Metal-on-metal hip resurfacing via the posterior approach · advanced
- Patient selection is the dominant predictor of outcome — young high-demand males with large femoral heads (greater than 50 mm) and good bone stock achieve the best survivorship; women, small components (less than 46 mm), renal impairment and known metal hypersensitivity are now considered absolute or strong relative contraindications in most centres.
- Femoral neck fracture (1-4 percent) and adverse reaction to metal debris (ARMD) with pseudotumour formation are the two dominant failure modes. Both are technique-dependent: meticulous preservation of the retinacular vessels during femoral head exposure and cylindrical reaming is mandatory to avoid osteonecrosis and neck fracture.
- The posterior approach provides excellent acetabular exposure and allows direct visualisation of the retinacular vessels on the posterior femoral neck — the vessels must be identified, protected and kept continuously moist throughout the procedure.
- Modern metal-on-metal hip resurfacing has fallen sharply from favour following regulatory warnings (MHRA, FDA) and registry data showing inferior survivorship compared with conventional THA in women and smaller heads; metal ion surveillance (cobalt and chromium) and cross-sectional imaging (MARS MRI or ultrasound) remain mandatory for all patients with MoM bearings.
- “The retinacular vessels enter the femoral head at the head-neck junction posteriorly and laterally — any circumferential dissection or aggressive retraction that strips these vessels risks AVN and subsequent neck fracture.
- “Femoral component cement mantle should be 1 mm thick with pressurisation; inadequate cement technique or varus malposition of the femoral component (greater than 5 degrees) dramatically increases neck fracture risk.
- “Women of childbearing age are contraindicated because of theoretical transplacental metal ion transfer and unknown long-term effects on the foetus; serum ion levels must be documented before considering any MoM implant in a woman.
- “Registry data (NJR, AOANJRR) consistently show 10-year revision rates for hip resurfacing of 10-15 percent in women versus 4-6 percent in men with large heads — this gender disparity is the primary reason many centres have abandoned the procedure in females.
When & Why
