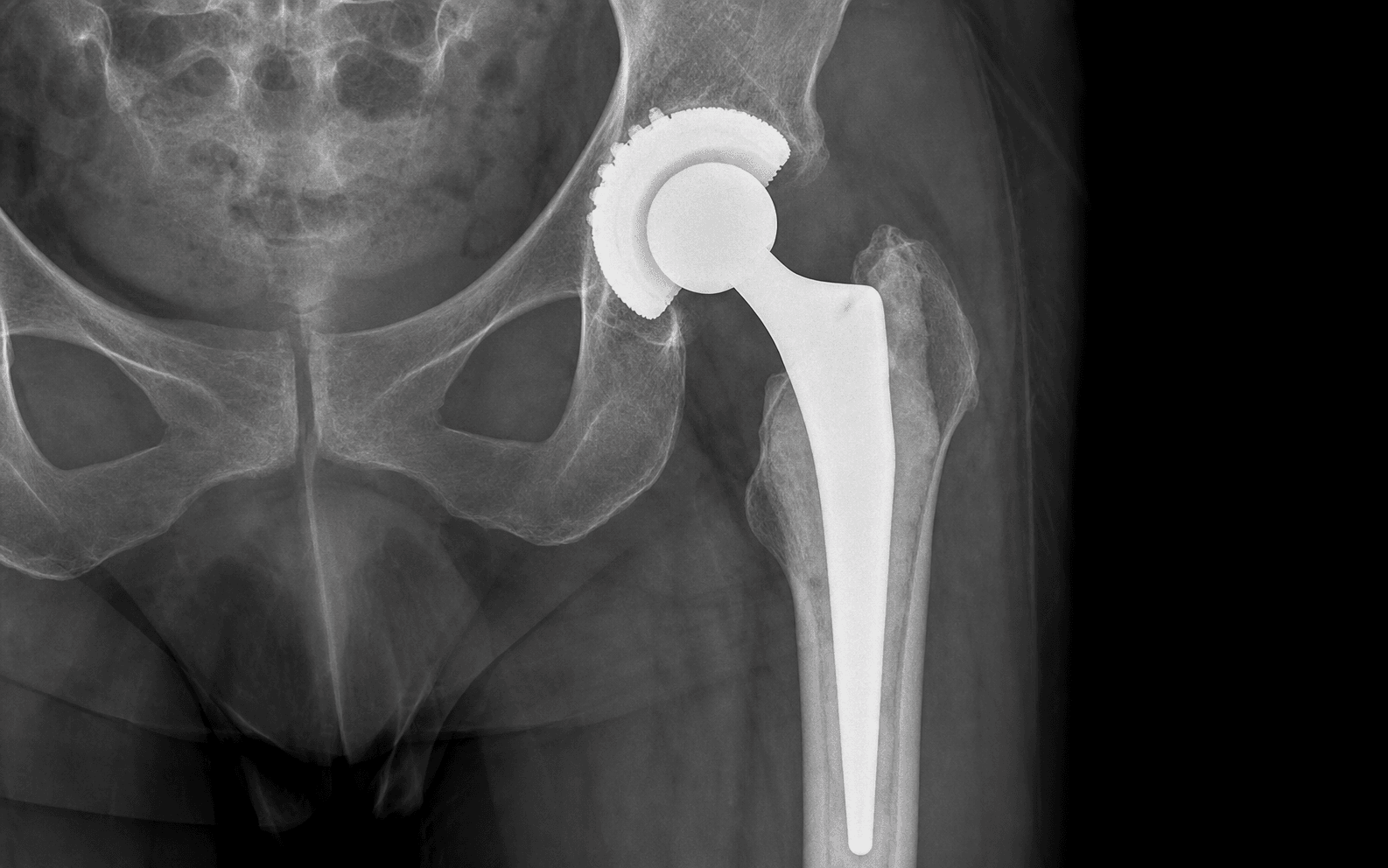
Cemented femoral stem with press-fit acetabular component | advanced
- Hybrid fixation combines the proven long-term survivorship of a cemented femoral stem (greater than 95 percent at 15 years in multiple registries) with the durable biologic fixation of a modern porous-coated uncemented acetabular cup (greater than 98 percent at 10 years).
