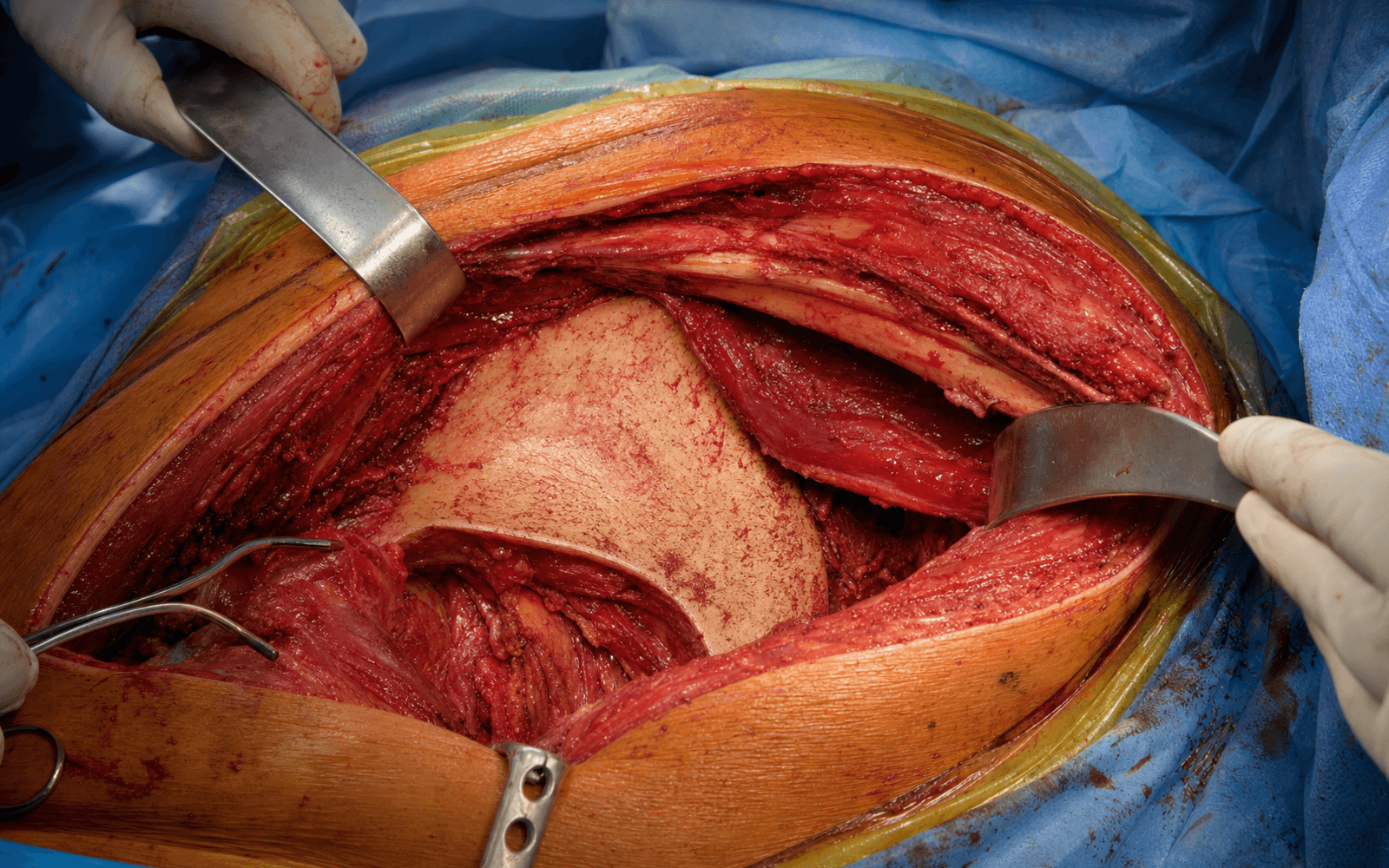
Iliac crest incision | subperiosteal iliacus elevation | LFCN protected at the ASIS | pelvic brim and anterior SI joint exposure
- Incision runs along the iliac crest from 2 cm posterior to the ASIS toward the PSIS, typically 10 to 15 cm for a standard window.
- The lateral femoral cutaneous nerve (LFCN) runs within 1 to 3 cm of the ASIS in most patients and is the structure most often injured - identify and protect it before any medial retraction.
- All inner-table dissection is strictly subperiosteal - elevate iliacus from the inner table down to the pelvic brim to preserve its vascularity.
- The external iliac vessels lie on the pelvic brim deep to the iliacus - use only broad malleable retractors, never pointed retractors placed blindly.
- The iliac window alone cannot reach the low anterior column, pubic rami or quadrilateral surface - extend to the middle or medial window (or a Stoppa) when these are involved.