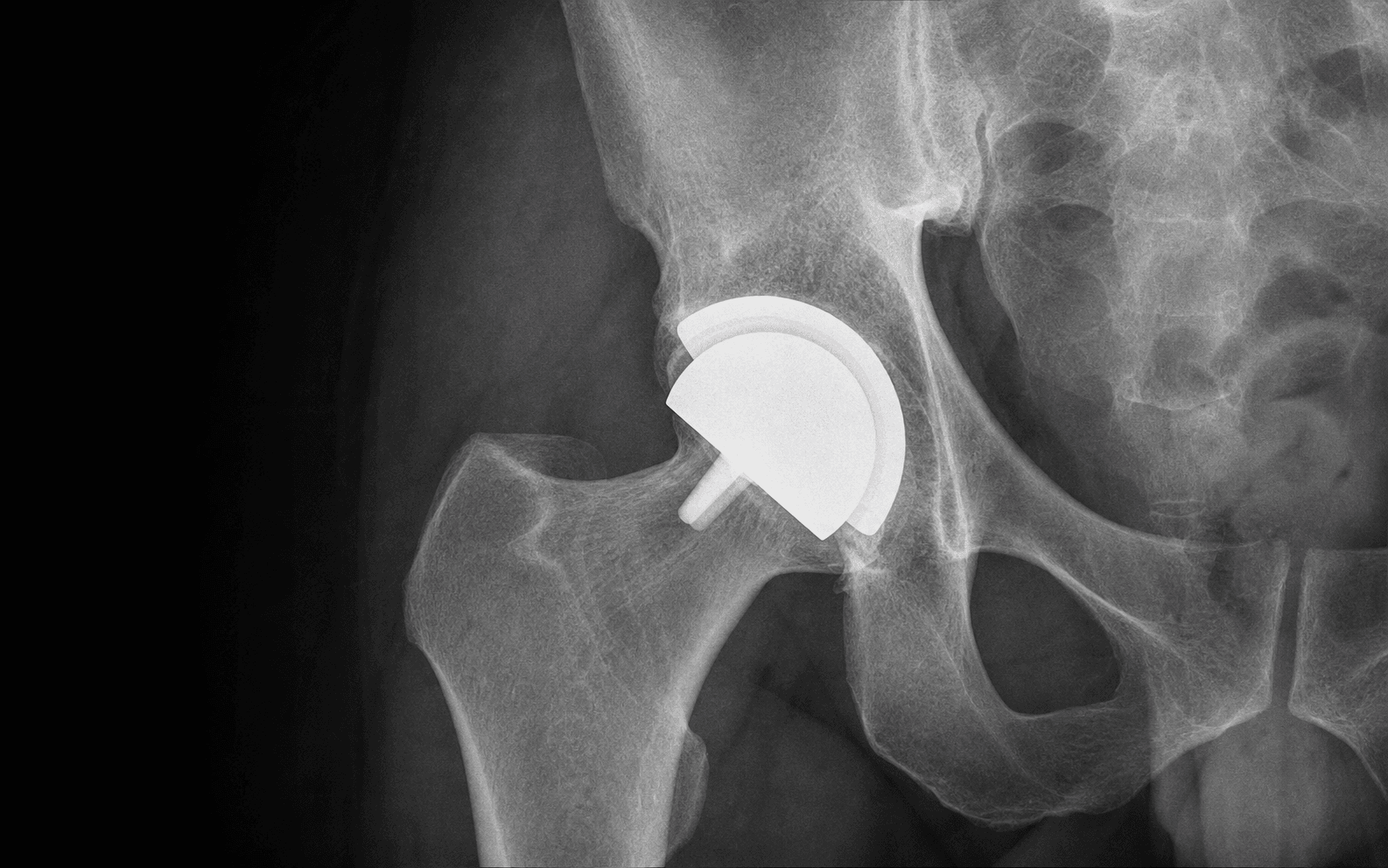
Hip resurfacing preserves the femoral neck and caps the native head with a metal shell, paired with a metal acetabular component — a bone-preserving, large-diameter metal-on-metal (MoM) bearing. Its only modern role is in a narrow, carefully selected population: young, high-demand men with large femoral heads and good bone stock, where it can match conventional total hip arthroplasty (THA) for survivorship while preserving bone and lowering dislocation risk. Outside that group the failure rate rises steeply, so selection IS the operation.
- Ideal candidate
- Male
- Contraindicated
- Female (most centres)
- Ideal candidate
- Greater than 50 mm on AP pelvis
- Contraindicated
- Less than 46 mm
- Ideal candidate
- 40-55 years, high demand (manual labour, sport)
- Contraindicated
- Not age-based alone
- Ideal candidate
- Good stock; no cysts greater than 1 cm; no osteopenia
- Contraindicated
- Severe head deformity or large cysts compromising fixation
- Ideal candidate
- eGFR greater than 60 mL/min
- Contraindicated
- eGFR less than 60 mL/min or dialysis
- Ideal candidate
- None on history or testing
- Contraindicated
- Known or suspected metal hypersensitivity
- Ideal candidate
- Not applicable
- Contraindicated
- Pregnancy or planning pregnancy
- Ideal candidate
- Primary OA, or post-traumatic with preserved head shape
- Contraindicated
- Active infection or tumour
Accepted but higher-risk indications (registry survivorship acceptable but inferior to the ideal group): - Male with head size 46-50 mm
- Avascular necrosis, Ficat stage II-III with greater than 50 percent head involvement (requires careful femoral head assessment)
- Developmental dysplasia with adequate bone stock after acetabular reaming Relative contraindications: - Acetabular dysplasia requiring structural graft
- Inflammatory arthritis with poor bone quality
- Previous pelvic irradiation
- Morbid obesity (BMI greater than 35) — technical exposure and component positioning difficulties Consent specifically for femoral neck fracture (1-4 percent), ARMD and pseudotumour (3-8 percent at 10 years), metal ion elevation requiring lifelong surveillance, dislocation (less than 1 percent with posterior repair), leg-length discrepancy, infection, and the regulatory history (MHRA, FDA) of MoM bearings.