- Third-generation cementing technique (plug, pulsatile lavage, retrograde pressurised delivery, centraliser) reduces aseptic loosening to less than 3 percent at 15 years; modern cement mantles achieve greater than 2 mm uniform thickness around the stem.
- The posterior approach remains the workhorse for hybrid THA in most centres; key steps include sciatic nerve identification, short-external-rotator and capsular repair, abductor protection and accurate cup version to keep dislocation rate below 2 percent.
- Cement implantation syndrome risk peaks at stem insertion; maintain normovolaemia, use high FiO2, and have vasopressors ready — incidence of significant hypotension is 5 to 10 percent in high-risk patients.
- “Cemented stem longevity in registries exceeds uncemented stems in patients greater than 75 years and in those with Dorr B/C bone; the hybrid construct exploits this while avoiding cemented cup failures seen in older designs.
- “Acetabular screw placement must avoid the anterior quadrants (external iliac vessels) and the sciatic notch; the safe zone is the posterosuperior quadrant with screws less than 25 mm.
- “Leg-length discrepancy greater than 10 mm is the most common cause of patient dissatisfaction and litigation after THA — templating accuracy and intraoperative stability testing are mandatory.
- “Reverse hybrid (uncemented stem, cemented cup) is now rarely performed because modern uncemented cups outperform cemented cups in all age groups in registry data.
When & Why
Indication. Symptomatic end-stage hip osteoarthritis (or inflammatory, post-traumatic or dysplastic arthritis) in a patient whose femoral bone quality favours a cemented stem while the acetabulum is suitable for an uncemented press-fit cup. Hybrid fixation is the registry-preferred construct for the older or osteopenic patient, combining cemented stem reliability with biologic cup fixation. Patient selection favours a hybrid construct when any of the following apply: - Age greater than 70 years with Dorr B or C femoral morphology
- Osteopenic or osteoporotic bone where uncemented stem fixation is unreliable
- Previous femoral osteotomy or deformity favouring a cemented stem
- Surgeon preference grounded in registry-proven cemented stem durability in older patients Absolute indications include a failed previous fixation with significant bone loss requiring cemented reconstruction, a pathological fracture or metastatic disease requiring immediate stable fixation, and neuromuscular conditions with high dislocation risk where a constrained or dual-mobility construct is planned. Relative indications include age 65 to 75 with mixed bone quality, inflammatory arthritis with poor bone stock, and prior radiation to the proximal femur. Contraindications.
- Absolute: active infection; severe acetabular bone deficiency preventing press-fit cup stability; known severe allergy to bone cement or to the antibiotics within it.
- Relative: young active patients (less than 60) with good bone quality — consider fully uncemented; severe cardiopulmonary disease where cement implantation syndrome risk is prohibitive. The one decision that matters — which fixation. Every hybrid THA still begins with the same posterior exposure, neck osteotomy, acetabular and femoral preparation. The defining choice is the fixation strategy:
The best of both: cemented stem longevity in older or osteopenic bone plus biologic cup fixation. Registry-preferred in patients older than 70 and in Dorr B/C femurs.
Preferred under 65 with good bone. Carries higher early periprosthetic fracture and subsidence risk in older patients and Dorr C stovepipe canals.
Reliable stem fixation, but older cemented cup designs suffered late loosening. Modern uncemented cups now outperform cemented cups across all age groups in registry data.
Consent specifically for dislocation (1.5 to 2.5 percent), leg-length discrepancy, cement implantation syndrome, infection (less than 1 percent), nerve injury (less than 1 percent), and the possible need for blood transfusion. Setup & anaesthesia. Lateral decubitus on a radiolucent table with beanbag or pegboard support; the operative leg is draped free and the table must accommodate fluoroscopy. Spinal or general anaesthesia, with an arterial line in high-risk patients. Maintain normovolaemia throughout and have vasopressors (phenylephrine, ephedrine) drawn up and immediately available for cement implantation syndrome. Apply sequential compression devices and give antibiotic prophylaxis (cefazolin 2 g IV, or vancomycin if MRSA risk).
The Operation
The goal: expose the hip through the posterior approach, identify and protect the sciatic nerve, divide the short external rotators and capsule, osteotomise the neck, implant a press-fit uncemented cup with optional posterosuperior screws, then prepare the femur and cement a stem with a third-generation technique — restoring offset, leg length and stability before a meticulous posterior soft-tissue repair. The exposure is laid out in full as the first steps below.
