the mid-substance of the Achilles, 6 cm proximal to the calcaneal insertion. Dorsiflexion is 5 degrees (knee extended) and improves to 15 degrees (knee flexed). What would you do?”
The decision (Silfverskiöld gatekeeper)
- Positive test (dorsiflexion improves with knee flexed) equals isolated gastrocnemius contracture equals recession
- Negative test (no improvement) equals soleus or Achilles contracture equals TAL, NOT recession
- Normal ankle dorsiflexion is at least 10 degrees beyond neutral with the knee extended
- Gastrocnemius contracture contributes to plantar fasciitis, metatarsalgia, midfoot overload, Achilles tendinopathy, diabetic ulceration, flatfoot
- Always confirm a positive test before planning a recession
Surgical anatomy
- Gastrocnemius: bi-articular (knee and ankle), two heads from posterior femoral condyles — tight with the knee extended
- Soleus: uni-articular (ankle only), from posterior tibia and proximal fibula — NOT affected by knee position
- Gastrocnemius aponeurosis: white, glistening, transverse fibres at the proximal-mid calf — released in the Strayer
- Soleus fascia: thin layer over the soleus — the floor of the release, preserved
- Sural nerve: posterolateral subcutaneous tissue, about 1 to 2 cm posterior to the fibula — primary danger structure
Technique comparison
- Strayer: release gastrocnemius aponeurosis from soleus fascia — most common; gastrocnemius only; preserves soleus
- Vulpius-Baker: V-Y of the conjoined aponeurosis — simpler but lengthens some soleus; higher over-lengthening risk
- Baumann: proximal release from the femoral condyles — no calf incision; useful in children; peroneal nerve at risk
- Percutaneous TAL: triple-cut Achilles — for combined contracture; high wound risk in diabetics
Strayer — key steps
- 1. Prone, thigh tourniquet; posteromedial incision on the musculotendinous junction (5 to 8 cm distal to the popliteal crease)
- 2. Identify the sural nerve in the posterolateral subcutaneous fat — vessel loop and protect
- 3. Open the deep fascia; identify the gastrocnemius aponeurosis and soleus fascia beneath
- 4. Develop the plane between them with a Freer dissector
- 5. Release the aponeurosis incrementally with scissors — check dorsiflexion after each cut
- 6. Stop at 5 to 10 degrees beyond neutral with the knee extended; Silfverskiöld now negative
- 7. Deflate the tourniquet, haemostasis, layered closure, walker boot
Danger zones
- Sural nerve: 5 to 15 percent transient neurapraxia — identify before the deep fascia
- Over-lengthening: push-off weakness, calcaneal gait — incremental release with intra-operative check
- Under-correction: residual equinus — adequate release and intra-operative verification
- Posterior tibial bundle (deep to soleus, between FDL and FHL) — stay above the soleus fascia
- Common peroneal nerve at the fibular neck — at risk only in the Baumann proximal release
Complications
- Sural nerve neurapraxia: 5 to 15 percent transient, less than 1 percent permanent
- Over-lengthening: less than 5 percent; calf strengthening and heel-lift; rare surgical revision
- Under-correction: 3 to 8 percent; revision recession if Silfverskiöld positive, TAL if soleus involved
- Wound infection: 1 to 3 percent; oral antibiotics or washout
- DVT/PE: less than 1 percent with prophylaxis (LMWH or aspirin)
Rehabilitation
- Walker boot 2 to 4 weeks; touch-down to partial weight-bearing initially
- Gentle active dorsiflexion from day 1; calf stretching from week 2
- Boot weaned by week 4 to 6; normal footwear by week 6 to 8
- Eccentric calf strengthening from week 6 to 8; sport-specific rehab from week 8 to 12
- Return: sedentary 2 to 4 weeks, manual 6 to 8 weeks, full sport 8 to 12 weeks
Special cases
- Diabetes: recession (NOT TAL) for recalcitrant forefoot ulceration with positive Silfverskiöld — Holzer RCT supports healing; TAL wound rate 20 to 50 percent
- Plantar fasciitis: recession as an adjunct to plantar fascia release when gastrocnemius tightness is present
- Flatfoot: recession as an adjunct to flatfoot reconstruction — gastrocnemius contracture is commonly present
- Paediatrics: Baumann (proximal release) preferred in children; high success in cerebral palsy and idiopathic toe-walking
- Achilles tendinopathy: recession reduces biomechanical load; confirm an adequate eccentric programme first
Background & Evidence