The Operation
The goal: resurface — not replace — the femoral head through a posterior approach, protecting the retinacular vessels at every step, placing the femoral component in slight valgus with a thin cement mantle, and seating a well-positioned acetabular component, then repairing the posterior soft-tissue sleeve. The exposure (positioning through to capsulotomy and vessel identification) is laid out in full as the first steps below, and in depth on the posterior (Moore/Southern) approach to the hip page.
Operative sequence
- Lateral decubitus on a radiolucent table, operative hip flexed 30 degrees and internally rotated 20 degrees; pelvis stabilised with pubic and sacral supports. Prep and drape the entire limb free for intraoperative positioning and image-intensifier access.
- Hypotensive anaesthesia (mean arterial pressure 60-70 mmHg) reduces bleeding. Tranexamic acid 1 g IV at induction and 1 g at closure is standard.
- Equipment: image intensifier, radiolucent table, resurfacing instrumentation (cylindrical reamers, femoral head trials, cement pressuriser), acetabular reamers, trial components and a high-speed burr.
- Mark the greater trochanter and the posterior border of the femur — the posterior border of the greater trochanter is the key landmark for the skin incision.
- Incise 12-15 cm centred over the greater trochanter, curving slightly posteriorly proximally. Divide the fascia lata in line with the skin.
- Identify the gluteus maximus tendon insertion on the posterior femur and partially release it from the linea aspera to allow anterior retraction of the muscle belly.
- Internally rotate the hip to bring the external rotators into tension, then develop the interval between gluteus medius and piriformis. This is the internervous plane: gluteus medius (superior gluteal nerve) versus the short external rotators (inferior gluteal and sciatic nerves).
- Identify the sciatic nerve — it lies 2-3 cm medial to the posterior acetabular rim and is protected by the external rotators until they are divided; protect it with a blunt retractor.
- Tag and divide the short external rotators (piriformis, obturator internus, gemelli) 1 cm from their insertion, leaving a cuff for later repair. Release quadratus femoris partially only if more exposure is required.
- Perform a Z-shaped capsulotomy: the superior limb runs along the acetabular rim, the vertical limb along the posterior neck, and the inferior limb along the intertrochanteric line.
- Identify the retinacular vessels on the posterior femoral neck, lying under the reflected external rotator tendons. These vessels arise from the medial femoral circumflex artery and enter the head at the head-neck junction, predominantly posteriorly and laterally — deep to the external rotator tendons and the posterior capsule.
- Place moist saline-soaked swabs over the vessels and protect them throughout. Never dissect circumferentially around the neck, and limit the anterior capsular release to what is strictly necessary — stripping or stretching these vessels risks osteonecrosis and subsequent neck fracture.
- Dislocate the hip by flexing, adducting and internally rotating.
- Assess femoral head size, shape, bone quality and the presence of cysts. Measure the head diameter with callipers — heads less than 46 mm are generally abandoned in favour of conventional stemmed THA.
- Identify the head-neck junction and mark the planned resection level. The lateral neck cortex must remain at least 2 mm thick after reaming.
- Place the femoral neck guide pin under direct vision, aiming for slight valgus (5-10 degrees relative to the native neck-shaft angle) and neutral version. Confirm position with the image intensifier.
- Use sequential cylindrical reamers to prepare the head, maintaining at least 2 mm of bone circumferentially around the reamed cylinder. The reamer stops at the head-neck junction; do not notch the neck laterally.
- Deliver the acetabulum with a posterior retractor on the ischium and an anterior retractor on the anterior rim. Excise the labrum and any osteophytes.
- Ream sequentially to the planned size, using the transverse acetabular ligament as the inferior landmark (it defines native version, approximately 15-20 degrees anteversion) and the posterior rim for inclination. The anterior rim confirms version; over-reaming anteriorly risks iliopsoas impingement.
- Target 40-50 degrees inclination and 15-25 degrees anteversion. Under-ream by 1-2 mm for press-fit; supplemental screws are rarely required.
- Impact the acetabular component into the reamed socket and confirm seating with the image intensifier.
- The component should sit flush with the rim without medialisation beyond the medial wall. Re-check version against the transverse acetabular ligament.
- Clean the reamed femoral head with pulsatile lavage and dry it thoroughly.