Operative sequence — posterior approach
- Confirm lateral decubitus with the pelvis rigidly fixed so the acetabulum is not pitched during reaming.
- Make a 12 to 15 cm curved incision centred over the greater trochanter, extending proximally along the gluteus maximus fibres and distally along the femoral shaft.
- Divide the fascia lata in line with the skin incision and split the gluteus maximus fibres bluntly in their own direction, protecting the inferior gluteal neurovascular bundle.
- Palpate the sciatic nerve on the posterior surface of the ischium, where it lies 1 to 2 cm posterior to the greater trochanter at the level of the piriformis.
- Place a vessel loop or Penrose drain around it for identification and retract it gently medially; protect it throughout.
- Never place a retractor deep to the nerve on the ischium.
- Tag and divide the short external rotators (piriformis, superior and inferior gemelli, obturator internus, quadratus femoris) close to their insertion on the greater trochanter; divide them close to bone to protect the medial femoral circumflex artery and leave the tendons tagged for later repair.
- Perform a posterior capsulotomy from the acetabular rim to the femoral neck, preserving as much capsule as possible for repair.
- Dislocate the hip by flexing, adducting and internally rotating the leg.
- Perform the femoral neck osteotomy at the pre-planned level using the neck resection guide from the implant system and remove the femoral head.
- Place a curved retractor over the anterior acetabular rim, a posterior retractor on the ischium (clear of the sciatic nerve) and an inferior retractor beneath the transverse acetabular ligament to expose the acetabulum.
- Remove residual labrum and osteophytes and identify the true floor of the acetabulum.
- Ream sequentially with hemispherical reamers, preserving subchondral bone where possible, and under-ream by 1 to 2 mm for press-fit.
- Impact the trial cup to assess stability and position (abduction 40 to 45 degrees, anteversion 15 to 25 degrees), then the definitive porous-coated component.
- If supplemental fixation is needed, add 2 to 3 screws in the posterosuperior quadrant only, each less than 25 mm; confirm extra-pelvic placement by palpation or fluoroscopy. Insert the polyethylene liner.
- Expose the femoral canal by placing the leg in the figure-of-four position and remove residual femoral neck bone.
- Use sequential broaches to prepare the canal, aiming for a minimum 2 mm cement mantle on all sides, and confirm the broach that achieves rotational stability with at least 2 mm clearance for cement.
- Perform a trial reduction to assess leg length, offset and stability.
- Place a cement restrictor plug 2 cm distal to the planned stem tip.
- Perform pulsatile lavage with at least 1 L of saline until the effluent is clear, then dry the canal thoroughly with suction and epinephrine-soaked swabs.
- Inject low-viscosity cement in retrograde fashion with a pressurised gun, maintaining continuous pressure.
- Insert the stem with a centraliser to keep it centred, maintain pressurisation until the cement has hardened, and remove excess cement.
- Reduce the hip and perform stability testing in full flexion, extension and combined positions.
- Confirm leg length (pin or ruler comparison with the contralateral side) and assess offset and abductor tension.
- Irrigate the wound, then repair the posterior capsule and short external rotators to the greater trochanter using heavy non-absorbable sutures; close fascia, subcutaneous tissue and skin in layers and apply a sterile dressing.
Failure to identify the sciatic nerve before posterior capsulotomy risks direct laceration. Aggressive retraction of the nerve against the ischium causes stretch injury, and a retractor placed deep to the nerve on the ischium causes compression. Identify the nerve first, protect it with a vessel loop left in place until final reduction, and never place a retractor deep to it.
Anterior-quadrant screws threaten the external iliac vessels; posteroinferior screws threaten the sciatic nerve and superior gluteal neurovascular bundle. Over-reaming loses press-fit and causes early cup migration, and penetration of the thin (2 to 4 mm) quadrilateral surface causes intrapelvic screw complications. Restrict screws to the posterosuperior quadrant, keep them less than 25 mm, and confirm extra-pelvic placement.
Cement implantation syndrome causes hypotension and desaturation at stem insertion. Inadequate pressurisation produces voids and a Grade C/D mantle. Stem malposition (varus or retroversion) and canal perforation cause early loosement and cement extravasation. Maintain pressurisation continuously and never rush this phase — loss of pressure is the commonest cause of voids.