Pathoanatomy. The triceps surae has three heads. The gastrocnemius is bi-articular: its medial head arises from the posterior medial femoral condyle and the posterior knee capsule, its lateral head from the lateral condyle and the supracondylar line — so it crosses both the knee and the ankle and is tightened by knee extension. The soleus is uni-articular, arising from the posterior tibia (soleal line) and the fibular head and proximal fibula, crossing only the ankle and unaffected by knee position. The two merge into a common aponeurosis in the distal calf to form the tendo-Achilles, inserting on the posterior calcaneal tuberosity. The gastrocnemius bellies converge on a thick, glistening, white, transversely-fibred aponeurosis at the junction of the proximal and middle thirds of the calf, which sits on — and can be separated from — the thinner soleus fascia beneath; that interval is the plane of the Strayer release. The gastrocnemius musculotendinous junction lies in the proximal third of the calf, roughly 5 to 8 cm distal to the popliteal crease, marking the level of the incision. Structures at risk. The sural nerve — formed from the medial sural cutaneous nerve (tibial) and the sural communicating branch (common peroneal) — descends in the subcutaneous tissue of the posterolateral calf about 1 to 2 cm posterior to the lateral fibular border, then passes behind the lateral malleolus to supply the lateral foot and fifth toe; it is the most commonly injured structure and the reason identification before deep dissection is mandatory. The posterior tibial neurovascular bundle (tibial nerve, posterior tibial artery and vein) lies deep to the soleus between flexor digitorum longus and flexor hallucis longus — safe as long as the dissection stays superficial to the soleus fascia. The common peroneal nerve at the fibular neck is at risk only in the Baumann proximal release. The Silfverskiöld test — biomechanics. Because the gastrocnemius crosses both joints and the soleus only the ankle, a contracted gastrocnemius limits dorsiflexion with the knee extended (gastrocnemius at maximum length). Flexing the knee slackens the gastrocnemius: if dorsiflexion then improves, the gastrocnemius is the tight structure (positive); if it does not, the soleus or tendo-Achilles is tight (negative). Stabilise the hindfoot in subtalar neutral, measure dorsiflexion with the knee extended and then flexed to 90 degrees, and compare.
- Finding
- Dorsiflexion limited with the knee extended but improves by at least 5 degrees with the knee flexed to 90 degrees
- Meaning
- Isolated gastrocnemius contracture — recession is the correct operation
- Finding
- Dorsiflexion limited equally with the knee extended and flexed
- Meaning
- Combined gastrocnemius-soleus or Achilles contracture — recession under-corrects; a TAL is required
Key evidence. The evidence supports recession when an isolated gastrocnemius contracture is confirmed. DiGiovanni (2002) established that isolated gastrocnemius tightness is significantly more common in patients with plantar fasciitis, metatarsalgia and forefoot overload than in controls — the biomechanical rationale. Maskill (2010) reported 93 percent satisfaction in 29 patients with isolated foot pain and a positive Silfverskiöld test. Kiewiet (2013) showed improved pain and function after recession for chronic non-insertional Achilles tendinopathy. The highest-level support is Molund (2018), a Level I randomised controlled trial in which proximal medial gastrocnemius recession plus stretching outperformed stretching alone for chronic plantar heel pain, with benefit sustained at 6 years. In diabetics with recalcitrant forefoot ulceration, Holzer's randomised trial showed recession plus wound care improved healing and reduced recurrence versus wound care alone.
References
Isolated gastrocnemius tightness
Prospective comparative study establishing that isolated gastrocnemius tightness is significantly more common in patients with plantar fasciitis, metatarsalgia and forefoot overload than in controls — the biomechanical rationale for addressing the equinus contributor rather than the symptom alone. doi: 10.2106/00004623-200206000-00010.
Gastrocnemius recession to treat isolated foot pain
Retrospective series of 29 patients with isolated foot pain and a positive Silfverskiöld test refractory to non-operative care: 93 percent satisfaction, 92 percent would undergo it again, with one transient sural neurapraxia that resolved. doi: 10.3113/FAI.2010.0019.
Gastrocnemius recession for chronic noninsertional Achilles tendinopathy
Case series of 8 patients with chronic non-insertional Achilles tendinopathy and a positive Silfverskiöld test: significant improvement in pain and function after isolated recession, with no over-lengthening or significant calf weakness. doi: 10.1177/1071100713477620.
Surgical anatomy of the gastrocnemius recession (Strayer procedure)
Cadaveric anatomic study defining the sural nerve's course and the zone of greatest risk in the proximal third of the posteromedial calf incision — the basis for systematic nerve identification before release. doi: 10.1177/107110070402500409.
Proximal medial gastrocnemius recession and stretching versus stretching for chronic plantar heel pain
Level I randomised controlled trial showing proximal medial gastrocnemius recession plus stretching gave significantly better pain relief and function than stretching alone for chronic plantar heel pain at minimum 2 years, with benefit sustained at 6 years — the highest-level evidence supporting recession for recalcitrant plantar fasciitis. doi: 10.1177/1071100718794659.