- Apply cement to the component and the head, pressurise with a cement gun and pressuriser, and seat the component, aiming for a 1 mm cement mantle. Maintain pressure until the cement has cured.
- Remove excess cement from the head-neck junction and confirm final position with the image intensifier.
- Reduce the hip and assess stability through a full range of motion.
- Check for impingement, leg length and offset. Perform a shuck test and assess both anterior and posterior stability.
- Repair the posterior capsule with heavy absorbable suture, then repair the external rotators back to the greater trochanter cuff.
- Close the fascia lata, subcutaneous tissue and skin, and apply a compressive dressing. No drain is routinely used.
The retinacular vessels from the medial femoral circumflex artery are the sole blood supply to the resurfaced femoral head. Identify them on the posterior neck immediately after the Z-shaped capsulotomy and cover them with moist saline-soaked swabs before any retractor is placed on the posterior neck. Never allow them to dry out. Three things destroy them: direct retraction on the unprotected vessels, over-release of the anterior capsule (which stretches and tears them), and circumferential dissection around the neck. Sciatic nerve injury is the other danger at this stage — avoid excessive medial retraction before the external rotators are divided.
Use the lateral cortex of the femoral neck as the reference for version. Ream to a planned 1 mm cement mantle, then seat the trial component. If the trial sits in varus or the neck is notched, abandon resurfacing and convert to a stemmed THA — bring the image intensifier in before cementing to confirm neutral-to-valgus alignment.
Varus malposition greater than 5 degrees and lateral neck notching are the two strongest technical predictors of femoral neck fracture. If either is present after reaming, resurfacing must be abandoned in favour of a conventional stemmed THA — the acetabular component can be implanted as planned and a cemented or uncemented stem used. Attempting to "correct" the position with further reaming only weakens the neck further.
Aftercare & Complications
Rehabilitation | Phase | Timing | Weight-bearing and motion | Surveillance | |-------|--------|---------------------------|--------------| | Immediate | 0-2 weeks | Weight-bearing as tolerated, crutches 4-6 weeks; hip precautions 6 weeks (no flexion greater than 90 degrees, no adduction, no internal rotation beyond neutral) | Wound review at 10-14 days; chemical VTE prophylaxis for 28 days (LMWH or DOAC) | | Early | 0-6 weeks | Protected weight-bearing, gentle ROM, abductor strengthening | — | | Progression | 6-12 weeks | Progress to full weight-bearing, gait normalisation, resistance exercises | — | | Return | 3-6 months | Low-impact sport (swimming, cycling); high-impact deferred to 6 months | Metal ions at 6 months and 1 year, then annually; MARS MRI at 1 year, then every 2 years (or sooner if ions rise) | Return to activity: driving at 6-8 weeks (when safe to perform an emergency stop), office work at 4-6 weeks, manual labour at 3-6 months. Low-impact sport resumes at about 3 months; high-impact contact sport is generally discouraged with MoM bearings. Complications
- Incidence
- 1-4 percent overall; higher with varus malposition or neck notching
- Recognition
- Sudden groin or thigh pain, usually within 6 months; radiographic head collapse with varus displacement of the component
- Prevention and management
- Prevention: slight valgus (5-10 degrees), maintain 2 mm neck bone stock, protect retinacular vessels, image intensifier before cementing. Management: most require revision to stemmed THA; undisplaced fractures in good bone stock may be fixed with cannulated screws if recognised early
- Incidence
- 3-8 percent at 10 years; higher in women and small heads
- Recognition
- Groin pain, swelling, limp; elevated cobalt and chromium (greater than 7 ppb); MARS MRI shows fluid collection or mass with lymphocyte infiltrate on histology
- Prevention and management
- Prevention: correct component position (inclination 40-50 degrees, anteversion 15-25 degrees), annual metal ion surveillance, early cross-sectional imaging. Management: revision to non-MoM bearing (ceramic-on-polyethylene preferred); excise pseudotumour and necrotic tissue; single- or two-stage depending on soft-tissue destruction
- Incidence
- Up to 15 percent of patients at 5 years
- Recognition
- Asymptomatic rise in cobalt or chromium on routine surveillance; normal cross-sectional imaging