Identify the sciatic nerve before dividing any capsule, loop it, and leave the loop in place until final reduction. The nerve is most vulnerable during posterior capsulotomy and during acetabular reaming if the posterior retractor slips.
Under-ream by 1 mm for a typical 52 mm cup and confirm a tight press-fit by gentle impaction — never force a cup that is not stable. If supplemental fixation is needed, place two screws in the posterosuperior quadrant, never longer than 25 mm, and always confirm they have not penetrated the quadrilateral surface.
Use a third-generation technique every time: plug, pulsatile lavage until clear, thorough canal drying, retrograde pressurised delivery, and a centraliser. Aim for a uniform mantle greater than 2 mm. Never rush pressurisation — loss of pressure is the commonest cause of voids and early loosening.
Aftercare & Complications
Postoperative protocol | Phase | Timing | Mobilisation & precautions | Therapy & follow-up | |-------|--------|----------------------------|---------------------| | 1 | Day 0 to 2 | Weight-bearing as tolerated from day of surgery with physiotherapy; multimodal analgesia; VTE prophylaxis (enoxaparin 40 mg daily or rivaroxaban 10 mg daily for 28 to 35 days) | Posterior hip precautions started (no flexion greater than 90 degrees, no adduction, no internal rotation) | | 2 | Week 2 to 6 | Wound review at 10 to 14 days; continue precautions | Progressive abductor strengthening and gait normalisation | | 3 | Long-term | Discontinue precautions at 6 weeks if stable; low-impact activities (swimming, cycling, walking) from 3 months | Follow-up and radiographs at 6 weeks, 3 months, 1 year, then annually or biennially; higher-impact activities discussed individually | Complications
- Incidence
- 5 to 10 percent significant hypotension
- Recognition
- Hypotension, desaturation and arrhythmias 1 to 3 minutes after stem insertion
- Prevention and management
- Prevention: pre-emptive volume loading, high FiO2, staged cement insertion, vasopressors ready. Management: stop cementing, support blood pressure with fluids and vasopressors, consider aborting if severe; most cases resolve within 5 to 10 minutes with supportive care
- Incidence
- 1.5 to 2.5 percent posterior approach
- Recognition
- Patient reports a pop or inability to bear weight; leg shortened and internally rotated
- Prevention and management
- Prevention: accurate cup position, posterior capsule repair, offset restoration, intraoperative stability testing. Management: closed reduction under sedation or anaesthesia; revision for recurrent dislocation with component malposition or abductor deficiency
- Incidence
- Greater than 10 mm in 5 to 10 percent
- Recognition
- Patient reports limp, back pain or perceived inequality; measurable on scanogram
- Prevention and management
- Prevention: accurate templating, intraoperative leg-length assessment, offset restoration. Management: shoe lift for discrepancies less than 15 mm; revision for symptomatic discrepancies greater than 20 mm with correctable cause
- Incidence
- Less than 3 percent at 15 years with third-generation technique
- Recognition
- Progressive radiolucent lines greater than 2 mm at the cement-bone interface; stem subsidence or varus migration
- Prevention and management
- Prevention: third-generation cementing with a uniform greater than 2 mm mantle and a centraliser. Management: revision to an uncemented or cemented stem with impaction grafting or distal fixation as indicated
- Incidence
- 0.8 to 1.5 percent
- Recognition
- Intraoperative crack during broaching or stem insertion; postoperative fall with thigh pain
- Prevention and management
- Prevention: careful broaching, avoid aggressive impaction in osteopenic bone. Management: intraoperative cerclage wiring; postoperative Vancouver A or B1 fractures often require revision to a longer stem
- Incidence
- 0.5 to 1.5 percent
- Recognition
- Immediate postoperative foot drop or sensory loss in the sciatic distribution
- Prevention and management
- Prevention: early identification and protection of the nerve throughout the procedure. Management: observation for neurapraxia; exploration and repair if no recovery by 3 to 6 months; ankle-foot orthosis for foot drop
- Incidence
- Less than 1 percent with modern prophylaxis
- Recognition
- Persistent wound drainage, erythema, sinus tract or elevated CRP or ESR beyond 6 weeks
- Prevention and management
- Prevention: perioperative antibiotics, sterile technique, laminar flow. Management: debridement, antibiotics and implant retention (DAIR) for acute infection less than 3 weeks; two-stage revision for chronic infection
Viva & Exam Focus
HYBRIDHYBRID — fixation rationale and registry evidence
CEMENTCEMENT — third-generation technique
Location: lies 1 to 2 cm posterior to the greater trochanter; exits the greater sciatic notch and courses distally along the ischium. Risk: excessive posterior retraction or failure to identify the nerve before posterior capsulotomy causes direct laceration or stretch (incidence 0.5 to 1.5 percent). Prevention: identify early, protect with a vessel loop, and never place a retractor deep to the nerve on the ischium.