When & Why
What it exposes. The iliac (lateral window) approach gives direct access to the internal iliac fossa, the inner and outer tables of the iliac wing, the pelvic brim and the anterior aspect of the sacroiliac (SI) joint. It is the lateral limb of the classic ilioinguinal approach and reaches the pelvic brim, but it does not extend safely below the iliopectineal eminence without adding the middle or medial window. When to use it. Indications are isolated iliac wing fractures, high anterior column acetabular fractures (fracture line exiting above the iliopectineal eminence), limited anterior SI joint access, iliac crest bone graft harvest, and the high fragment of both-column fractures. As a stand-alone exposure it avoids the morbidity of a full three-window ilioinguinal approach. Position & landmarks. Most often supine on a radiolucent table with an ipsilateral buttock bump (20 to 30 degrees elevation) for anterior-column work, or lateral decubitus (affected side up) when outer-table or abductor elevation is planned; arms are tucked or abducted less than 90 degrees with padding. Before draping, confirm the C-arm can obtain AP, obturator oblique and iliac oblique (Judet) views without repositioning. Palpate and mark the ASIS (the incision starts 2 cm posterior to it along the crest), the iliac crest to the PSIS, the pubic tubercle (medial extent if extending into the ilioinguinal) and the greater trochanter (reference for the lateral position). Approach variants.
- What it exposes
- Crest to ASIS, inner table only
- Typical use
- Iliac wing ORIF
- What it exposes
- Inner table plus outer-table abductor elevation
- Typical use
- Combined column access
- What it exposes
- Lateral limb of the full three-window approach
- Typical use
- Acetabular reconstruction
The Exposure
There is no true internervous plane superficially - the approach passes through subcutaneous fat and the fascia over the crest, which is incised directly on bone, leaving a cuff for repair. The deep dissection is strictly subperiosteal: on the inner table the plane is between iliacus (femoral nerve) medially and crest periosteum; on the outer table, when required, a genuine internervous plane exists between tensor fascia lata (superior gluteal nerve) anteriorly and gluteus medius (superior gluteal nerve) posteriorly.
Exposure sequence
- Begin 2 cm posterior to the ASIS along the iliac crest and extend posteriorly along the crest as far as the PSIS or as the fracture dictates (typically 10 to 15 cm for a standard iliac window).
- Divide skin and subcutaneous fat, then identify the lateral femoral cutaneous nerve as it crosses or passes medial to the ASIS (within 1 to 3 cm in most patients).
- Tag it with a vessel loop before any medial retraction.
- Incise the fascia directly on the iliac crest, leaving a 3 to 5 mm cuff on both the inner and outer lips for later repair, and tag the fascial edges.
- With a Cobb elevator, develop the subperiosteal plane on the inner table and elevate iliacus medially and inferiorly toward the pelvic brim.
- Continue the subperiosteal dissection to expose the entire iliac fossa and the anterior aspect of the sacroiliac joint.
- Place pointed Hohmann retractors on the pelvic brim under direct vision, avoiding the iliac vessels, and irrigate frequently to visualise the psoas tendon and iliopectineal eminence.
- Only if full wing exposure or posterior access is needed, elevate gluteus medius and minimus subperiosteally from the outer table.
- Limit distal dissection to protect the superior gluteal neurovascular bundle (the nerve enters gluteus medius about 5 cm above the greater trochanter), and expose the greater sciatic notch only if posterior column or posterior SI access is required.
- Reduce the fracture with pointed reduction clamps, Schanz pins in the crest, or pelvic reduction forceps.
- Fix with 3.5 mm reconstruction plates contoured along the iliac crest or pelvic brim, using lag screws from crest to brim for simple patterns.
- Confirm reduction with direct vision and fluoroscopy (AP, obturator and iliac oblique Judet views).
The lateral femoral cutaneous nerve is the structure most often injured in this approach - it crosses the iliac crest or passes within 1 to 3 cm of the ASIS in most patients, and injury (causing painful meralgia paraesthetica) occurs in up to 30 percent of cases. Document pre-operative sensation, incise the fascia 2 cm posterior to the ASIS, identify and loop the nerve before any medial retraction, never use self-retaining retractors that compress it against the ASIS, and re-document sensation post-operatively.