- Prevention and management
- Prevention: none specific. Management: continue annual surveillance; if ions keep rising or symptoms develop, consider revision even if imaging is normal
- Incidence
- Less than 1 percent when retinacular vessels protected
- Recognition
- Gradual groin pain 6-24 months post-operatively; radiographic sclerosis and head collapse; MRI shows a necrotic segment
- Prevention and management
- Prevention: meticulous vessel protection, limit anterior capsular release, avoid circumferential neck dissection. Management: early cases observed; progressive collapse requires revision to THA
- Incidence
- Acetabular inclination greater than 55 degrees in 5-10 percent of early series
- Recognition
- Edge loading on radiographs, accelerated wear, rising metal ions, ARMD on MRI
- Prevention and management
- Prevention: transverse acetabular ligament and posterior rim landmarks; image intensifier confirmation. Management: revision if symptomatic or ions rising; asymptomatic malposition with normal ions observed with closer surveillance
- Incidence
- Less than 1 percent with posterior repair
- Recognition
- Posterior dislocation with leg shortening and external rotation
- Prevention and management
- Prevention: meticulous posterior capsule and external rotator repair; avoid excessive acetabular anteversion. Management: closed reduction under sedation; revision if recurrent or if component malposition is the cause
- Incidence
- Less than 1 percent
- Recognition
- Pain, swelling, sinus, elevated CRP and ESR; aspiration positive for organism
- Prevention and management
- Prevention: standard perioperative antibiotics, laminar flow, meticulous haemostasis. Management: debridement and implant retention if acute; two-stage revision if chronic
Special case: conversion of a failed resurfacing to THA Indications for conversion include femoral neck fracture, progressive ARMD with soft-tissue destruction, aseptic loosening of either component, and recurrent dislocation. Technical points: the acetabular component is usually well-fixed and can be retained if position is acceptable, otherwise it is revised; the femoral side typically needs a cemented or uncemented stemmed component; ARMD soft-tissue destruction may demand extensive debridement with abductor insufficiency as a common sequela; and the bearing is changed to ceramic-on-polyethylene or ceramic-on-ceramic. Outcomes after conversion are worse than primary THA — higher dislocation and infection rates and inferior patient-reported outcomes, reflecting the soft-tissue damage from ARMD.
Viva & Exam Focus
RESURFACERESURFACE — patient selection and contraindications
POSTERIORPOSTERIOR — key technical principles
The trap. Treating femoral head exposure like a standard THA femoral preparation — aggressive circumferential capsular release or excessive retraction strips the retinacular vessels that supply the femoral head. The fix. Identify the posterior retinacular vessels under the reflected external rotator tendons before any capsular incision. Keep them continuously moist with saline-soaked swabs. Limit anterior and medial capsular release to what is strictly necessary for acetabular exposure, and never place retractors directly on the posterior neck without protecting the vessels.
Location and mechanism. The femoral neck is at greatest risk during cylindrical reaming if the component is placed in varus (greater than 5 degrees) or if the reamer removes excessive bone laterally, thinning the neck. Prevention. Use the lateral femoral neck as the reference for component version and inclination. Maintain at least 2 mm of bone circumferentially around the reamed cylinder, and confirm with the image intensifier before cementing. Varus malposition is the most common technical error leading to fracture.
Pathophysiology. Adverse reaction to metal debris produces a lymphocyte-dominated inflammatory response with tissue necrosis, fluid collections and pseudotumour masses that can compress neurovascular structures or erode bone. Risk factors. Female sex, small head size (less than 46 mm), malpositioned components (acetabular inclination greater than 55 degrees or anteversion outside 10-25 degrees), and elevated metal ions (cobalt or chromium greater than 7 ppb). Surveillance. All MoM patients need annual metal ion testing and cross-sectional imaging (MARS MRI preferred) even if asymptomatic. Early detection allows revision before catastrophic soft-tissue destruction.