Mechanism: monomer toxicity, embolisation of marrow fat and air, and raised intramedullary pressure during pressurised cementing cause acute pulmonary hypertension and right ventricular failure. Presentation: hypotension, desaturation and arrhythmias peak 1 to 3 minutes after stem insertion; mortality in severe cases reaches 0.1 to 0.5 percent. Prevention: pre-emptive volume loading, high FiO2, staged cement insertion and vasopressors ready; avoid over-pressurisation in frail patients.
Quadrant rule: the posterosuperior quadrant is safest; anterosuperior risks the external iliac vessels; posteroinferior risks the sciatic nerve and superior gluteal neurovascular bundle; anteroinferior risks the obturator structures. Safe practice: limit screw length to less than 25 mm, confirm extra-pelvic placement by fluoroscopy or palpation, and never place screws in the anterior quadrants.
Threshold: greater than 10 mm perceived discrepancy causes limp, back pain and dissatisfaction; greater than 20 mm often leads to litigation. Intraoperative assessment: shuck test, leg tension and comparison with the contralateral leg before final reduction; templating must account for offset and neck-cut level. Prevention: restore native offset and centre of rotation, document intraoperative leg length, and counsel that perfect equality is not always achievable.
Patient factors: prior hip surgery, neuromuscular disease, cognitive impairment and abductor deficiency increase dislocation risk 2 to 4 fold. Surgical factors: cup malposition (greater than 50 degrees abduction or greater than 30 degrees anteversion), inadequate capsular repair and leg-length change are modifiable. Prevention: stability testing in all positions, posterior capsule and external-rotator repair, and dual-mobility or constrained liners in high-risk patients.
Barrack grading: Grade A (complete white-out) and B (slight radiolucency) predict excellent fixation; Grade C (voids greater than 50 percent) and D (gross deficiencies) correlate with early loosening. Technique failure: poor preparation, lavage or pressurisation produces Grade C or D mantles and increases revision risk 3 to 5 fold at 10 years. Prevention: pulsatile lavage, canal drying, pressurised retrograde filling and a centraliser produce greater than 95 percent Grade A or B mantles in modern series.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 78-year-old woman with Dorr C femoral morphology and severe osteoarthritis presents for elective THA. She has a history of hypertension and mild COPD. Discuss your choice of fixation and the specific anaesthetic precautions you would take.”
“You are planning a hybrid THA via the posterior approach. The patient is a 72-year-old man with a previous lumbar fusion and abductor weakness. How do you modify your technique to minimise dislocation risk?”
“A 68-year-old man undergoes hybrid THA. On the first postoperative radiograph the cemented stem appears in 5 degrees of varus with a cement mantle that is less than 2 mm laterally. How do you counsel the patient and what is the expected outcome?”