All inner-table dissection stays on bone until the pelvic brim is reached. Elevating iliacus without its periosteum devascularises the muscle, promoting fatty atrophy and heterotopic ossification. The same principle protects the iliac vessels lying immediately deep on the brim - keep broad malleable retractors under direct vision and never place a pointed retractor blindly.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Lateral femoral cutaneous nerve (1 to 3 cm medial to or over the ASIS; injury 10 to 30 percent)
- Protection
- Incise 2 cm posterior to ASIS; identify and loop; no self-retainers on the nerve
- Structure at risk
- Superficial circumflex iliac artery crossing the ASIS region
- Protection
- Coagulate or ligate if encountered
- Structure at risk
- Iliacus - devascularisation if not elevated subperiosteally (fatty atrophy, heterotopic ossification)
- Protection
- Strict subperiosteal elevation with a Cobb elevator
- Structure at risk
- Tensor fascia lata origin (must be repaired if detached)
- Protection
- Leave a fascial cuff on the outer lip and reattach at closure
- Structure at risk
- External iliac vessels on the pelvic brim
- Protection
- Broad malleable retractors only, under direct vision; never pointed retractors placed blindly
- Structure at risk
- Superior gluteal artery and nerve exiting the greater sciatic notch 2 to 3 cm posterior to the posterior crest
- Protection
- Limit outer-table dissection and stay proximal on the crest
- Structure at risk
- Iliohypogastric and ilioinguinal nerves (if extending medially)
- Protection
- Careful medial extension with protection on approach
- Structure at risk
- Femoral nerve on iliopsoas (medial-retraction neuropraxia)
- Protection
- Gentle, periodic medial retraction only
- Structure at risk
- Corona mortis behind the superior pubic ramus (if extending medially)
- Protection
- Anticipate and control when extending toward the Stoppa or medial window
Extensile options. Extend posteriorly along the crest toward the PSIS for more posterior iliac-wing or SI-joint access, and the window can be connected to the Kocher-Langenbeck (posterior) approach for combined anterior-posterior column fractures. Extend distally and medially along the inguinal ligament to convert into the full ilioinguinal approach (middle and medial windows), or use the Stoppa (anterior intrapelvic) approach for the quadrilateral surface and low anterior column. Closure. Reattach iliacus and the abdominal obliques to the inner lip of the crest using heavy non-absorbable suture through drill holes (or over a bone bridge), repair the tensor fascia lata and gluteal fascia to the outer lip, close subcutaneous tissue in layers, place a suction drain in the iliac fossa for extensive dissection, and use hip-flexion precautions for 4 to 6 weeks to protect the repair.
Procedures Through This Approach
- ORIF of isolated iliac wing fractures.
- High anterior column acetabular fractures (fracture line above the iliopectineal eminence).
- Anterior SI joint plating or screw fixation.
- Iliac crest bone graft harvest (tricortical strut or cancellous).
- Limited exposure for anterior column screw placement in both-column fractures.
Viva & Exam Focus
ILIACILIAC — the lateral window
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old male sustains a high-energy anterior column acetabular fracture with a large iliac wing fragment. The fracture line exits above the iliopectineal eminence. Which approach would you use and why?”
“During an iliac window approach the LFCN is not identified before deep dissection. The patient wakes with severe burning pain and numbness on the lateral thigh. What went wrong and how could it have been prevented?”
“You are planning fixation of a both-column acetabular fracture. The iliac wing fragment is large and the anterior column fracture exits high. Which windows of the ilioinguinal approach will you use and why?”
Positioning
- Supine with an ipsilateral buttock bump (20 to 30 degrees) - standard
- Lateral decubitus - when outer-table or abductor work is required
- C-arm access for AP, obturator oblique and iliac oblique views confirmed before draping
Key landmarks
- ASIS - the incision starts 2 cm posterior along the crest
- Iliac crest from ASIS to PSIS - palpable throughout
- Pelvic brim - the terminal point of inner-table dissection
Critical dangers
- LFCN - identify within 1 to 3 cm of the ASIS, protect with a vessel loop (injury 10 to 30 percent)
- External iliac vessels - broad malleable retractors only at the brim
- Superior gluteal neurovascular bundle - limit outer-table dissection (nerve 5 cm above the trochanter)
Internervous plane
- Inner table: subperiosteal (no true plane)
- Outer table: between TFL (superior gluteal) and gluteus medius (superior gluteal)
- Limit distal outer-table exposure to protect the superior gluteal nerve
Procedures accessible
- Iliac wing ORIF
- High anterior column acetabulum (above the iliopectineal eminence)
- Anterior SI joint access
- Iliac crest bone graft harvest
Closure principles
- Drill holes in the crest for heavy suture repair of iliacus and abdominal muscles
- Repair TFL and gluteal fascia to the outer lip
- Suction drain in the iliac fossa for extensive cases
- Hip-flexion precautions for 4 to 6 weeks post-operatively
References
Anatomical considerations of the internal iliac artery in association with the ilioinguinal approach for anterior acetabular fracture fixation
- Anatomical study detailing the course of the internal iliac artery and its branches relative to the ilioinguinal approach windows
Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury
- Large series demonstrating the importance of accurate reduction via anterior approaches including the iliac window for optimal outcomes in acetabular fractures
Screw fixation of acetabular fractures
- Technical description of screw placement through the iliac window for anterior column and iliac wing fixation
Results of 75 consecutive patients with an acetabular fracture
- Early clinical series using the ilioinguinal approach with iliac window component showing reduction quality and complication rates