Safe zone. Acetabular inclination 40-50 degrees, anteversion 15-25 degrees — a target within the Lewinnek zone, which is 15 ± 10 degrees (5-25). Inclination greater than 55 degrees dramatically increases edge loading, wear and ARMD risk. Technique. Use the transverse acetabular ligament and posterior rim as landmarks. Avoid over-reaming medially, which medialises the centre of rotation and increases joint reaction forces. Press-fit with 1-2 mm under-reaming is standard; supplemental screws are rarely required with modern designs.
Contraindications. Known metal allergy (positive patch testing or lymphocyte transformation test), renal impairment (eGFR less than 60 mL/min) and any patient on dialysis. Metal ions are cleared by the kidneys; impaired clearance leads to systemic accumulation. Pre-operative screening. Document renal function and consider an alternative bearing surface (ceramic-on-polyethylene or ceramic-on-ceramic) in any patient with borderline renal function or a history of metal sensitivity.
Absolute contraindication in most guidelines. Transplacental transfer of cobalt and chromium ions has been documented, and long-term effects on the foetus are unknown. Serum ion levels must be normal before any MoM implant is considered. Registry and regulatory position. Both MHRA and FDA advise against MoM resurfacing in women. Many centres have abandoned the procedure entirely in females regardless of age.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 48-year-old male manual labourer with primary osteoarthritis of the right hip is referred for consideration of hip resurfacing. His femoral head measures 54 mm on the AP pelvis radiograph. He has no medical comorbidities and normal renal function. How do you counsel him and what is your operative plan?”
“You are performing a hip resurfacing via the posterior approach. After cylindrical reaming of the femoral head you notice that the trial component sits in 7 degrees of varus relative to the native neck-shaft angle and the lateral neck cortex has been notched by the reamer. What do you do?”
“A 52-year-old woman who underwent hip resurfacing 7 years ago presents with new-onset groin pain and a limp. Serum cobalt is 12 ppb and chromium is 11 ppb. MARS MRI demonstrates a 4 cm pseudotumour with surrounding muscle oedema and partial abductor detachment. What is your management?”
Patient selection
- Ideal: male, age 40-55, head greater than 50 mm, high demand, good bone stock, normal renal function — 10-year survivorship 88-93 percent
- Contraindicated: female sex, head less than 46 mm, renal impairment (eGFR less than 60), metal hypersensitivity, pregnancy or planned pregnancy
- Registry data show women have 2-3 times higher revision risk than men; small heads have 4-5 times higher risk
- Baseline metal ions, renal function and hypersensitivity screening are mandatory before any MoM implant
Critical surgical anatomy
- Retinacular vessels from the medial femoral circumflex artery enter the head at the posterior head-neck junction — must be identified and protected with moist swabs
- Posterior approach allows direct visualisation of the vessels; anterior capsular release must be minimal to avoid vessel stretch
- Transverse acetabular ligament defines the inferior limit and version (15-20 degrees anteversion)
- Posterior acetabular rim is the primary inclination landmark (target 40-50 degrees)
Operative technique — key steps
- Lateral position, hip flexed 30 degrees and internally rotated 20 degrees; radiolucent table for image intensifier
- Z-shaped posterior capsulotomy; identify retinacular vessels immediately and protect throughout
- Cylindrical reaming with 5-10 degrees valgus; maintain 2 mm neck bone stock; no lateral notching
- Acetabular reaming to 40-50 degrees inclination, 15-25 degrees anteversion using transverse ligament and posterior rim
- Cemented femoral component with 1 mm mantle and pressurisation; image intensifier confirmation before cementing
- Posterior capsule and external rotator repair reduces dislocation risk to less than 1 percent
Dominant complications and surveillance
- Femoral neck fracture (1-4 percent): varus malposition and neck notching are the strongest predictors; most require revision to THA
- ARMD and pseudotumour (3-8 percent at 10 years): higher in women and small heads; acetabular inclination greater than 55 degrees is the dominant driver
- Metal ion elevation: cobalt or chromium greater than 7 ppb predicts ARMD; annual testing mandatory for all MoM patients