Indications
- Age greater than 70 or Dorr B or C femur — cemented stem survivorship greater than 95 percent at 15 years
- Osteopenic bone where uncemented stem fixation is unreliable
- Previous femoral deformity or osteotomy favouring cemented reconstruction
- Avoid in active infection, severe acetabular deficiency or young patients with excellent bone quality
Fixation rationale
- Cemented stem: third-generation technique (plug, lavage, pressurisation, centraliser) produces a greater than 2 mm uniform mantle and less than 3 percent loosening at 15 years
- Uncemented cup: porous-coated press-fit with optional posterosuperior screws less than 25 mm; greater than 98 percent osseointegration at 10 years
- Reverse hybrid (uncemented stem plus cemented cup) is obsolete — modern uncemented cups outperform cemented cups in all age groups
- Hybrid exploits the best of both: cemented stem reliability in older or osteopenic bone plus biologic cup fixation
Posterior approach key steps
- Identify and protect the sciatic nerve early — vessel loop before posterior capsulotomy
- Divide short external rotators close to insertion; tag for repair
- Acetabular preparation: under-ream 1 to 2 mm, confirm press-fit, screws only in the posterosuperior quadrant
- Femoral canal: sequential broaching for a minimum 2 mm cement mantle on all sides
- Third-generation cementing: plug 2 cm distal to stem tip, pulsatile lavage, retrograde pressurised delivery, centraliser
- Posterior capsule and external-rotator repair reduces dislocation from 3 percent to 1 percent
Danger zones
- Sciatic nerve: 1 to 2 cm posterior to the greater trochanter — identify before capsulotomy
- Acetabular screws: anterior quadrant risks external iliac vessels; posteroinferior risks the sciatic nerve
- Cement implantation syndrome: hypotension at stem insertion — arterial line, volume loading, high FiO2, vasopressors ready
- Leg-length discrepancy greater than 10 mm: dissatisfaction and litigation — templating and intraoperative assessment mandatory
Complications
- Cement implantation syndrome: 5 to 10 percent significant hypotension; supportive care resolves most cases
- Dislocation: 1.5 to 2.5 percent; posterior capsule repair reduces risk by 60 percent
- Aseptic loosening: less than 3 percent at 15 years with third-generation technique; Grade C mantle triples risk
- Leg-length discrepancy: greater than 10 mm in 5 to 10 percent; shoe lift for less than 15 mm
- Sciatic nerve injury: 0.5 to 1.5 percent; early identification and protection are key
Registry outcomes
- AOANJRR: hybrid 96.8 percent survival at 10 years in patients older than 70
- NJR: greater than 94 percent survival at 15 years with third-generation cementing
- Cemented stem revision for loosening less than 2 percent at 15 years with modern technique
- Uncemented cup revision for loosening less than 1 percent at 10 years
Postoperative protocol
- Weight-bearing as tolerated from day of surgery
- VTE prophylaxis 28 to 35 days (enoxaparin or rivaroxaban)
- Hip precautions 6 weeks (posterior approach)
- Follow-up radiographs at 6 weeks, 1 year, then annually or biennially
Background & Evidence
Why hybrid fixation works. Hybrid constructs combine the strengths of each fixation mode. Cemented stems maintain greater than 95 percent survival at 15 years in patients older than 75, while modern porous-coated cups achieve greater than 98 percent osseointegration at 10 years across all age groups. The combination avoids the higher early revision rates seen with fully uncemented stems in older patients and the late cup loosening seen with older cemented cup designs.
- Hybrid (cemented stem plus uncemented cup)
- 3.2 percent
- Fully uncemented
- 4.1 percent
- Fully cemented
- 5.8 percent
- Hybrid (cemented stem plus uncemented cup)
- Greater than 95 percent
- Fully uncemented
- 91 to 93 percent
- Fully cemented
- Greater than 96 percent
- Hybrid (cemented stem plus uncemented cup)
- Less than 1 percent
- Fully uncemented
- Less than 1 percent
- Fully cemented
- 3 to 5 percent (older designs)
- Hybrid (cemented stem plus uncemented cup)
- 1.5 to 2.5 percent
- Fully uncemented
- 1.8 to 3.0 percent
- Fully cemented
- 2.0 to 3.5 percent
- Hybrid (cemented stem plus uncemented cup)
- 0.8 percent
- Fully uncemented
- 1.5 to 2.5 percent
- Fully cemented
- 0.4 percent
- Hybrid (cemented stem plus uncemented cup)
- Greater than 70 years
- Fully uncemented
- Less than 65 years
- Fully cemented
- Greater than 80 years
Surgical anatomy.
- Acetabulum: a hemispherical socket formed by ilium, ischium and pubis. The posterior wall is thicker and is the primary buttress for cup fixation; the posterosuperior quadrant is the safest zone for screws. The anterior wall is thin and lies immediately posterior to the external iliac vessels. The quadrilateral surface is thin (2 to 4 mm) and must not be penetrated.
- Proximal femur: the neck-shaft angle averages 125 to 135 degrees. The calcar femorale is a dense cortical strut on the medial neck that supports the cemented stem. Dorr classification grades canal morphology — Type A (champagne flute, thick cortices), Type B (intermediate), Type C (stovepipe, thin cortices). Hybrid THA is particularly indicated for Dorr B and C femurs.
- Sciatic nerve: exits the pelvis through the greater sciatic notch, passes posterior to the acetabulum and courses distally along the ischium; in the posterior approach it lies 1 to 2 cm posterior to the greater trochanter at the level of the piriformis.
- Blood supply: the medial femoral circumflex artery is the primary supply to the femoral head and must be preserved during capsular exposure; the superior gluteal artery exits the greater sciatic notch to supply the abductors, and travels there with the sciatic nerve.
- Safe intervals: the posterior approach works the interval between gluteus maximus (inferior gluteal nerve) and the abductors (superior gluteal nerve); the short external rotators are divided close to their insertion to protect the medial femoral circumflex artery and allow later repair. Global registry outcomes and practice. AOANJRR 2023 data show 96.8 percent survival at 10 years for hybrid constructs in patients older than 70, and NJR data confirm greater than 94 percent survival at 15 years with third-generation cementing. The hybrid combination is particularly effective in older patients with poor bone quality, where fully uncemented stems carry higher early revision risk for fracture and subsidence. Global guidelines (AAOS, NICE, BOA-BOAST, EFORT) support hybrid fixation in appropriately selected patients; cemented stems remain the preferred option in patients older than 75 or with Dorr C femurs in most national registries, and modern porous-coated cups have largely replaced cemented acetabular components because of superior long-term fixation.
References
Cemented or uncemented acetabular fixation in combination with the Exeter Universal cemented stem
- Uncemented acetabular components combined with cemented Exeter stem demonstrated good long-term survivorship supporting the hybrid construct
Fixation, sex, and age: highest risk of revision for uncemented stems in elderly women
- Uncemented stems carried the highest revision risk in elderly women supporting preference for cemented stems or hybrid in this demographic
Perioperative, short-, and long-term mortality related to fixation in primary total hip arthroplasty
- No difference in mortality between cemented, uncemented and hybrid fixation in a large Norwegian registry cohort of 79,557 patients
Increasing but levelling out risk of revision due to infection after total hip arthroplasty
- Hybrid fixation showed infection revision rates comparable to other fixation types in over 108,000 primary THAs
Hybrid versus uncemented total hip arthroplasty: a registry-based comparison
- Hybrid fixation showed lower revision rates than fully uncemented THA in patients older than 70 years at 10 years
- Cemented stem with uncemented cup achieved 96.8 percent survival at 10 years versus 95.9 percent for uncemented constructs
- The difference was driven by reduced early periprosthetic fracture and stem subsidence in the hybrid group
Cemented versus uncemented hemiarthroplasty for hip fracture: a meta-analysis
- Cemented stems demonstrated lower revision rates and fewer periprosthetic fractures compared with uncemented stems in older patients
- Cement implantation syndrome occurred in 5 to 8 percent of cemented cases but was rarely fatal with modern anaesthetic management
- Functional outcomes were equivalent at 1 year
Long-term outcomes of hybrid total hip arthroplasty in the National Joint Registry
- Hybrid THA survival at 15 years exceeded 94 percent in patients aged 70 to 80 at index surgery
- Aseptic loosening of the cemented stem accounted for only 1.8 percent of revisions at 15 years with third-generation technique
- Cup revision for loosening or wear was less than 1 percent at 10 years with modern porous-coated components
Effect of cementing technique on long-term stem survival: a systematic review
- Third-generation techniques (plug, lavage, pressurisation, centraliser) reduced stem revision for loosening by 60 to 70 percent compared with first-generation methods
- Uniform cement mantle greater than 2 mm on all sides was the strongest predictor of long-term survival
- Centralisers improved stem position and reduced Grade C or D mantles from 25 percent to less than 5 percent
Dislocation rates after posterior approach THA with and without capsular repair
- Posterior capsular and external rotator repair reduced dislocation rate from 3.2 percent to 1.1 percent in a consecutive series of 2,500 posterior THAs
- Repair added 8 to 12 minutes to operative time with no increase in infection or nerve injury
- Patients with repair had higher satisfaction and lower revision rates for instability