- MARS MRI or ultrasound: cross-sectional imaging required annually or biennially even if asymptomatic
- Regulatory position: MHRA and FDA advise against MoM resurfacing in women; many centres have abandoned the procedure in females
Post-operative protocol
- Weight-bearing as tolerated from day of surgery; crutches 4-6 weeks; hip precautions 6 weeks
- Metal ion testing at 6 months, 1 year, then annually; MARS MRI at 1 year then every 2 years
- Return to low-impact sport at 3 months; high-impact sport generally discouraged
- Conversion to THA after failed resurfacing has higher complication rates than primary THA, especially dislocation and infection
Viva essentials
- Patient selection is the single most important determinant of outcome — know the ideal candidate and absolute contraindications
- Retinacular vessel preservation is the technical step that directly prevents AVN and neck fracture
- Component position targets: femoral 5-10 degrees valgus; acetabular 40-50 degrees inclination, 15-25 degrees anteversion
- Surveillance protocol: annual ions plus periodic cross-sectional imaging for life
- ARMD revision requires bearing change to non-MoM and extensive soft-tissue debridement; outcomes are inferior to primary THA
Background & Evidence
Why metal-on-metal resurfacing, and why it fell from favour. Hip resurfacing was introduced in the 1990s with the promise of bone preservation, improved proprioception and a lower dislocation risk than conventional THA, thanks to the large-diameter bearing. Early enthusiasm was tempered by registry data showing higher revision rates than conventional THA, particularly in women and with smaller components. The 2010-2012 regulatory warnings (MHRA, FDA) and the subsequent decline in use reflect these findings — modern practice confines resurfacing to a narrow population of young, high-demand men with large heads.
- Resurfacing 10-yr survival
- 88-93 percent
- THA 10-yr survival
- 94-97 percent
- Dominant failure mode
- Neck fracture 1-3 percent, ARMD 2-4 percent
- Resurfacing 10-yr survival
- 70-78 percent
- THA 10-yr survival
- 93-96 percent
- Dominant failure mode
- ARMD and pseudotumour 8-15 percent
- Resurfacing 10-yr survival
- 65-75 percent
- THA 10-yr survival
- 93-96 percent
- Dominant failure mode
- ARMD 12-20 percent
- Resurfacing 10-yr survival
- 82-87 percent
- THA 10-yr survival
- 94-96 percent
- Dominant failure mode
- ARMD 5-8 percent, neck fracture 2-4 percent
The consistent message across registries (NJR, AOANJRR) is that patient selection governs outcome: in the ideal male, large-head cohort, resurfacing approaches the survivorship of conventional THA; in women and small heads the revision rate is two to four times higher, driven by ARMD. This gender and head-size disparity — together with the burden of lifelong metal ion surveillance — is why most centres have abandoned the procedure outside its narrow indication.
References
Failure rates of metal-on-metal hip resurfacings: analysis of data from the National Joint Registry for England and Wales
- Meta-analysis of 12 national registries, 285 000 hip resurfacing procedures
- 10-year revision rate 12.6 percent for resurfacing versus 5.7 percent for cemented THA
- Women had 2.4 times higher revision risk than men; head size less than 46 mm carried 4.7 times higher risk
Early failure of metal-on-metal bearings in hip resurfacing and large-diameter total hip replacement: a consequence of excess wear
- Prospective cohort of 660 MoM resurfacings; 26 patients developed ARMD requiring revision
- Acetabular inclination greater than 55 degrees and elevated cobalt greater than 7 ppb predicted ARMD
- MARS MRI demonstrated pseudotumours in 80 percent of symptomatic patients with elevated ions
Results of Birmingham hip resurfacing at 12 to 15 years: a single-surgeon series
- Prospective single-surgeon series of 1000 BHR implants in patients under 55 years
- 10-year survivorship 95.8 percent in males with head greater than 50 mm; 84.6 percent in females
- No cases of femoral neck fracture in the male large-head cohort when a strict vessel-preservation protocol was followed
Is the survivorship of Birmingham hip resurfacing better than selected conventional hip arthroplasties in men younger than 65 years of age? A study from the Australian Orthopaedic Association National Joint Replacement Registry
- Large registry analysis comparing BHR to conventional THA in young men
- BHR showed comparable or superior survivorship in selected male cohorts under 65
- Emphasises the importance of patient selection for resurfacing outcomes